Page: /
Page Synopsis: You don't have to read this entire page! It is meant to show you the many tests doctors could be doing but either aren't, or are misreading (low range as acceptable, for instance) as well as the tests that will help pinpoint your specific issues.
Print it out and have your doctor or practitioner read it. Items that have genuinely helped patients are further in the report (so don't get discouraged)
Skill Level 5
Relevance:5 Technical Level:5
Though this page has a high relevance, it can be skimmed
Testing and Detect https://bra.in/2qzAEb, https://bra.in/8pxNE6,
1) Hormone testing
2) Chronic Infections testing
Testing Infectious Causes of ME/CFS and Fibromyalgia ***
2a) Mycoplasma Testing
3) parasite test and cleanse test Ova, Cysts and Parasites
3a) Parasitic Examination, Stool https://www.labtestsonline.org.au/learning/test-index/o-and-p-or-ocp
4) Heavy Metal Testing heavy metals panel or heavy metal toxicity test Comprehensive Urine Element Profile
https://www.drmyhill.co.uk/wiki
5) Lab tests
5a) Calcium Channels
user Issie on healthrising forum 'I have mutations on TRMP3. I find Tramadol and GastroCrom to be two of my best helps. Both have mild calcium channel blocker effects. They dilate vessels. I also find using a Bentyl (muscle relaxer), with them to make the combination better. I’m not healed, but this does keep me more functional. I do believe these meds have other properties that help. Tramadol works on all the neurotransmitters. Some sort of tweak there helps. (I use a quarter of RXd amount and cycle on and off this. When it stops helping, I go off a few weeks to reset a lower dose to work.) GastroCrom is also a mast cell stablizer and that helps MCAS. Also using enzymes to help blood flow and thin blood'
user Anke on healthrising forum 'the last time I tried a calcium blocker I swelled up with oedema and we had to stop'
6) Scanning Imaging
6a) MRIst scan testing
6a i) R2t* Signal Testing, Testing for amount and kind of brain cells by evaluating R2t* signal from MRI scan
6b) Diffusion Tensor Imaging
6 2) 'Role of Imaging' Oxford Textbook of Neurorehabilitation 2nd Edition
The role of neuroimaging in understanding the impact of neuroplasticity after CNS damage
6c) Grayfield method microscopy
6 3) High-speed 3D microscope
New technology could make biopsies a thing of the past, High-speed 3D microscope can see real-time cellular detail in living tissues to guide surgery, speed up tissue analyses, and improve treatments
6c) SPECT scan
'A SPECT scan showed that I had significantly impaired bloodflow to the brain' list of my current CFS symptoms
https://livingwithchronicfatiguesyndrome.wordpress.com/page/10
Our brain imaging diagnostic tool called SPECT (Single Photon Emission Computed Tomography) accurately identify underlying brain issues that can contribute to symptoms.
Address 350 N. Wiget Lane, Suite 105
Walnut Creek, CA 94598
Phone
650-416-7830
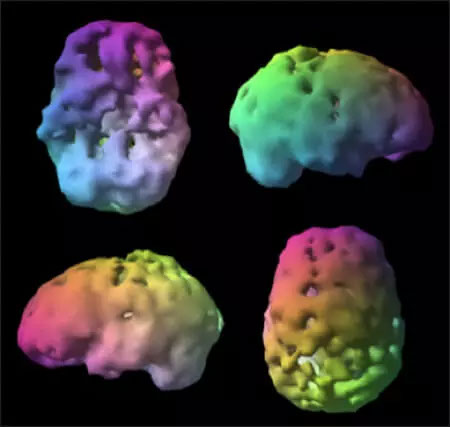 Unhealthy SPECT Brain Scan
Unhealthy SPECT Brain Scan
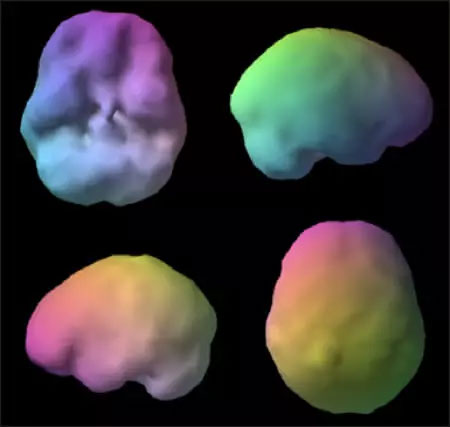 healthy SPECT Brain Scan
healthy SPECT Brain Scan
7) allergens tested
7a) food allergens tested
8) Blood flow and heart valves
9) Other biomarkers
10) CD4 T-lymphocyte count
11) Somnogen in Cerebrospinal Spinal Fluid of Hypersomnia Patients, and (Endogenous) Enhancement of GABAA Receptors
Overview
Brain injury or trauma causes immune system suppression. Infection is a serious consequence of these events and is present in both open and closed TBI, mTBI, and with stroke. CD4 T-lymphocyte count may be a marker to determine emergence of infection after brain trauma, including stroke 'The Injured Brain: TBI, mTBI, the Immune System, and Infection: Connecting the Dots'
Which tests can be done for free at Kaiser, and how are they interpreted? According to Dr Myhill "Most patients, by the time they get to see me, have had all the routine tests done. These tests just test for macroscopic pathology such as major organ failure (anaemia, heart disease, cancer, liver failure, kidney failure and some gut problems). They do not test for minor organ failures (such as partial thyroid gland failure, partial adrenal gland failure, mild liver damage, poor ability to detox). None of these tests look for poor function of the brain or brain damage, nutritional tests are often absent or limited, hormone tests are usually incomplete and there are virtually no tests of micropathological function.
Having said that, there are often mild abnormalities in standard tests which have not been picked up on by the GP or consultant, but which are clinically important for the CFS sufferer. Results are given by a figure and there should also be a reference range next to this figure – that tells you if you are inside or outside the reference range. This reference range often varies from one lab to another
Most patients, by the time they get to see me, have had all the routine tests done. These tests just test for macroscopic pathology such as major organ failure (anemia, heart disease, cancer, liver failure, kidney failure and some gut problems). They do not test for minor organ failures (such as partial thyroid gland failure, partial adrenal gland failure, mild liver damage, poor ability to detox). None of these tests look for poor function of the brain or brain damage, nutritional tests are often absent or limited, hormone tests are usually incomplete and there are virtually no tests of micropathological function.
Having said that, there are often mild abnormalities in standard tests which have not been picked up on by the GP or consultant, but which are clinically important for the CFS sufferer. Results are given by a figure and there should also be a reference range next to this figure – that tells you if you are inside or outside the reference range. This reference range often varies from one lab to another"
Joined selfhacked and they analyze uploaded tests
1) Test Adrenal Stress Profile (salivary)
Laboratory Genova Diagnostics
Price £90.00
Sample required Saliva sample
https://www.drmyhill.co.uk/wiki/Adrenal_stress_profile_-_salivary
This test measures levels of cortisol and DHEA-s in 4 samples of saliva collected over 24 hours to assess body levels of both hormones.
1b) For primary adrenal insufficiency: Check adrenal cortex antibodies and steroid 21-hydroxylase abs
2) Amylase
Laboratory TDL
Price £50.00
Sample required blood
https://www.drmyhill.co.uk/wiki/Amylase
This test measures the level of the enzyme amylase in the blood serum. This enzyme is specific to the pancreas and raised levels suggest damage to the pancreas as in acute and chronic pancreatitis. I would usually do this test along with liver function tests. Another useful test for the pancreas is faecal elastase
3) Test Antioxidant status profile
Laboratory Biolab
Price £145.00
Sample required blood
https://www.drmyhill.co.uk/wiki/Antioxidant_status_profile
This profile measures levels of the front line antioxidant molecules in cells and mitochondria, i.e. Co-enzyme Q10, red cell glutathione and two enzymes: superoxide dismutase (SODase) and glutathione peroxidase.
Co-enzyme Q10 is the most important antioxidant inside mitochondria and also a vital molecule in oxidative phosphorylation (energy production in cells). A deficiency of Co Q10 can be corrected with supplementation.
Superoxide dismutase (SODase) is the most important superoxide (free radical) scavenger in muscles. Deficiency can explain muscle pain and easy fatigue-ability in some patients. SODase is dependent on correct levels of copper, manganese and zinc and therefore checking levels gives clear indications for supplementation with appropriate doses of these minerals.
Glutathione peroxidase requires glutathione and selenium for its synthesis. Again, as a functional test of these two important antioxidants, the glutathione peroxidase result gives indications for addressing deficiencies of these two nutrients
4) Test B vitamins - functional blood profile
Laboratory Biolab Medical Unit
Price £96.00
Sample required blood
https://www.drmyhill.co.uk/wiki/B_vitamins_-_functional_blood_profile
This test measures levels of vitamins B1, B2 and B6. These are common deficiencies and I do not often do this test because I recommend taking B vitamins routinely
5) Test B12 (active) vitamin levels
Laboratory TDL
Price £45.50
Sample required blood
https://www.drmyhill.co.uk/wiki/B12_vitamin_levels
The test measures levels of vitamin B12 in serum.
I do not usually recommend checking B12 levels in chronic fatigue syndrome patients because in most cases they benefit from B12 by injection even if the levels are "normal" (see B12 - rationale for using vitamin B12 in CFS). However, it is worth checking levels in someone who does not have CFS, but who wants to make sure that all his systems are functioning at the optimum level. This would be a useful test as part of a disease prevention screen. (See Disease prevention).
I would also prescribe B12, regardless of serum levels, in anyone with poor antioxidant status
6) Test Carbonic anhydrase studies in red blood cells
Laboratory TEST NO LONGER AVAILABLE
Price £41.00
Sample required blood
https://www.drmyhill.co.uk/wiki/Carbonic_anhydrase_studies_in_red_blood_cells
Hyperventilation is a difficult diagnosis to make clinically and that is why having an objective test of hyperventilation is so useful. People who hyperventilate deplete their levels of red cell carbonic anhydrase and the ratio between the activity and the protein gives us a good indication of whether or not hyperventilation is a problem.
Hyperventilation is also difficult to treat and so this test tells us how much effort we have to put in to correcting this. Essentially, there is a two-pronged approach - firstly biochemical and secondly physical:
Biochemically, red cell carbonic anhydrase is a zinc dependent enzyme and will be depleted simply by zinc deficiency.
Furthermore, a low red cell carbonic anhydrase drives hyperventilation and so this is another example of one of the many vicious cycles seen in patients with chronic fatigue. Zinc is best absorbed at night and I recommend taking 30mg last thing at night on an empty stomach. This should be in addition to zinc taken in my physiological mix of minerals, Mineral Mix. Please see Multi Mineral Mix I now also supply Sunshine Salt. Please see Online Sales shop link for Sunshine Salt Sunshine Salt can be used instead of Multi Mineral Mix MMM and can be used instead of salt for cooking and on the table. Sunshine salt contains the top twelve essential minerals, vital for good health but lacking in modern Western diets. Adults should consume one rounded teaspoonful daily, less for children according to weight. Please also see my book The PK Cookbook - Go Paleo-ketogenic and get the best of both worlds for more detail on Sunshine Salt.
Low magnesium often drives hyperventilation and again magnesium is present in my physiological mix of minerals in adequate amounts. Absorption of magnesium is enhanced by vitamin D, hence the need to continue with vitamin D supplements or ideally sunshine. I like all my patients to take 2,000 i.u. of vitamin D or get a good half-hour's sunshine daily.
Low potassium is also common in hyperventilation; furthermore in the short-term hyperventilation results in a respiratory acidosis and such pH changes may well be responsible for many of the peculiar symptoms seen in hyperventilation. I recommend using potassium bicarbonate as Sando-K, 1 tablet twice daily to help redress the pH balance - this is available on prescription as Sando-K.
We now come to the physical interventions. What seems to go wrong in hyperventilation is that the respiratory centre appears to be set incorrectly and this of course partly explains why hyperventilation continues throughout sleep. The idea is to use breathing exercises to consciously reduce and slow the rate of ventilation thereby increasing carbon dioxide retention. Initially the respiratory centre rails against this and tries to make the sufferer breathe more, but this is what must be resisted. If this is done consciously for long enough then eventually the respiratory centre readjusts to tolerate a higher degree of CO2 retention. There are many ways in which this technique can be learned - the best known is probably the Buteyko method and there are many practitioners trained to undertake breathing retraining. There are also some physiotherapists who are interested in hyperventilation and a list of therapists is available from Ann Pitman from the Physio-Hyperventilation interest group. The address is www.physiohypervent.org - click here Physiotherapy for Hyperventilation There is also an e-mail address for Ann Pitman [email protected]. She produces audios which help greatly for DIY treatment.
I suspect hyperventilation is a much more common problem than actually realised and I have to say that the tests that I have been doing so far confirm thi
7) Test Co-enzyme Q10
Laboratory Biolab Medical Unit
Price £64.00
Sample required blood
https://www.drmyhill.co.uk/wiki/Co-enzyme_Q10
Co-enzyme Q 10 is a co-factor on which depend some vitally important mitochondrial enzymes involved in the production of both ATP and therefore also energy. This affects every cell in the body. It is the most important electron donor and receiver in Krebs citric acid cycle, which is fundamental to all life forms. This makes it a vital molecule in oxidative phosphorylation. It is also the most important antioxidant inside mitochondria and plays a signficant role in situations of oxidative stress
8) Coeliac disease (gluten allergy) test - Gliadin antibodies
Laboratory TDL
Price £ASK THE OFFICE
Sample required blood
https://www.drmyhill.co.uk/wiki/Coeliac_disease_(gluten_allergy)_test_-_Gliadin_antibodies
his test measures antibody levels to a wheat protein (gluten) in the blood serum.
This is an important diagnosis, partly because coeliac is a risk factor for gut lymphoma and avoidance of gluten is essential and partly because this should entitle you to prescriptions for gluten free products.
Just because this test is negative does not mean you are not allergic to wheat. There are many different antigens in wheat - gluten is just one of them. Other tests which could be useful include:
- Endomysial Antibodies
- Reticulin Antibodies
- All three tests (Gliadin A/Bs, Reticulin A/Bs, Endomysial A/Bs and also Tissue Transglutaminase) have been combined into a Gluten Sensitivity Evaluation Profile
9) Comprehensive Digestive Stool Analysis
Test Comprehensive Digestive Stool Analysis
Laboratory Genova Diagnostics
Price £175.00
Sample required stool
https://www.drmyhill.co.uk/wiki/Comprehensive_Digestive_Stool_Analysis
The test gives an idea of how well foods are digested and absorbed, gives some products of gut fermentation, looks for blood in the stool, gives counts of bacteria and yeast, identifies those bacteria which should not be there and gives a list of antibiotic and anti-fungal preparations, both herbal and drug, to which that micro-organism is sensitive. N.B. If this test is requested as a second or subsequent test on an order, please contact the Office because there will be a small additional interpretation fee due to the complexity of this test result. Please see Ordering Tests for worked examples of how to calculate the costs of tests and their interpretations.
The stool analysis is carried out at Genova Diagnostics in the US.
Please, note this test does not include looking for gut parasites. For that, see Comprehensive Digestive Stool Analysis with parasitology or Parasitology.
A second test, CDSA 2.0 was then designed with some markers that supersede the original CDSA. CDSA 2.0 does not report on faecal fat (measure of poor fat digestion), chymotrypsin (protein digestion) and acetates (measure of friendly fermentation). But CDSA 2.0 puts in useful additional tests, i.e.: Calprotectin and EPX - these are very sensitive markers of inflammation. If these are normal then one can exclude inflammatory bowel disease as a diagnosis. Early indications suggest this is going to be an equally reliable test for bowel cancers and therefore will be an excellent screening test. Watch this space!
Pancreatic elastase - this is a good marker of pancreatic exocrine, ie digestive function.
Secondary bile acids - this is a very useful test where there is gall bladder disease, poor digestion of fats, or upper gut fermentation. A major cause of the latter is overgrowth of prevotella - see Fermentation in the gut and CFS - and prevotella is killed by bile salts (derived from bile acids
10) Comprehensive Digestive Stool Analysis with parasitology
Test Comprehensive Digestive Stool Analysis with Parasitology - Genova Lab
Laboratory Genova
Price £210.00
Sample required stool
https://www.drmyhill.co.uk/wiki/Comprehensive_Digestive_Stool_Analysis_with_parasitology
This test gives an idea of how well foods are digested and absorbed, gives some products of gut fermentation, looks for blood in the stool, gives counts of bacteria and yeast, identifies those organisms which should not be there and lists antibiotic and/or antifungal preparations, both herbal and drug, to which that micro-organism is sensitive. It also looks for parasitic micro-organisms such as amoeba, blastocystis hominis, cryptosporydia and giardia lamblia and suggests possible treatment options.
The stool analysis is carried out at Genova Diagnostics in the USA
This test is performed on stool samples collected over 3 days and provides a detailed assessment of gut flora. It reports on bacterial and yeast flora, both beneficial and pathogenic as well as looking for parasitic micro-organisms such as amoeba, blastocystis hominis, cryptosporydia and giardia lamblia etc. . It also provides an overview of available treatments and their efficiency for treating bacterial and yeast dysbiosis.
The analysis is carried out at Genova Diagnostics in the USA
11) Comprehensive parasitology
Test Comprehensive parasitology
Laboratory Genova Diagnostics
Price £155.00
Sample required stool samples
https://www.drmyhill.co.uk/wiki/Comprehensive_parasitology
test Ova, Cysts and Parasites
Parasitic Examination, Stool https://www.labtestsonline.org.au/learning/test-index/o-and-p-or-ocp
Medical science simply doesn't have good "broad" and reliable parasite testing available unless one is in a research lab. There are some species specific antibody and PCR tests but given the thousands of different parasites, its absurd to think a doctor would guess correctly assuming they were willing to try. The Mayo Clinic ran one antibody test and Stanford ran the same antibody test based on my high IgE and EOS. Of course they were negative and that ended their effort.
When I learned that the company Ubiome was beginning to offer a Metagenomic sequencing based stool test, the "Explore Plus" last year that didn't just cover Bacteria and Archaea via 16S sequencing but also virus's and Eukaryotes, I ordered the 4 test kits for $399. Both Fungi and Parasites are Eukaryotes. Because of their wide variety and genetic breadth, using a marker sequencing via PCR just isn't effective as it is in Bacteria. Metagenomic sequencing has the incredible advantage that it doesn't assume or require guessing about "what infection you have" but simply reports all the organisms DNA it found and then a computer sorts out the "junk". Its far from perfect but it avoids the doctor "guessing" and testing.
https://shop.ubiome.com/pages/explorer-plus
user reported 'So rather than more testing, I began empirically treating it with albendazole and Praziquantel and both can cross the BB barrier. They are quite safe being used in the 100's of millions worldwide due to worm infections being common in the third world. On the third day, my constipation stopped like a miracle after 3 years of struggles. The bodywide pain declined in a near magic way. But the neurological symptoms flared including some new problems. Is it Neurocysticercosis? The Cysts are far more difficult to clear in the brain than elsewhere. The CDC says it requires 14-28 days of the anti-parasitics for Neurocysticercosis due to this difficulty.
So here I am after my first week on albendazole and Praziquantel and the changes are dramatic but the jury is still out. I thought I would share my experience here since I've seen so many people describe their symptoms as seemingly revolving around their diet, sugar and gut and IBS like symptoms. But these also include many non-gut such as fatigue, neurological and pain conditions etc'
12) Comprehensive Urine element Profile
Test Comprehensive Urine Element Profile
Laboratory Genova
Price £130.00
Sample required urine
https://www.drmyhill.co.uk/wiki/Comprehensive_Urine_element_Profile
recommend this test when I suspect metal toxicity as a cause of symptoms. This test is recommended for patients who have not yet carried out a toxic elements in urine test.
The test measures urinary levels of the following elements:- aluminium, antimony, arsenic, barium, bismuth, cadmium, calcium, cesium, chromium, cobalt, copper, gadolinium, gallium, iron, lead, lithium, manganese, magnesium, mercury, molybdenum, nickel, niobium, platinum, potassium, rubidium, selenium, strontium, sulfur, thallium, thorium, tin, tungsten, vanadium, uranium and zinc.
It is performed on a urine sample collected after a dose of DMSA, an substance which chelates metals and allows them to be excreted in urine. The reason for this is that toxic metals get "stuck" in body tissues but DMSA "grabs" them so they are excreted in urine. This is the most reliable measure of toxic metals
13) DHEA (saliva) single
Test DHEA (saliva) single
Laboratory Genova Diagnostics
Price £60.00
Sample required saliva
https://www.drmyhill.co.uk/wiki/DHEA_(saliva)_single
usually check salivary DHEA levels in patients with fatigue syndromes who are not responding to my normal work up. It is done as part of the Adrenal stress profile - salivary with saliva samples collected over 24 hour. The result also includes salivary cortisol levels.
This single sample test is used to check the level of DHEA in a patient who is on a course of pregnenolone supplementation
14) Disease screening tests
Test Disease screening tests
Laboratory TDL (DL6L, FOB, FT3)
Price £155.00
Sample required blood, urine, stool
- These tests, offered by TDL, screen for the common illnesses and include:
- haematology (for anaemia, leukaemia, blood problems), see Haematology - interpretation
- liver tests (bilirubin, enzyme levels, protein levels),
- kidney tests (urea and creatinine),
- biochemistry (sugar levels, cholesterols - total, HDL and LDL , triglycerides, sodium and calcium; but not potassium, which leaks out of cells and so cannot be done on a postal sample), see Biochemistry - interpretation
- thyroid function test, i.e. free T4,TSH (hypothyroidism is increasingly common, and my guess is that because of increasing pollution, symptoms of hypothyroidism creep up insidiously and are often mistaken for signs of aging), fecal occult blood (some bowel problems).
This group of tests screens for the majority of common diseases and is a good starting point for any investigation of health problems.
For those people who think they are otherwise well, tests of nutritional and toxic status can be used to confirm or refute that! Many diseases start with unforseen micronutrient deficiencies or unknown toxic stress. My experience is that the functional tests are more useful than measuring actual levels and so I would recommend the following:
- Antioxidant status profile
- B vitamins - functional blood profile
- B12 vitamin levels
- Essential fatty acid profile and possibly
- Vitamin D Home Test Kit
- To estimate total toxic load, Fat biopsy for pesticides or Volatile Organic Compounds would give a good indication
- https://www.drmyhill.co.uk/wiki/Disease_screening_tests
15) DNA adducts
Test DNA adducts
Laboratory TEST NO LONGER AVAILABLE
Price £116.00
Sample required blood
This test measures chemicals that have stuck on to DNA. I now use this test regularly for patients who have either been exposed to chemicals, or who have developed cancer. Almost invariably I find toxic chemicals with the most common being lindane, nickel, PBBs (used as fire retardants) and other heavy metals. It is possible to get rid of these toxins, either by using high doses of the beneficial minerals, or by using chelation therapy, or by doing sweating detox regimes, or a combination of these methods
https://www.drmyhill.co.uk/wiki/DNA_adducts
16) Elastase - a new test for pancreatic disease
Test Elastase - a new test for pancreatic disease
Laboratory TDL
Price £159.00
Sample required stool
Elastase is an enzyme normally produced in the pancreas. When the pancreas is diseased such as with insufficiency, pancreatitis or cancer, then levels of the enzyme fall. This new test is a useful diagnostic test for an organ which is difficult to get at and investigate
https://www.drmyhill.co.uk/wiki/Elastase_-_a_new_test_for_pancreatic_disease
17) Essential fatty acid profile
Test Essential fatty acid profile
Laboratory Biolab Medical Unit
Price £120.00
Sample required blood
This test measures amounts of the omega 3 and omega 6 series fats in red blood cells (these fats are found in fish oil and evening primrose oil). These are very common deficiencies and I recommend supplementing with EFAs routinely
https://www.drmyhill.co.uk/wiki/Essential_fatty_acid_profile
18) Faecal calprotectin
Test Faecal calprotectin
Laboratory The Doctors' Laboratory
Price £73.50
Sample required stool
This is a simple, non-invasive and low cost test. Calprotectin is an abundant neutrophil protein found in both plasma and stool that is markedly elevated in infectious and inflammatory conditions, including inflammatory bowel disease.
Faecal calprotectin may also be useful in determining whether clinical symptoms in patients with known IBD are caused by disease flares or non-inflammatory complications/underlying irritable bowel syndrome and in providing objective evidence of response to treatment https://www.drmyhill.co.uk/wiki/Faecal_calprotectin
19) Faecal occult blood
Test Faecal occult blood
Laboratory TDL
Price £49.50
Sample required stool sample needed
This test looks for blood in the stool. It can be used as a crude screening test for bowel cancer, but any cause of blood loss will give a positive test such as piles, sometimes ulcer disease, inflammatory bowel disease such as Crohn's or ulcerative colitis. Taking aspirin or other NSAIs (non-steroid anti-inflammatories) such as ibuprofen, diclofenac, indomethacin can also cause blood loss.
A positive result requires urgent investigation in which case you need to contact your own physician with a copy of the test result
https://www.drmyhill.co.uk/wiki/Faecal_occult_blood
20) Fat biopsy for pesticides or Volatile Organic Compounds
est Fat biopsy for pesticides or Volatile Organic Compounds
Laboratory TEST NO LONGER AVAILABLE
Price £96.00
Sample required tiny amount of fat tissue
Any presence of pesticides and/or volatile organic compounds in human tissue is abnormal and is a reflection of the polluted world in which we live. These chemicals are all lipid soluble and bio-accumulate in fatty organs, particularly the brain, breast, bone marrow and testes. Levels are measured in milligrams per kilogram. This is a comparable level to those used when testing blood levels for drugs - so these are not trace amounts but represent a substantial and significant load.
For some people with sensitivities it is possible that levels within the reference ranges are, indeed, causing them symptoms now. Many patients with multiple chemical sensitivity will react to such an endogenous chemical load. Many of these chemicals are known carcinogens and teratogens (an agent that can disturb the development of an embryo or foetus) - indeed, some authorities believe that these chemicals now cause more cancer than cigarette smoking.
It is now possible to analyse a fat sample for the presence of a number of pesticides or volatile organic compounds (Fat Biopsy). Depending on the chemicals you have been exposed to, you can choose to have your sample tested either for pesticides or for the VOCs. Each individual test costs 96 GBP.
If you would like to be tested for the full range of toxins (pesticides and VOCs), this can also be requested. The cost of the Fat cell toxins test is 171 GBP. Please, make your choice clear on the order part of the questionnaire.
A positive result does not tell us when that exposure took place, nor if these chemicals are causing symptoms now. Having said that, the commonest manifestation of such a high chemical load are chronic fatigue syndrome, multiple chemical sensitivity, neurological damage and immunological damage (reflecting damage to other organs which are relatively rich in lipids
https://www.drmyhill.co.uk/wiki/Fat_biopsy_for_pesticides_or_Volatile_Organic_Compounds
21) Fat Soluble Vitamin profile
Test Fat Soluble Vitamin profile
Laboratory Biolab
Price £100.00
Sample required blood
Many degenerative diseases are caused by free radicals. Antioxidants are the body's natural defences against free radicals. I regularly check a red cell selenium, which is the most important mineral antioxidant. This test checks the important vitamins, namely A, E and carotene
https://www.drmyhill.co.uk/wiki/Fat_Soluble_Vitamin_profile
22) Female hormone profile (Oestrogen, progesterone and testosterone levels in saliva
Test Female hormone profile RHYTHM (Oestrogen, progesterone and testosterone levels in saliva)
Laboratory Genova Diagnostics
Price £165.00
Sample required saliva samples
This is a salivary test which measures female sex hormones during a menstural cycle.
Oestradiol and progesterone levels are plotted from 12 samples taken during one monthly cycle and testosterone levels are measured from a single sample
23) Ferritin levels in serum
Test Ferritin levels in serum
Laboratory TDL
Price £83.00
Sample required blood
Ferritin is a protein found inside cells that stores iron for the body's future use. A ferritin test indirectly measures the amount of iron in your blood.
Abnormally high ferritin levels may be due to:
- Alcoholic liver disease;
- Frequent transfusion of packed red blood cells ;
- Hemochromatosis;
- Hemolytic anemia;
- Hodgkin's lymphoma;
- Megaloblastic anemia.
- Ferritin levels can become elevated if the patient has an inflammatory disorder.
- Abnormally low levels may be due to:
- Vegetarian or vegan diet;
- Hypochlorhydria;
- Long-term digestive tract bleeding;
- Heavy menstrual bleeding
https://www.drmyhill.co.uk/wiki/Ferritin_levels_in_serum
24) Full blood count
Test Full blood count
Laboratory TDL
Price £50.50
Sample required blood
This test looks at the number of red blood cells, their size and how much haemoglobin (to carry oxygen) is packaged into each one; the numbers of white cells; and also provides a break-down of the numbers of different types of cell, including the number of platelets (which allow blood to clot). One would expect to find abnormalities here in anaemia, B12 deficiency, folic acid deficiency, sometimes underactive thyroid, iron deficiency, infections, leukaemias, and - rarely - allergy or parasites.
It is a screening test very commonly done in any medical work-up of a patient. Just because it shows "normal" results does not mean all is well. However, some doctors are very naughty and tell their patients, quite erroneously, "Oh! The blood test is fine, so there is nothing the matter!"
https://www.drmyhill.co.uk/wiki/Full_blood_count
25) Glutathione peroxidase
Test Glutathione peroxidase
Laboratory TEST NO LONGER AVAILABLE
Price £25.00
Sample required blood
enzyme family whose main biological role is to protect the organism from oxidative damage. In other words they are important antioxidants. Their proper function depends on adequate levels of selenium, therefore this test is a functional test of selenium status
https://www.drmyhill.co.uk/wiki/Glutathione_peroxidase
26) Hair Mineral Analysis
Test Hair Mineral Analysis
Laboratory Biolab
Price £77.00
Sample required hair
This test measures the levels in hair of the following trace elements and toxic metals: calcium, magnesium, phosphorus, sodium, potassium, iron, copper, zinc, chromium, manganese, selenium, nickel, cobalt, lead, mercury, cadmium, arsenic, aluminium.
If there are raised levels of toxic minerals then there probably is a toxicity problem.
However normal or low levels of toxic minerals does not exclude a toxicity problem. Some people are poor detoxifiers and do not dump heavy metals in hair - they get dumped elsewhere in the body. In a study of autistic children, they were found to have lower levels of mercury in the hair compared to controls! The researchers could not understand this until they realised they were dumping the mercury in their brains instead!
The zinc level can be misleading. A low zinc probably means zinc deficiency. A normal zinc may be due to a very low zinc which then makes the hair grow slowly. This slow growth has the effect of concentrating minerals in the hair to give falsely high readings.
A high copper suggests inflammation and always needs investigating further. It is often high with the Pill and HRT - this is one of the tests which makes me worry about the Pill and HRT!
High nickel (together with high leVels of any metals) also means nickel sensitivity (to jewelry, watches, zips etc)
Chromium, cobalt, manganese and selenium levels are probably accurate.
I would not take much notice of abnormal calcium, magnesium, phosphorus, potassium or sodium results.
Low iron needs further investigation with a ferritin serum test.
However, if all the essential minerals are low (excluding the toxics) I would think of poor nutrition or malabsorption of foods. See Malabsorption - failure to get the goodness from food
https://www.drmyhill.co.uk/wiki/Hair_Mineral_Analysis
27) Helicobacter pylori antibodies
Test Helicobacter Pylori antibodies
Laboratory TDL
Price £88.50
Sample required blood
This test looks at the level of antibodies in the serum to the helicobacter pylori bacteria. A positive result is evidence of present or past infection. If you have never had eradication therapy, then a positive result means you probably do have an infection now.
If the result of this test is positive, you may need eradication therapy which has to be prescribed be your GP/physician. I say "may need" because some physicians choose not to eradicate in cases of oesophagitis because their clinical experience suggests some cases are worsened.
There is some research which suggests H pylori may be a risk factor for atherosclerosis (arterial disease) - another good reason to get rid of it! See Arteriosclerosis - what causes it and how to prevent it
https://www.drmyhill.co.uk/wiki/Helicobacter_pylori_antibodies
28) Helicobacter Pylori breath test
Test Helicobacter Pylori Breath Test
Laboratory Infai
Price £38.00
Sample required breath sample
This test is a measure of current, as opposed to past, infection with helicobacter pylori bacterium. It is useful to monitor whether or not eradication therapy has been effective.
If the result of this test is positive, you need eradication therapy which has to be prescribed by your GP/physician.
It is possible that H. pylori is a risk factor for arterial disease - see Arteriosclerosis - what causes it and how to prevent it - another good reason for getting rid of it
https://www.drmyhill.co.uk/wiki/Helicobacter_Pylori_breath_test
29) Lipid profile - cholesterol and triglycerides in the blood
Test Lipid profile - Cholesterol and tryglicerides in the blood
Laboratory TDL
Price £58.00
Sample required blood
Patients are now frequently offered a test of blood cholesterol level and triglycerides. This normally just measures total cholesterol. However, for a more detailed breakdown of the good fats and the bad fats, you also need HDL cholesterol (good fat) and LDL cholesterol (bad fat). The Lipid Profile includes all three measurements as well as triglycerides
https://www.drmyhill.co.uk/wiki/Lipid_profile_-_cholesterol_and_triglycerides_in_the_blood
30) Litmus paper test
Test Litmus paper test
Laboratory N / A
Price £3.00
Sample required urine
This test helps to make the diagnosis of hyperventilation.
Hyperventilation is a clinical diagnosis. However during an acute attack of hyperventilation, the pH (acidity) of the blood changes to alkali and so does the urine. Testing urine with litmus paper after an attack could suggest a diagnosis of hyperventilation. Please see Hyperventilation - makes you feel as if you can't get your breath
This test wants to be done in conjunction with other measures of hyperventilation such as re-breathing into a paper bag, measuring how fast you breath, ability to hold a controlled pause, symptoms and provoking factors etc. The litmus test is just part of the diagnosis
https://www.drmyhill.co.uk/wiki/Litmus_paper_test
31) Lymphocyte sensitivity to metals and chemicals
Test Lymphocyte sensitivity to metals and chemicals
Laboratory TEST NO LONGER AVAILABLE
Price £81.00 for up to 12 test substances
Sample required blood
This test looks at the sensitivity of lymphocytes (a type of white blood cells) to a range of substances which are potential allergens. The test substances are grouped in several categories (see below). The price in the test information box opposite is for up to 12 substances. They can be selected from any category. To order the test, please give the name of the test in the questionnaire and list your chosen substances. If your list has more than 12 substances, then the price per each additional test substance is £7. So, 14 substances would cost £81 + 2 x £7 = £95.
For a complete list of substances that can be tested for, please have a look here: Lymphocyte sensitivity test - list of test substances
https://www.drmyhill.co.uk/wiki/Lymphocyte_sensitivity_to_metals_and_chemicals
32) Magnesium test - red cell
Test Magnesium test - red cell
Laboratory Biolab Medical Unit
Price £38.00
Sample required blood
This test measures the amount of the mineral magnesium inside the red blood cells. This is the test I do most often, partly because I see many patients with fatigue, partly because it is a very common deficiency and partly because it is a very difficult mineral to correct.
Most doctors do not understand the difference between a serum magnesium and a red cell magnesium. Serum levels must be kept within a tight range, or the heart stops. Therefore serum levels are maintained at the expense of levels inside cells. Most labs just do serum levels and patients are told their magnesium is normal.
So we have to measure intracellular magnesium. The easiest cell to get at is the red cell, hence this test.
For advice on treating magnesium problems please see Magnesium
https://www.drmyhill.co.uk/wiki/Magnesium_test_-_red_cell
33) Mercury- DMSA Provocation test
Test Mercury - DMSA Provocation
Laboratory Biolab Medical Unit
Price £110.00
Sample required urine
This test is used to assess the body's burden of mercury by measuring urine mercury levels before and 2.5 hours after the patient takes the chelating agent DMSA
https://www.drmyhill.co.uk/wiki/Mercury-_DMSA_Provocation_test
34) Microbial ecology profile
Test Microbial ecology profile
Laboratory Genova Diagnostics
Price £190.00
Sample required STOOL
The stomach, duodenum and small intestine should be free from micro-organisms (bacteria, yeast and parasites – hereafter called bugs!). In the large bowel, on the other hand, we have huge numbers of bugs. Foods that cannot be digested upstream are fermented in the large bowel to produce many substances highly beneficial to the body. This also generates heat to help keep us warm. While the human body is made up of 10 million million cells, in our gut we have 100 million million bugs or more, i.e. ten times as many! Bugs make up 60% of dry stool weight, there are over 500 different species, but 99% of bugs are from 30-40 species. All is well when these bugs are the beneficial ones, but things can go wrong when pathogenic organisms set up camp in the large bowel.
In this test Genova Diagnostics lab can measure the amount of different bacteria, both beneficial and pathogenic, in a stool sample
https://www.drmyhill.co.uk/wiki/Microbial_ecology_profile
35) Mitochondrial Function Profile
Test Mitochondrial Function Profile
Laboratory PROFILE NO LONGER AVAILABLE
Price £300.00 (includes complimentary 2nd Edition of Diagnosis and Treatment of CFS/ME book, or other nominated book)
Sample required blood
This blood test combines several tests which together assess mitochondrial function and identify where the problem areas with energy production are. It is exceptionally useful for chronic fatigue syndrome / ME sufferers as it gives clear indications for a treatment regime. More details of the test can be found in CFS - The Central Cause: Mitochondrial Failure
Mitochondrial function profile is made up of the following individual tests:
- ATP profiles;
- NAD (functional B3);
- SODase;
- L-carnitine;
- Cell-free DNA;
- Glutathione Peroxidase.
- All the above tests are performed at Acumen Laboratory
- Co-enzyme Q10 - this test is performed at Biolab Medical Unit
About "ATP profiles"
The most significant test in the Mitochondrial function profile is called "ATP profiles". It was developed by Dr John McLaren-Howard. The result is made up of three elements. First of all, it measures the rate at which ATP is recycled in cells. Because production of ATP is highly dependent on magnesium status so the first part of the test studies this aspect.
The second part of the test measures the efficiency with which ATP is made from ADP. If this is abnormal, then this could be as a result of magnesium deficiency, and/or low levels of Co-enzyme Q10, and/or low levels of vitamin B3 (NAD) and/or low levels of acetyl L-carnitine.
The third possibility is that the protein which transports ATP and ADP across mitochondrial membranes is impaired and this is also measured
https://www.drmyhill.co.uk/wiki/Mitochondrial_Function_Profile
35b)Traditional blood tests measure NAD
Lactic acid and pyruvate (blood):
- Pyruvic acid comes from foods and supplies energy to the citric acid cycle when oxygen is present and alternatively ferments to produce lactic acid when oxygen is lacking (fermentation). Therefore elevated lactic acid or pyruvate may be a signal of NAD deficiency.
Specialty lab tests
- Organic Acid testing (urine) is available from Genova Diagnostics, Great Plains Laboratory and Metametrix Clinical Laboratory:
- Pyruvate and lactic acid can also be measured in a first-morning urine.
36) Organic acids present in urine (Metabolic Analysis Profile)
Test Organic acids present in urine (metabolic analysis profile)
Laboratory Genova Diagnostics
Price £210.00
Sample required urine
Urine contains a great number of waste products from the body and by analysing these one can learn an awful lot about what is going on in the internal workings of the body. It is a little bit like rummaging through the rubbish that has been thrown out of a house - that would tell you a great deal about what went on in that house with respect to the occupants' diet, work, hobbies, interests and so on. I have rather avoided doing urinary organic acids in the past because it supplies so much information about so many different substances that the interpretation was really very difficult. However, Genova Diagnostics have got their head around this problem and have listed all the amino acids, enzymes, breakdown products of metabolism, bacterial markers, detox enzymes and so on in such a way that it is much more clear what the problem is. Obviously there will be overlaps because many compounds do more than one job, but by packaging these together in groups it has become very much more obvious what is or is not going on.
Indeed I was interested to hear from Dr Chris Heard that this is a test he now does routinely in his autistic children - partly because it is non-invasive, i.e. no needles, and partly because there is a great deal of useful information that he can glean from this.
For example, the grouping together of twenty nine different measures of amino acids and waste products gives one a good idea about antioxidant status. Looking at fourteen other organic acids gives one a handle on mineral status. B6 status can be determined by looking at levels of sixteen different substances. So, through one test one can get a handle on antioxidants, minerals, B vitamins, protein malabsorption and maldigestion, bacterial dysbiosis, yeast fungal dysbiosis, nitrogen balance, detoxification ability, methylation ability, oxidative stress, neurotransmitter balance, markers of malabsorption and dysbiosis, markers of cellular energy and mitochondrial metabolites (from glycolosis, citric acid cycle, ketones and fatty acids), and organic acids for co-factor needs.
I anticipate using this test when I get stuck. There is probably little point in using it early on in the work up of any problem because "common things are common" and everybody has to do my basic work up. However, if we are not making progress then this could be a very useful test because it allows us to concentrate our efforts in certain areas
https://www.drmyhill.co.uk/wiki/Organic_acids_present_in_urine_(Metabolic_Analysis_Profile)
37) Parasitology
Test Parasitology
Laboratory Genova Diagnostics
Price £111.00
Sample required stool sample
This test is performed on stool samples collected over 3 days and looks for and identifies parasitic micro-organisms such as amoeba, blastocystis hominis, cryptosporydia and giardia lamblia etc.
If a more detailed assessment of gut flora is needed, then Comprehensive parasitology might be useful. This test reports on bacterial and yeast flora as well as looking for parasites in the stool samples. It also provides an overview of available treatments for bacterial and yeast dysbiosis.
The analysis is carried out at Genova Diagnostics in the USA
https://www.drmyhill.co.uk/wiki/Parasitology
38) Short chain fatty acids
Test Short chain fatty acids
Laboratory TEST NO LONGER AVAILABLE
Price £48.00
Sample required blood
Short chain fatty acids are produced in the large bowel as a result of bacterial fermentation of soluble fibre. They can provide over 500 kcals a day of energy which is especially useful when blood sugar levels fall low because mitochondria like to use SCFAs as an energy source. At night we all switch to SCFAs as blood sugar levels fall and this prevents hypoglycaemia at night. Night-time hypoglycaemia is a common cause of disturbed sleep.
This test looks for a hypoglycaemic tendency by measuring levels of short chain fatty acids first thing in the morning before breakfast has been taken. The logic is that when there is hypoglycaemia, the body switches early to using short chain fatty acids for energy supply and these will then deplete. Therefore, low levels of short chain fatty acids indicate a hypoglycaemic tendency. Hypoglycaemia is a common problem for people with a fermenting gut, so the test may indirectly be pointing to a problem with yeast or bacterial overgrowth in the bowel.
Low levels of SCFAs may also be indicative of a low fibre diet. This can be helped by eating foods rich in fibre such as nuts, seeds and vegetables
https://www.drmyhill.co.uk/wiki/Short_chain_fatty_acids
39) Short chain polypeptides - another measure of protein digestion and absorption
Test Short chain polypeptides
Laboratory TEST NO LONGER AVAILABLE
Price £81.00
Sample required blood
Incomplete digestion of proteins produces short chain polypeptides which may mimic hormones, neurotransmitters, cytokines and chemotactic agents. This test may help explain inexplicable reactions to foods
40) SODase (superoxide dismutase) studies
Test SODase (superoxide dismutase) studies
Laboratory TEST NO LONGER AVAILABLE
Price £75.00
Sample required blood
Superoxide dismutase is one of the most important antioxidant enzymes which mops up free radicals. It is the most important superoxide scavenger in muscles. Deficiency can explain muscle pain and easy fatiguability in some patients. Normal levels of SODase are dependent on good levels of copper, manganese and zinc.
In addition this test will also report levels of glutathione peroxidase and red cell glutathione, which are also front line antioxidant
https://www.drmyhill.co.uk/wiki/SODase_(superoxide_dismutase)_studies
41) Thyroid profile: free T3, free T4 and TSH
Test Thyroid profile: free T3, free T4 and TSH
Laboratory TDL
Price £74.50
Sample required blood
This test measures the amount of thyroid stimulating hormone (TSH) as well free T4 and free T3 in the blood serum.
There are three common ways in which there may be inadequte amounts of the thyroid hormone for normal metabolism. The one which all doctors are aware of is primary hypothyroidism, in which there is a raised TSH and a low T4 and low T3. This is due to failure of the thyroid gland itself, possibly due to autoantibody disease, possibly due to toxic stress or possibly due to iodine deficiency.
The second, and in my view the most common cause of thyroid failure, occurs at the pituitary level. In this condition there is inadequate thyroid stimulating hormone (TSH) produced from the pituitary and so one tends to see low or normal TSHs, low T4s and variable T3s. This condition I see most commonly in my patients with chronic fatigue syndrome, where there is a general suppression of the hypothalamic-pituitary-adrenal axis.
The third type of under-functioning is due to poor conversion of T4 to T3. This requires enzymes and co-factors, in particular selenium, zinc and iron. In this condition there are normal or possibly slightly raised levels of TSH, normal levels of T4 but low levels of T3. This requires micronutrients and also T3 to correct.
Therefore, in any patient in whom I suspect a thyroid problem I now routinely ask for a TSH, a Free T4 and a Free T3 in order to gain the full picture.
Important message to non-patients or old patients over 2 years, wishing to have thyroid hormones prescribing
If you have a thyroid function test via my website and the results indicate a need for thyroid supplementation, then I will first ask your GP to consider prescribing this for you in my letter of interpretation.
If your GP is not willing to prescribe thyroid hormones, then I would be able to do so, ON THE CONDITION THAT either your GP or a thyroid specialist agree to monitor your thyroid function regularly to check that you remain EUTHYROID; that is to say, you do not have any symptoms of thyrotoxicosis. These symptoms and signs would be: racing pulse, tremor, undue anxiety, undue sweating, irritability, unexplained weight loss, unexplained loss of muscle, unexplained osteoporosis, bulging eyes (exophthalmos) or unexplained goitre. Before I can start prescribing thyroid hormones, I would need written assurance either from your doctor (NHS or private) that he will be monitoring you clinically or from you confirming that you have such a doctor who is happy to monitor you.
Old patients who have had contact within 2 years, are welcome to send in a thyroid result and UPDATE questionnaire for 45 minutes of my time (£165).
Old patients who have not had contact for more than 2 years are welcome to send in a result and a FULL medical questionnaire for 1 hour of my time (£275).
If you cannot find a doctor who can state that you are euthyroid, then you would need an hour and a half appointment (currently £330) with me here in Mid Wales to initiate thyroid hormone prescribing, OR I would refer you to a local specialist
https://www.drmyhill.co.uk/wiki/Thyroid_profile:_free_T3,_free_T4_and_TSH
41b) home iodine loading test
salt intake, combined with a decline in the use of iodophors by the dairy industry and in commercial bread production, has lead to the re-emergence of this mineral deficiency around the world. Since iodine is required for the synthesis of thyroid hormones, the major indication of iodine deficiency include hypothyroid symptoms. An iodine deficiency during pregnancy can result in cretism, lowered IQ, mental retardation and stunted growth. Iodine may also play a role in the maintenance of healthy breast tissue and cancer prevention. Its antioxidant, immune regulating and estrogen modulating functions may be mechanisms by which these properties can be explained.
Research has indicated that severe iodine deficiency has more than quadrupled in Australia over the last 20 years; increasing from 2.6% to 11.7%. Even more disconcerting is the observation that nearly half of the pregnant women in these areas also have this mineral deficiency.
Iodine Loading Test: Assesses iodine deficiency firstly by measuring iodine levels in a morning spot urinary specimen (random iodine test) and the loading test analyses iodine deficiency using a much more sensitive technique. For this part of the test, 50mg of an iodine/iodide mixture is given as a loading dose and the amount of iodine excreted in the urine over the next 24 hours is measured.
If the patient is iodine deficient, the body retains the iodine and only a small quantity of the mineral is excreted into the urine. If the patient has sufficient iodine levels, the body does not retain the iodine and the majority of the iodine dosage is excreted into the 24 hour urinary sample. In contrast to the random iodine test, the iodine loading test is able to detect mild and moderate as well as severe deficiencies.
Common Conditions:
- Thyroid abnormalities
- Decreased fertility
- Fibrocystic breast disease
- Estrogen imbalance
- Fatigue
- Depression
- Weight gain
42) Translocator protein studies
Test Translocator protein studies
Laboratory TEST NO LONGER AVAILABLE
Price £111.00
Sample required blood
ATP is made inside mitochondria, but is used outside mitochondria but still inside the cells. ATP therefore has to get across the mitochondrial membrane to deliver its energy. Once done ATP has been converted back to ADP and this needs to be recycled back through the mitochondrial membrane. What allows ATP and ADP to cross mitochondrial membranes is a dedicated carrier protein called translocator protein.
The ATP profile test (part of the mitochondrial package) looks at how efficiently TL proteins work. It is common in patients with CFS to find blockages. The TL protein studies looks at why TL protein may be malfunctioning. It could be because of blockage by chemicals (xenobiotic stress such as organochlorines, organophosphates), blockage because of poor antioxidants status (lipid peroxides), because of products of detox (glutathione conjugates), mineral deficiencies, high calcium, pH disturbances, switches into anaerobic metabolism or whatever. This provides important clues towards further management
https://www.drmyhill.co.uk/wiki/Translocator_protein_studies
43) Vascular endothelial growth factor (VEGF)- salivary test for hypochlorhydria
Test Vascular endothelial growth factor - salivary test for hypochlorhydria
Laboratory TEST NO LONGER AVAILABLE
Price £81.00
Sample required saliva
John McLaren-Howard has again come up with a brilliant suggestion for a simple test to diagnose hypochlorhydria. The idea here is that it is very difficult for the stomach to produce stomach acid. The normal acidity of blood is about pH7, but the acidity of stomach acid can be as low as pH 2 or below. That means that hydrogen ions (which create acidity) are a 100,000 times more concentrated in the stomach than in the bloodstream. So the stomach wall has a very difficult job to do. The gastric parietal cells need quite a bit of energy from ATP to pump hydrogen ions from the inside of the parietal cell into the lumen of the stomach. The difficult bit is stopping these hydrogen ions leaking back again. This is achieved because the gastric parietal cells forming a protective barrier between each other at the cell membrane tight junction to stop hydrogen ions leaking back. Because this is extremely hard work and the body does not want to waste energy, the main regulator for the cell membrane tight junction is vascular endothelial growth factor (VEGF). This is produced by the salivary glands.
What this means is that the more stomach acid is produced, the more VEGF is necessary to keep the glue going between gastric parietal cells. Therefore, one would expect salivary VEGF levels to be proportionate to the amount of stomach acid. And indeed this is the case. There is a huge amount of research that has been done with respect to VEGF, most of which is to do with high levels. However, the reverse is also true and low levels of VEGF would be a pointer towards hypochlorhydria.
This test would be invalidated by taking proton pump inhibitors and possibly other acid blockers, so for the best chance of an accurate result, really these drugs need to be stopped for four days prior to doing the test
44) RNS repetitive nerve stimulation
45) Vitamin D Home Test Kit
46) anti-VCA IgG of EBV
SelfHacked tests
2) The ACTH test measures the amount of ACTH in the blood. This test is often performed alongside a cortisol test to help identify problems with the adrenal glands or pituitary glands.
More specifically, the ACTH test (and a cortisol test) are used to help diagnose 2, 3:
- Cushing’s syndrome (when the adrenal glands produce too much cortisol)
- Cushing’s disease (when the adrenal glands produce too much ACTH)
- Addison disease (when the adrenal gland does not produce enough cortisol)
- Adrenal and pituitary tumors
ACTH levels can vary throughout the day, so blood tests are typically performed in the morning when levels are highest. A doctor may request that the patient fast overnight before the test
https://selfhacked.com/blog/acth
3) An albumin blood test measures the amount of albumin in the blood. Low albumin is common in many health problems, so albumin levels are often checked in conjunction with other tests to help diagnose diseases, determine if other tests are needed, or to check if treatments for a condition are working. An albumin blood test is a standard part of the following sets of blood tests:
- Comprehensive Metabolic Panel (CMP) for an overall picture of health
- Liver Function Panel to assess inflammation, infection, or liver damage and disease
- Total Protein to check nutrition, general health, or to diagnose liver and kidney diseases
- Renal Panel to diagnose or monitor kidney conditions
https://selfhacked.com/blog/albumin/
4) Blood iron tests are typically ordered as follow-up tests when routine tests such as a complete blood count, hemoglobin, and hematocrit levels show abnormal results.
1) Blood Iron
Blood iron measures the amount of circulating iron in the blood. Blood iron is a poor measure of iron status in the body because it fluctuates daily depending on the ingestion of iron-containing foods 26, 27.
A blood iron test without a TIBC or transferrin has limited value except in cases of iron poisoning. Normal range of iron is around 50-195 mcg/dL or µg/dL (8.95 – 35 µmol/L) in men and 40-190 mcg/dL (7.16 – 34 µmol/L) in women. Ranges will vary slightly between labs, due to differences in equipment, techniques, and chemicals used.
2) Serum Ferritin
Ferritin levels can serve as a measure of total body iron stores 28.
Low ferritin levels signal that the body’s iron stores are low. Higher levels, on the other hand, may indicate that you have a condition that causes the body to store too much iron 29.
However, ferritin is also an acute phase protein, which means it plays a role in the immune response, and increases in conditions such as chronic inflammation, infections, and cancer, irrespective of iron levels 29, 27, 30.
Read this post to learn more about ferritin.
According to the World Health Organization, the generally accepted cut-off level for blood ferritin levels in which iron stores are depleted is 15 ng/mL for people aged 5 years and older and 12 ng/mL for people younger than 5 years of age 31.
3) Total Iron-Binding Capacity
Total iron-binding capacity (TIBC) measures the total capacity of your blood to bind and transport iron. It is used to estimate the amount of iron stored in your body 32.
TIBC is an indirect measure of transferrin, a protein that binds iron molecules and transports them in the bloodstream 33, 34.
Normal range is around 250 – 450 µg/dL or 44.8 – 76.1 µmol/L. Raised TIBC is characteristic of iron deficiency anemia.
4) Unsaturated Iron-Binding Capacity
UIBC (unsaturated iron-binding capacity) measures the reserve capacity of transferrin, the portion of transferrin that has not yet been saturated with iron. UIBC also reflects transferrin levels.
5) Transferrin Saturation
Transferrin (iron) saturation, also called % saturation, is the percentage of transferrin that is saturated with iron.
Transferrin saturation is calculated by dividing iron levels by total iron-binding capacity (TIBC).
Normally transferrin saturation ranges between 15 – 55 %.
Transferrin saturation <15% indicates iron deficiency, while high levels indicate iron overload (hemochromatosis, transfusional iron overload) 27.
The combined results of transferrin, iron, and TIBC tests are helpful in the differential diagnosis of anemia, iron-deficiency anemia, thalassemia, sideroblastic anemia, and hemochromatosis.
6) Red Cell Zinc Protoporphyrin
When there is an inadequate supply of iron, zinc is incorporated into the protoporphyrin ring of the heme structure, creating zinc protoporphyrin. An elevated zinc protoporphyrin is characteristic of iron-deficient red blood cell production 27.
7) Serum Transferrin Receptor
An elevated serum transferrin receptor (sTfR) is a marker of tissue iron deficiency and increased bone marrow erythropoietic activity.
Since concentrations of transferrin receptor rise when iron stores are depleted to promote cellular iron uptake, they can be used to estimate the magnitude of functional iron deficit once iron stores are depleted 35.
Transferrin levels reflect the extent of red blood cell production and iron demand since the transferrin receptor is mainly derived from developing red blood cells 36.
Advantages of Serum Transferrin Receptor Testing 37, 28, 30:
- It is an early and sensitive indicator of iron deficiency
- It can distinguish between anemia from chronic disease vs. iron deficiency anemia.
- It is not significantly affected by infection or inflammatory processes, and it does not vary with age, gender, or pregnancy
Normal ranges are between 2.8 – 8.5 mg/L 38
https://selfhacked.com/blog/iron-balance-blood-test-iron-deficiency-anemia-overload/
5) Androstenedione Test
Androstenedione can be measured directly from a blood sample 42.
Normal Range for Adult Men
According to the Endocrine Society, which manages multiple journals on endocrine research, adult men should have androstenedione levels in the range of 65–210 ng/dL or 2.27–7.33 nmol/L.
These levels will decrease with age, and the highest numbers are only expected for young adults shortly after adolescence 43, 44.
Normal Range for Adult Women
According to the Endocrine Society, adult women should have androstenedione levels in the range of 80–240 ng/dL or 2.79–8.38 nmol/L. However, other studies of healthy women have found androstenedione levels range from 0.89 to 4.56 nmol/L. As is the case for men, these levels will decrease with age 43, 45.
Higher androstenedione levels are normal in younger women, but test results outside the reference range may be a sign of polycystic ovarian syndrome (PCOS) 46
https://selfhacked.com/blog/androstenedione/
6) AMH tests evaluate blood samples to determine the AMH concentration. The ranges defining normal AMH levels vary between tests 6.
While AMH is the most accurate existing reflection of the quantity of a woman’s eggs and follicles (ovarian reserve), to achieve the most accurate depiction of a woman’s ovarian reserve, antral follicle count must also be measured 2.
You can request that your doctor test your AMH levels. FSH and estradiol are also part of the routine check, but since they fluctuate with every cycle, they are not accurate markers of ovarian reserve 2
https://selfhacked.com/blog/anti-mullerian-hormone/
7) Aspartate aminotransferase (AST), also known as SGOT, is an enzyme that breaks down proteins for energy. It is found mainly in the liver and heart, but also in many other tissues, including the muscles, red blood cells, kidneys, and the brain. When any one of these tissues is damaged or diseased, AST is released into the blood 1, 2.
AST levels are often measured to check overall liver health. However, as mentioned above, increases in AST levels can also be due to damage to other organs, such as the heart, kidneys, or muscles. Therefore, AST is often paired with other tests in order to determine the specific location of the problem
https://selfhacked.com/blog/aspartate-aminotransferase-ast/
8) Adiponectin levels are a marker of metabolic health. Low or high levels don’t necessarily indicate a problem if there are no symptoms
https://selfhacked.com/blog/adiponectin/
9) The albumin/globulin ratio (A/G ratio for short) is a test that compares the concentrations of albumin and globulin in the blood 1, 2, 3
Albumin and globulin are proteins that are naturally found in the serum, the liquid part of your blood that doesn’t include blood cells or clotting components 1.
An imbalance in the ratio of albumin to globulin may signify ongoing inflammation, liver problems, or in rare cases immunodeficiency. There is emerging evidence that a low ratio (less albumin and more globulin) may be associated with the risk of cancer and may also predict worse outcomes in cancer and heart disease patients
https://selfhacked.com/blog/albumin-globulin-ratio
10) The normal range of alkaline phosphatase in the blood is 20 to 140 U/L, although this can vary from lab to lab. Some labs set the range at 30 to 130 U/L. Children and pregnant women can have significantly higher levels of the enzyme in their blood
https://selfhacked.com/blog/low-alkaline-phosphatase
11) Blood/Serum Total Amylase
Blood (serum) amylase consists of approximately equal amounts of salivary and pancreatic amylase. Therefore, abnormal levels of either will affect the total blood levels 6, 1.
Most often, your doctor will order an amylase test if they suspect issues with your pancreas, such as inflammation (pancreatitis). Symptoms of pancreas inflammation include 27, 28:
- Moderate to severe abdominal or back pain
- Nausea
- Vomiting
- Loss of appetite
- Oily stools
However, if you want to know for certain whether you have pancreatitis, the amylase test is not the best test to take. This is because amylase can be increased or decreased by a myriad of causes, many of them pancreas-unrelated. Lipase, for example, is a better test of pancreas function.
The normal range for blood (serum) amylase can differ somewhat between laboratories. Generally, it’s around 30 – 120 U/L (units per liter).
Salivary and Pancreatic Amylase
Apart from the total amylase, some tests can differentiate between pancreatic and salivary amylase. These tests can zero in on exactly what is going on in your body with greater precision 2.
For salivary amylase, the normal range is around 11 – 83 U/L
For pancreatic amylase, the normal range is 10 – 53 U/L
These can also vary slightly between laboratories.
Urine Amylase
Finally, there is also a urine amylase test.
Kidneys eliminate amylase from the blood into the urine. When blood levels are high, the urine levels will also increase, unless the kidneys are not functioning properly – in which case the kidneys are not able to remove amylase efficiently 29.
When needed, urine amylase may be used instead of the blood test because it’s less invasive 30.
The normal range for urine amylase is 24 – 400 U/L
https://selfhacked.com/blog/amylase
12) https://selfhacked.com/blog/anion-gap
The anion gap cannot be directly measured, instead, it is calculated from the results of an electrolyte panel, another type of blood test.
The anion gap is calculated using the concentrations of the major anions in the blood, chloride and bicarbonate, and the major cations, sodium and potassium.
However, the concentration of potassium in the blood is usually much lower compared to sodium, chloride, and bicarbonate. Therefore, it is common practice to not use potassium when calculating the anion gap, as it usually has little effect 1.
In the body, the total positive charge from cations should equal the total negative charge from anions in the blood to maintain overall neutrality.
However, blood tests usually do not measure all types of ions. This means the anion gap gives us a picture of the unmeasured anions and cations in the blood. There are normally more unmeasured anions than cations, hence there is usually an anion gap 2.
Clinically, the anion gap value is primarily used to help evaluate acid-base disorders, which occur when the concentration of acids and bases in the blood becomes unbalanced 2.
Although the term anion gap usually refers to the concentrations of cations and anions in the blood, it can also refer to their concentrations in the urine
13) https://selfhacked.com/blog/apolipoprotein-b
Testing ApoB is not part of routine practice, but doctors will use ApoB to help determine your risk of heart disease if you have a family history of heart disease or other heart disease risk factors (i.e. high cholesterol and triglycerides). It is also used to diagnose genetic diseases that cause extremely low or high ApoB levels
14) https://selfhacked.com/blog/alanine-aminotransferase
ALT blood test may be ordered to 10, 11, 12, 13:
- Assess liver health
- Investigate symptoms of liver disease, such as abnormally yellow skin or eyes (jaundice), or pain in the upper-right section of the abdomen
- Monitor progression of a liver disease
- Evaluate the effectiveness of a treatment for liver disease
- Determine if the liver is involved in or damaged by a health condition, such as diabetes or heart disease
Since ALT is an enzyme, its levels are typically determined by measuring its activity (the rate at which ALT transforms L-alanine and α-ketoglutarate into pyruvate and L-glutamate) 14.
ALT levels are often measured together with the liver enzyme aspartate transaminase (AST). The ratio of AST/ALT is also sometimes used as a marker of liver health.
While ALT levels can signal the presence of liver damage, they cannot determine the type of damage, such as scarring, infection, or inflammation
15) https://selfhacked.com/blog/need-know-aldosterone-health-effects
Aldosterone
This post focuses on the science of blood pressure regulation and electrolyte balance in relation to aldosterone. It is solely informational. Talk to your healthcare provider if your blood pressure and/or labs are abnormal
16) total alkaline phosphatase (ALP) test is run to find all types of ALP in the blood to diagnose bone and liver disorders
https://selfhacked.com/blog/alkaline-phosphatase-normal
17) https://selfhacked.com/blog/amylin
Amylin
Lab results are commonly shown as a set of values known as a “reference range”, which is sometimes referred to as a “normal range”. A reference range includes the upper and lower limits of a lab test
18) https://selfhacked.com/blog/anti-ccp-antibody-test
The anti-CCP antibody test measures your body’s level of antibodies that commonly target specific proteins found in the joints. These antibodies are commonly found in rheumatoid arthritis patients
19) https://selfhacked.com/blog/basophils
Basophils
results are commonly shown as a set of values known as a “reference range”, which is sometimes referred to as a “normal range”. A reference range includes the upper and lower limits of a lab test
20) https://selfhacked.com/blog/bilirubin-benefit-how-to-optimize
Bilirubin
Causes shown below have been associated with lower bilirubin. Your doctor will interpret your results, taking into account your medical history, symptoms, and other test results
21) https://selfhacked.com/blog/causes-of-high-or-low-blood-urea-nitrogen-bun
A blood urea nitrogen (BUN) test is performed to:
- See if your kidneys are working normally or if kidney disease is progressing
- Check for severe dehydration
Any standard blood test will have BUN or urea numbers.
Conventional doctors will look at high or low BUN numbers and not mention anything, but these can indicate that certain processes in the body aren’t optimal
22) https://selfhacked.com/blog/bun-creatinine-ratio-high-low-levels-normal-range
BUN (blood urea nitrogen) and creatinine are two blood tests that can reveal a lot about your metabolism, kidney, liver, and overall health. And while they can be used separately, the BUN/creatinine ratio can help pinpoint iissues
23) https://selfhacked.com/blog/bdnf-genes-correct/
The BDNF Gene rs6265 levels
24) https://selfhacked.com/blog/bilirubin-test
Bilirubin is normally measured with a blood test. A healthcare professional will collect a blood sample from your vein and send it to a lab for analysis. The test determines your total and direct bilirubin levels. Indirect bilirubin is what is left after subtracting direct bilirubin from the total 11.
The bilirubin test is normally included in a liver panel or a complete metabolic panel
25) https://selfhacked.com/blog/bmd-z-score
Z-score is a comparison of your individual bone mineral density (BMD) to what is expected for a person of the same age and sex. The Z-score represents how far off your score is (measured in the number of standard deviations) from the average score of healthy people of similar age, ethnicity
26) https://selfhacked.com/blog/beta-carotene
Beta-carotene is not a routine test. But it is possible to test it using a simple blood test. Women will usually have slightly higher levels than men 5.
Normal levels for men are around 4 – 51 ug/dL (micrograms per deciliter) and for women 6 – 77 ug/dL. Levels may vary slightly between laboratories
27) DHEA-S, Testosterone (Total, Bioavailable, and Free, HDL-C, C-reactive Protein, HbA1c, Triglycerides, Homocysteine
28) https://selfhacked.com/blog/brca1-brca2-genes
29) Tests You May Not Be Getting
1) Insulin
Even if your blood sugar (glucose) levels are fine, your body may still be struggling to keep them in line. You will know if that’s the case when you check your insulin levels.
Insulin is a hormone that is released when you eat in order to help move glucose from the blood into the tissues (mainly muscles, fat tissue, and liver) 1, 2. Insulin levels can go out of balance long before blood sugar does (you can read more about insulin resistance here).
Researchers found that having fasting insulin levels above the optimal range increases your risk of developing metabolic syndrome, diabetes, heart disease, and dementia 3, 4, 5, 6, 7, 8. For example, one study found that a fasting insulin level above 9.0 uIU/mL (well within the normal range of up to 25 uIU/mL) could identify prediabetes with 80% accuracy 5.
2) Ferritin
You may be testing your iron levels, but are you checking your ferritin? Even if your iron is within the normal range, low ferritin can indicate iron deficiency. And if you have unexplained fatigue and ferritin is on the lower side – that indicates you are deficient in iron.
Ferritin is an iron-storing protein. It is important for maintaining proper levels of iron and making sure that iron is available for the different bodily processes that need it. Essentially, ferritin is a measure of your body’s iron stores 9.
Low ferritin levels are usually due to some kind of gut inflammation that is not allowing the person to absorb iron well, or because of hypothyroidism. When iron (indicated by ferritin) is lower, it can worsen existing health problems. Studies suggest that low ferritin may increase the risk of depression and anxiety by about twofold 10, 11.
Conversely, ferritin may be high in many chronic inflammatory conditions including metabolic syndrome, fatty liver, kidney disease, autoimmune disease, diabetes, and cancer 12. This makes ferritin a marker of acute and chronic inflammation.
You can read more about ferritin here.
3) Magnesium
Here is an alarming statistic – research suggests that about half (48%) of the U.S. population is deficient in magnesium 13.
Why is this alarming? Magnesium is the 4th most abundant mineral in our bodies and it’s required for more than 300 different bodily processes 14, 15. A deficiency can wreak havoc on your health. When your magnesium levels are low, you may experience a loss of appetite, fatigue, nausea, insomnia, irritability, and muscle weakness.
In addition, the older you get, the less efficiently your body holds onto magnesium 16, 17, 18. In its worst stages, magnesium deficiency can contribute to osteoporosis, heart disease, high blood pressure, and diabetes 19, 20, 21, 22, 15, 14, 23.
Thankfully, magnesium levels are very easy to test. If your levels are suboptimal or low, you can correct them by increasing your intake of magnesium-rich foods or supplementing.
4) hs-CRP
Another important marker to keep track of if you are concerned about your heart health is C-reactive protein (CRP). Doctors use it to help predict your risk of heart disease. One study suggests that when both CRP and cholesterol levels are high, it may increase the overall risk of heart disease up to ninefold 24!
CRP is a protein that increases in response to chronic stress (lack of sleep, emotional issues, smoking, alcoholism, diabetes, nutritional deficiencies, etc.). It’s a great measure of chronic inflammation in your body.
5) LDL Particle Number and Size
Concerned about heart disease? You may be checking your cholesterol levels regularly (if you are not, you should be). But what about your LDL particle number?
LDL particles transport cholesterol in the bloodstream. You can think of LDL particles as cars on a highway (blood vessel) and cholesterol and fats like triglycerides as the passengers. A standard lipid panel will give you a measure of the number of passengers on the roads, but you need LDL particle number to know the number of cars. In addition, LDL particles come in different sizes, with large particles able to carry more cholesterol (buses and SUVs) than small particles (2-seaters) 25.
Why do LDL particle number and size matter?
For decades, reducing LDL cholesterol has been the primary target for doctors in treating and preventing heart disease. However, researchers found that almost 50% of people who have a heart attack have normal LDL cholesterol levels! In addition, in clinical trials with LDL cholesterol-reducing drugs (statins), a substantial number of patients taking these drugs continue to have heart attacks and strokes 26, 27, 28.
This has led researchers to look for other measures, such as LDL particle size, that could better predict heart disease risk and serve as a better treatment target than LDL cholesterol.
That’s because, while small LDL particles carry less cholesterol than the larger particles, they are linked with a greater risk of hardening of the arteries (atherosclerosis) and heart disease than large LDL particles, and even LDL cholesterol 29, 30, 31, 32, 33, 34, 35.
Work with your doctor to find out if testing LDL particles makes sense in your particular case.
6) Testosterone (Free or Bioavailable)
Testosterone levels decline as we age, and men and women alike are affected. This hormone protects men from obesity, depression, osteoporosis, and heart disease. Similarly, low levels have been linked with decreased libido and well-being in women 36, 37, 38.
Now, you may have been testing just your total testosterone. But total testosterone doesn’t tell the whole story. This is because it’s only the unbound (bioavailable) testosterone that works its magic in your body. Both free and total testosterone levels peak in the late 20s and decline from then on in both men and women. However, SHBG (sex hormone binding globulin), a protein that binds testosterone making it inactive, increases with age. This means that free testosterone levels will decline more dramatically with age than total testosterone levels 39, 40.
Free testosterone levels are less often measured than total testosterone because it’s a more expensive and difficult test to perform. However, if you have symptoms of low testosterone (weakness, fatigue, depression, irritability, low libido, decreased muscle mass, insomnia, bones that decrease in density) but have normal total testosterone levels, it’s definitely a test worth getting 41.
7) Estradiol
Estradiol is important for female and male fertility, brain and thyroid function, bone health, and maintaining a healthy weight.
Studies suggest that people with low estradiol levels can have an impaired stress response and may be more susceptible to stress 42. Low levels increase the risk of osteoporosis and bone fractures in men and women alike 43, 44. In addition, there is evidence that shows low estrogen increases the risk of developing heart disease and metabolic syndrome 45, 46.
For women, estradiol levels decrease sharply during menopause. This decrease contributes to age-related declines in memory and learning 47. In addition, one study showed that post-menopausal women with lower estrogen levels tended to gain weight, but those who had hormone therapy did not 48.
On the other hand, high estrogen levels can decrease sex drive in men. They also may increase the risk of stroke and cancer (especially breast cancer in women) 49, 50.
Hormones control a lot of different functions in our bodies, but we often don’t test them until things become serious. It may be a good idea to check your hormone levels once in a while to make sure everything is in order
30) Tests linked

Testing for amount and kind of brain cells by evaluating R2t* signal from MRI scan
From: https://m.medicalxpress.com/news/2018-09-overlooked-mri-scans-amount-kind.html?utm_source=fark&utm_medium=website&utm_content=link&ICID=ref_fark(https://m.medicalxpress.com/news/2018-09-overlooked-mri-scans-amount-kind.html?utm_source=fark&utm_medium=website&utm_content=link&ICID=ref_fark)
Overlooked signal in MRI scans reflects amount, kind of brain cells
September 24, 2018 , Washington University School of Medicine
An MRI scan often generates an ocean of data, most of which is never used. When overlooked data is analyzed using a new technique developed at Washington University School of Medicine in St. Louis, they surprisingly reveal how many and which brain cells are present—and show where cells have been lost through injury or disease.
The findings, published online the week of Sept. 24 in Proceedings of the National Academy of Sciences, eventually may lead to new ways to diagnose Alzheimer's disease, multiple sclerosis, traumatic brain injury, autism and other brain conditions through a simple brain scan.
"There's no easy way to detect the loss of neurons in living people, but such loss plays a role in many neurological diseases," said Dmitriy Yablonskiy, Ph.D., a professor of radiology at the university's Mallinckrodt Institute of Radiology, who directed this study together with Marcus Raichle, MD, a professor of radiology and the Alan A. and Edith L. Wolff Distinguished Professor of Medicine. "We've shown in the past that there's a signal that goes down in parts of the brain in people with Alzheimer's disease, multiple sclerosis and traumatic brain injury, but we didn't know what it meant. Now, we know it means neurons have died in those areas."
Most researchers studying brain function with MRI are only interested in a small portion of the MRI signal. They want to see how the MRI signal changes when a person performs a task, not what stays the same. Researchers trying to understand vision, for example, focus on the signal variation due to the brain activity when a person looks at a picture, and discard the parts of the signal that hold steady. But that is like looking at the waves along the surface of the ocean, and ignoring the mass of water beneath.
Yablonskiy, Raichle and colleagues including Jie Wen, Ph.D., an instructor in radiology and the study's first author, Manu Goyal, MD, an assistant professor of radiology and of neurology, and Serguei Astafiev, Ph.D., a senior scientist in psychiatry, decided to find what the rest of the ocean could tell us about how the brain works.
They analyzed the background data on an MRI scan and found a signal, which they called R2t , that remained largely unchanged when people performed tasks but varied across parts of the brain. Then, they compared the R2t signal with data from the Allen Human Brain Atlas, which maps genes active in various areas of the brain. The researchers found three sets of gene networks that tracked with the R2t signal—the genes were more active where the signal was strong, and less active where the signal was weak. These groups of genes, it turned out, reflected the different kinds and numbers of brain cells, and the extent of connections between them.
In other words, this quick new MRI scan gave the researchers all they needed to know to determine how densely packed and interconnected the neurons are in any part of the brain. This information could help us understand how a person's brain develops and changes from infancy to old age, and how we build memories and learn. It could also give clues to brain illness or injury.
"We did some studies on traumatic brain injury where we found some areas of the brain are already losing neurons even though the standard scans show nothing," Yablonskiy said.
The researchers also applied their technique to the hippocampus—the memory center of the brain—in people with Alzheimer's disease. They found that not only was the hippocampus smaller than in healthy people, but the remaining part was not healthy—it had lost cells and begun to decay.
"There are MRI scans now that can detect brain atrophy even before people show symptoms of Alzheimer's disease," Yablonskiy said. "Our technique can show the brain degrading even before it begins to atrophy."
Yablonskiy and colleagues are now working on applying their technique to brain diseases and disorders including Alzheimer's, schizophrenia, multiple sclerosis and autism, as well as to understanding how a healthy brain develops and grows.
"We've developed a method that takes a six-minute scan and tells you what types of cells are there and how extensively they're connected," Yablonskiy said. "As babies develop, neurons start growing, they connect with each other, they start forming memories. Nobody really knows how this is done. But this method could help us understand normal development, as well as how brain diseases develop."
More information: Jie Wen el al., "Genetically defined cellular correlates of the baseline brain MRI signal," PNAS (2018). www.pnas.org/cgi/doi/10.1073/pnas.1808121115
Chronic Infections Testing
Mycoplasma
Fom: 'Chronic Fatigue Syndrome, A Roadmap for Testing and Treatment' https://sites.google.com/site/cfstestingandtreatmentroadmap/home
Mycoplasma pneumoniae IgM and IgG antibodies. Dr A Martin Lerner only considers a ME/CFS patient to have a persistent Mycoplasma pneumoniae infection if their titer is 1:600 or more (Lerner uses LabCorp for testing).1(http://www.treatmentcenterforcfs.com/documents/MECFSTreatmentResourceGuideforPractitioners.pdf)
Mycoplasma Roles in Disease + Treatment, Prevention - SelfHacked https://selfhacked.com/blog/mycoplasma-infection
Patient symptoms, physical examination, radiology procedures and laboratory findings along with additional serologic and culture tests lead to an accurate diagnosis 1(https://www.ncbi.nlm.nih.gov/pubmed/3737868),153(https://www.ncbi.nlm.nih.gov/pubmed/20094751).
Laboratory Diagnosis of Mycoplasmas
Culture
Culturing *M. hominis* and *U. urealyticum*is relatively easy from urogenital specimens 154(http://jmd.amjpathol.org/article/S1525-1578%2812%2900143-2/fulltext#sec2).
A culture of *M. pneumoniae* from clinical samples such as nose and throat swabs or sputum was considered standard for diagnosis several years ago 155 (http://jcm.asm.org/content/37/1/14.full).
However, the organism usually takes 2 to 3 weeks to grow, it requires specialized and expensive growth media, and the sensitivity of cultures may be as low as 60-70% 156 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1840889/).
Therefore, the culture method is rarely used for routine diagnosis of *M. pneumoniae* infections in specialized laboratories and should be done for epidemiological reasons 156 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1840889/).
Culture is rarely successful for *M. genitalium*154 (http://jmd.amjpathol.org/article/S1525-1578%2812%2900143-2/fulltext#sec2).
Serology
Serologic tests are simple and very often used to diagnose *M. pneumoniae* respiratory infections 157(https://www.ncbi.nlm.nih.gov/pubmed/17040871).
Serologic tests measureantibodies specific for *M. pneumoniae* to show the presence of infection 157 (https://www.ncbi.nlm.nih.gov/pubmed/17040871).
In all serologic tests, two blood specimens are collected 2 – 4 weeks apart, one taken in the acute and one in the convalescent stage of the illness. A fourfold rise in antibody level (titer) indicates recent infection 158 (https://www.ncbi.nlm.nih.gov/pubmed/12667235).
Serologic tests include:
* Complement fixation test
Antibody levels do not peak until 4 – 6 weeks after infection. Since antibodies may persist for up to 1 year, a sustained high level of antibodies does not necessarily indicate a current infection 155(http://jcm.asm.org/content/37/1/14.full).
* Cold agglutinin test (frequently used to confirm the diagnosis)
Approximately 30% – 60% of patients with *M. pneumoniae* infection develop cold agglutinins (IgM(https://selfhacked.com/blog/immunoglobulin-m/) antibodies to the I antigen of red blood cells(https://selfhacked.com/blog/increase-decrease-red-blood-cells/)).
This test is not specific since positive results can be seen in infectious mononucleosis, influenza, cold agglutinin disease, and leukemia. However, if present in a patient with clinical signs of *M. pneumoniae* infection, a presumptive diagnosis can be made 159(https://www.cdc.gov/pneumonia/atypical/mycoplasma/index.html).
* ELISA (Enzyme-Linked Immuno Assay) and IFA(immunofluorescence assays)
ELISA is used for the detection of IgM (shows the presence of acute infection) and IgG (shows prior exposure, remains positive for years) antibodies 160(https://www.ncbi.nlm.nih.gov/pubmed/9286066).
Antibodies can be detected after about 1 week of illness, and peaks at 3 – 6 weeks and then declines gradually.
Molecular Methods
Development of molecular methods such as polymerase chain reaction (PCR) assays improved diagnosis of *Mycoplasma*infection in pediatric and adult patients 161(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC104575/),162(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC84154/).
Many studies have described the use of different molecular methods among which real-time PCR has both high sensitivity (true positive rate) and high specificity (true negative rate) 153(https://www.ncbi.nlm.nih.gov/pubmed/20094751).
Real-time PCR may detect *Mycoplasma*in 60 – 100% of people with the infection, and report an absence of infection in 96.7 – 100% of healthy people. In practical terms, this means that the PCR technique is extremely unlikely to report an infection in someone who doesn’t have one, but it has up to a 40% chance of reporting no infection in someone who is infected 163(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC193789/).
The PCR technique is practically the only method for detection of*M. genitalium* 164(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC269700/).
Diagnosis is made only through nucleic acid amplification testing (NAAT), but there are no commercially available diagnostic tests 165(https://www.cdc.gov/std/treatment/2010/std-treatment-2010-rr5912.pdf)
Blood looked at under microscope
EBV Testing
From: 'Chronic Fatigue Syndrome, A Roadmap for Testing and Treatment' https://sites.google.com/site/cfstestingandtreatmentroadmap/home
Epstein-Barr virus antibodies. Dr A Martin Lerner says ME/CFS patients have an active EBV infection when there are elevated ELISA antibodies in theEBV IgM VCA test and/or the EBV EA diffuse test.1(http://www.treatmentcenterforcfs.com/documents/MECFSTreatmentResourceGuideforPractitioners.pdf) 2(https://www.dovepress.com/subset-directed-antiviral-treatment-of-142-herpesvirus-patients-with-c-peer-reviewed-article-VAAT)
Similarly, Professor Jose Montoya considers that when the Quest EBV IgG VCA(http://www.questdiagnostics.com/testcenter/TestDetail.action?ntc=38015)test result is 1:640 or higher and/or the Quest EBV IgG EA(http://www.questdiagnostics.com/testcenter/TestDetail.action?ntc=15447) test result is 1:160or higher, this is indicative of an active EBV infection.1(http://www.ncbi.nlm.nih.gov/pubmed/23080504)
Note that:
EA = early antigen
VCA = virus capsid antigen (also denoted by CA)
EBNA = Epstein-Barr nuclear antigen
Lymphocyte subset panel. If this test shows elevated CD8 T-cells, this can indicate an ongoing viral infection with EBV or cytomegalovirus, which both raise CD8 T-cells.1(http://www.sydpath.stvincents.com.au/tests/ImmunoFrames/lymphocytosis.htm)
Human herpes virus six HHV-6
valganciclovir showed promising results in a subset of CFS patients with elevated IgG antibody titers against human herpesvirus 6 (HHV- 6) and Epstein Barr virus (refering to Randomized clinical trial to evaluate the efficacy and safety of valganciclovir in a subset of patients with chronic fatigue syndrome https://pubmed.ncbi.nlm.nih.gov/23959519
From: 'Chronic Fatigue Syndrome, A Roadmap for Testing and Treatment' https://sites.google.com/site/cfstestingandtreatmentroadmap/home
HHV-6 antibodies.Dr A Martin Lerner says that when tested using the LabCorp HHV-6 IgM(https://www.labcorp.com/test-menu/28471/human-herpesvirus-6-hhv-6-igm) test and the LabCorp HHV-6 IgG(https://www.labcorp.com/test-menu/28461/human-herpesvirus-6-hhv-6-antibodies-igg) test, antibody titers of 1:160 or higher are indicative of an active HHV-6 infection.1(http://www.treatmentcenterforcfs.com/documents/MECFSTreatmentResourceGuideforPractitioners.pdf) 2(https://www.dovepress.com/subset-directed-antiviral-treatment-of-142-herpesvirus-patients-with-c-peer-reviewed-article-VAAT)
Alternatively, Professor Jose Montoya considers that when tested using the Quest HHV-6 IgG IFA test(http://www.questdiagnostics.com/testcenter/BUOrderInfo.action?tc=101426&labCode=QSO), an HHV-6 IgG antibody titer of 1:320 or higher is indicative of an active infection.1(http://www.ncbi.nlm.nih.gov/pubmed/23080504)
Further info:
HHV-6 Foundation: Viral Testing(http://hhv-6foundation.org/patients/hhv-6-testing-for-patients)
Enterovirus
The reverse transcription– polymerase chain reaction (RT PCR) technique is widely applied to test for the presence of enterovirus genomes and is the method of choice for identifying virus infection in many countries. This technique is very sensitive and specific, particularly in diagnosing CNS infections from cerebrospinal fluid specimens, and has become the ‘gold standard’ of diagnosis, surpassing viral culture. Enterovirus RNAs have also been detected in myocardial biopsies from patients with myocarditis and dilated cardiomyopathy, in muscle of people with inflammatory muscle disease and chronic fatigue syndrome, and in brain biopsies. The significance of these findings is not clear, as infectious virus can rarely be isolated and viral antigen cannot be detected. Highly conserved sequences of the 5′ end of enterovirus genomes have allowed the design of PCR primers detecting most enterovirus RNAs. As the EV22 genome is very different from that of the other enteroviruses (see earlier), tailor made primers have to be added in a multiplex RT PCR to include detection of these viruses, which cause infections particularly in neonates and infants. A modified RT PCR procedure can differentiate between wild type and vaccine derived poliovirus infections. Modern sequencing techniques (Deep, Massive parallel or Next Generation sequencing) offer the possibility of sequencing without either cell culture isolation, PCR or knowledge of the sequence to be sought and are having a major impact on diagnosis of enterovirus and other infections, and environmental surveillance
M.E. tests (in brief https://www.hfme.org/metests.htm
M.E. tests (in brief)
M.E. is a distinct, recognisable disease entity with several unique features that is not difficult to diagnose within just a few weeks of onset. Although there is as yet no single test which can be used to diagnose M.E. there are (as with Lupus, multiple sclerosis and ovarian cancer and so on) a series of tests which can confirm a suspected M.E. diagnosis with confidence. Virtually every M.E. patient will also have various abnormalities visible on physical exam. If all tests are normal then a person does NOT have M.E.
M.E. tests
M.E. is a distinct, recognisable disease entity that is not difficult to diagnose and can in fact be diagnosed relatively early in the course of the disease, within just a few weeks, providing that the physician has some experience with the disease. There is just no other disease that has all the major features of M.E.
Objective evidence of quantifiable organic abnormalities in M.E. patients has existed since the 1950s. As with a wide variety of illnesses – lupus, multiple sclerosis, and ovarian cancer for example – there is as yet no single test which can diagnose M.E. in all patients. Therefore, like these other illnesses, M.E. must be diagnosed by taking a detailed medical history, noting the type and severity of symptomatology and other characteristics of the illness and the type of onset of the symptoms. (An acute or sudden onset of symptoms is always seen in M.E. and this onset type rules out a wide variety of other illnesses associated with gradual onset). A series of tests may also then be necessary to rule out or confirm a suspected M.E. diagnosis.
One cannot test for ‘CFS’ but M.E. is not the same thing as ‘CFS’ (or ‘ME/CFS.’) The presence or absence of ‘fatigue’ is largely irrelevant in determining an M.E. diagnosis except in that its presence may of course make the diagnosis of a large number of well-known fatigue causing illnesses considerably more likely (depression, vitamin deficiency or malignancy for example) (Hyde & Jain, 1992). M.E. is not a diagnosis of exclusion or an untestable disease. Tests will only all be normal in M.E. patients – as with all illnesses – if the wrong tests are conducted, or if those tested do not in fact have M.E. (Hyde 2007, [Online]) (Hyde 2006, [Online]) (Chabursky et al. 1992, p.22).
Contrary to common disinformation erroneously linking M.E. with ‘CFS,’ it is not mere ‘fatigue’ that defines M.E. but central nervous system (CNS) dysfunction. M.E. represents a major attack on the CNS by the chronic effects of a viral infection which targets the brain: an enterovirus. As M.E. expert Dr Byron Hyde explains:
The one essential characteristic of M.E. is acquired CNS dysfunction. A patient with M.E. is a patient whose primary disease is CNS change, and this is measurable. We have excellent tools for measuring these physiological and neuropsychological changes: SPECT, xenon SPECT, PET, and neuropsychological testing (2003, [Online]).
Tests which together can be used to confirm an M.E. diagnosis include:
SPECT and xenon SPECT scans of the brain.
MRI scans of the brain.
PET scans of the brain.
EEG/QEEG brain maps.
Neurological examination. Neuropsychological testing.
The Romberg test.
Immune system tests.
Insulin levels and glucose tolerance tests.
Erythrocyte Sedimentation Rate (ESR) tests.
Circulating blood volume tests.
24 hour Holter monitor testing.
Tilt table examination and standing/sitting/reclining blood pressure tests.
Exercise testing and chemical stress tests.
Physical exam.
These tests are the most critical in the diagnosis of M.E., although various other types of tests are also useful.
M.E. expert Dr Byron Hyde’s Nightingale Definition of M.E. also now makes diagnosis easier than ever before even for those with no prior experience in diagnosing M.E. This is a pure M.E. definition and, most importantly, it defines M.E. as testable (Hyde 2007, [Online]) (Hyde 2006, [Online]) (Hyde 2003, [Online]) (Dowsett 2001a, [Online]) (Dowsett 2000, [Online]) (Hyde 1992 p. xi) (Hyde & Jain 1992 pp. 38 - 43) (Hyde et al. 1992, pp. 25-37) (Dowsett et al. 1990, pp. 285-291) (Ramsay 1986, [Online]) (Dowsett n.d., [Online]) (Dowsett & Ramsay n.d., pp. 81-84) (Richardson n.d., pp. 85-92).
More information
To read or download an extended and fully referenced version of the above text, please see the Testing for M.E. page.
Additional note for patients: Despite the existence of the tests for M.E. described in this paper, the unfortunate reality is that many people who suspect they have M.E. do not have access to the appropriate tests or to doctors who are able to make the diagnosis due to political interference in science (helped immeasurably by the creation of the bogus disease category of 'CFS'). See Testing for M.E.: Plan D for discussion of the ways in which patients seek a diagnosis in practice.
Additional relevant links:
For more information on all aspects of M.E. please see the (fully referenced) What is M.E.? A historical, medical and political overview paper.
For more information on the political issues facing M.E. patients please see: M.E. vs MS: Similarities and differences and Who benefits from 'CFS' and 'ME/CFS'? and M.E.: The shocking disease.
Patients given a diagnosis of 'CFS' are advised to read the following papers: The misdiagnosis of CFS, Where to after a 'CFS' (mis)diagnosis? and Why the disease category of 'CFS' must be abandoned and Who benefits from 'CFS' and 'ME/CFS'?
To read a list of all the articles on this site suitable for different readers, see the Information guides page. Guides available so far include the following: severe M.E. patients, M.E. patients, patients given a 'CFS' diagnosis (but that do not have M.E.), doctors, carers looking after M.E. patients, friends and family of M.E. patients, parents of children with M.E., members of the public who would like to know a little more about the disease, media and politicians and human rights groups.
To view a list of all HFME papers and resources, see the HFME site map page.
Extra information: Medical science vs politics
M.E. is not difficult to diagnose, or to distinguish from ‘CFS’ or any other fatiguing illnesses. M.E. is also not ‘difficult to define’ or ‘mysterious’ or ‘medically unexplained’ or a mere ‘diagnosis of exclusion.’ These are characteristics of ‘CFS’ but not of M.E.
M.E. is no more difficult to diagnose through using a series of tests than is MS. In fact, it has been suggested that M.E. diagnosis is significantly less difficult and more reliable than that of MS! We can also be a lot more certain about the cause of M.E., compared to MS. The cause of MS is hotly debated, while the fact that M.E. is caused by a virus is well established beyond doubt and there is overwhelming evidence that M.E. is caused by an enterovirus.
On a purely scientific level, we have more than enough information to reliably diagnose patients with M.E. using objective tests (and by taking detailed case notes and conducting a detailed physical exam etc.) within just a few weeks of the onset of the disease.
If the will and the funding were there, scientists could right now very easily make sure that studies contained a 100% M.E. population – just as they do with MS patients or patients with Lupus and so on. Scientifically, it would be no more difficult to do this for M.E. than with these other diseases.
The problem is not that these tests don’t exist, but that doctors – and many patients – are unaware of this information on testing, that it is not generally accepted due to the nefarious influence of political and financial vested interest groups, and that there are overwhelming financial and political incentives for researchers to IGNORE this evidence in favour of the bogus ‘CFS’ (or ‘subgroups of ‘ME/CFS’) construct, and so on.
For more information see: Testing for M.E. and Dr Hyde's The Nightingale Definition of M.E. plus Are we just 'marking time?' Why are we waiting to act when tests for M.E. exist RIGHT NOW, and the need for activism/action is so very urgent? See also: See M.E. vs MS: Similarities and differences
diffusion tensor imaging
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253
A recently developed magnetic resonance imaging technique, called diffusion tensor imaging (DTI), has become an extremely valuable tool for evaluating patients with brain injuries.
DTI enables measurement of the integrity of white matter fibre tracts making the axonal organization of the brain visible. It measures the diffusion of water molecules that prefer to diffuse along white matter fibre tracts (anisotropically) and not perpendicularly to the course of the fibre tracts (Mori and Zhang, 2006(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b62)).
Values for fractional anisotropy (FA) range between 0 and 1, with 0 standing for isotropic, lack of directional diffusion, and 1 representing anisotropic (directional) diffusion.
Factors influencing FA are myelination of fibre tracts and axonal integrity and density (Mori and Zhang, 2006(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b62); Kraus *et al.*, 2007(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b44)).
In a recent study, DTI was validated in a controlled cortical mouse TBI model using histology and electronmicroscopic analysis. The technique was able to detect perilesional white matter damage in a range of acute to subacute time points, thereby predicting the approximate time since trauma (Mac Donald *et al.*, 2007(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b53)).
DTI was also able to correlate recovery of the damaged corticospinal tract with functional improvement in a patient suffering from paraparesis after TBI (Han *et al.*, 2007(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b34)).
These remarkable abilities of DTI make it an extremely valuable tool in the evaluation of restorative and axon regenerative therapies in animal models of TBI. DTI has recently been used to document myelin-protective activities of a therapeutic antibody candidate in an animal multiple sclerosis model (Mi *et al.*, 2007(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2721253/#b57)) and is extensively used in rodent models characterized by axonal or myelin damage
Grayfield method microscopy
A new concept in optical microscopy is the grayfield method as developed by Kurt Olbrich (www.grayfieldoptical.com(www.grayfieldoptical.com)). This allows one to see detailed structures that are otherwise not even visible with conventional phase contrast microscopy. Now it is possible to observe the decomposition of live blood or the pleomorphic changes from spores or viral forms to bacteria and fungi in diseased blood
test for a jawbone infection
Jawbone Cavitation Infection
Cases of ME/CFS have occasionally been caused or worsened by infections located within the jawbone (osteomyelitis). Such infections develop inside hollow pockets within the jawbone called cavitations. Cavitations can be left in the jawbone after a tooth extraction, such as a wisdom tooth removal; and cavitations can be created as a result of osteonecrosis (the death of bone tissue due to poor blood flow to the bone).1
When these jawbone cavitations also induce facial pain, they are called NICO lesions https://en.wikipedia.org/wiki/Neuralgia-inducing_cavitational_osteonecrosis
- Jawbone cavitation infections induce the inflammatory chemokine RANTES https://en.wikipedia.org/wiki/CCL5
- as well as FGF-2 https://en.wikipedia.org/wiki/Basic_fibroblast_growth_factor Both are linked to systemic disease.
- https://pubmed.ncbi.nlm.nih.gov/23637551
- https://pubmed.ncbi.nlm.nih.gov/25987906 Increased RANTES is found in the jawbone and blood serum of ME/CFS patients.
- https://pubmed.ncbi.nlm.nih.gov/28685531 This suggests RANTES from jawbone cavitations may play a role in ME/CFS.
See this thread for more info https://forums.phoenixrising.me/threads/inflammatory-chemokine-rantes-elevated-in-jawbone-serum-of-me-cfs-patients-link-to-jawbone-cavitation-infections.53799
Stories of ME/CFS patients improving after treatment of jawbone cavitations:
- Ian's recovery story https://forums.phoenixrising.me/threads/my-recovery-story.7912/ and also here http://www.howigotbetter.com
- Stories/21/My-recovery-from-CFS-due-to-osteonecrosis-in-my-jaw.aspx
- Ian's Website http://caviscan.com/cavitations.html
- Errol's cavitations and root canal story https://forums.phoenixrising.me/threads/cavitations-and-root-canals.39121
- Dukey's recovery story https://www.reddit.com/r/cfs/comments/1kgfrg/i_was_sick_for_8_years_and_got_better_ama
Jawbone infections can be hard to detect, as they often cause only very minimal local symptoms. Yet a local infection within the jawbone can cause a condition symptomatically identical to ME/CFS.
Sometimes a jawbone cavitation infection may cause chronic facial pain, but such facial pain is not always present. Jawbone infections may also cause a sour bitter taste in the mouth, causing bad breath or even gagging.
A simple test for a jawbone infection is applying pressure with a finger on the gums to the jawbone beneath; if any area feels painful, this indicates a possible jawbone infection (though this test will not always detect a jawbone infection).
A MRI STIR scan is an accurate way to detect jawbone infections. A handheld ultrasound device called the Cavitat scanner is the best and most effective way to detect jawbone cavitations.
Panoramic dental X-rays can detect jawbone cavitations, but are not very reliable, and they require skilled interpretation by dentists experienced in detecting cavitations (very few dentists have this experience). Ordinary MRI scans or CT scans are not good at detecting jawbone cavitations.
More info on the diagnosis and treatment of jawbone cavitation infections is given here:
- Symptoms and Location of Cavitations https://tmj-facialpain.com/symptoms-location-cavitations
- The Appearance of NICO Lesions https://tmj-facialpain.com/appearance-of-nico-lesions
- Diagnosis and Treatment of Cavitational Lesions https://tmj-facialpain.com/diagnosis-and-treatment-of-cavitational-lesions
Jawbone cavitation infections come under the category of focal infections, which are defined as infections localized in a small region of the body. Focal infections within the tonsils may also lead to fatigue symptoms.
UK dental clinics which specialize in diagnosing and treating jawbone cavitation infections include: Munro-Hall Clinic (Bedford), https://www.munro-hallclinic.co.uk Tooth Fairy Holistic (Kent http://www.toothfairyholistic.co.uk/cavitations.html
Jawbone infection treatments. If you suspect you may have a jawbone cavitation infection, you may want to seek help from a dentist or maxillofacial surgeon who specializes in diagnosis and treatment of jawbone cavitations
A1) Dr. Myhill's recommendations DETECT
Useful medical tests for investigating the patient who presents with chronic fatigue
One of the things I really dislike about the Medical Profession is their power over patients. The main two ways in which they use that power is firstly by controlling the availability of tests and secondly through the power of prescription. My website allows patients to order any test they see fit. The test result comes to me as the referring practitioner; I can interpret it and write to their GP with recommendations (copy to patient). Secondly, nearly all my treatments do not require prescription drugs and so are available to all. I can also recommend a local ecologically trained physician who can advise further if necessary.
There is no simple test currently available to diagnose CFS because CFS is not a diagnosis – it is a symptom. Blood tests merely serve to exclude other diagnoses. Doctors can sometimes be very naughty – they do the routine tests which all come back as normal and the doctors then turn round and tell their patient that nothing is wrong with them. I believe that the reason so many medical tests are negative in the case of CFS patients is because doctors are looking in the wrong place. The pathology is inside cells, i.e. in mitochondria. Although cells (and therefore organs) look fine, they do not function properly. It is a bit like having a car with a flat battery – an MRI scan of a car would come back completely normal – but you try and start it and nothing would work!
However, I now believe CFS is very often a symptom of mitochondrial failure. This means when other causes have been excluded (lack of sleep, allergy, hormonal problems etc) we now have a definitive test which can tell us how disabled the CFS sufferer is, where the biochemical lesion lies and what has to be put in place to correct it. Having said that, various routine blood tests have a place in investigating a patient with fatigue and so let’s review them first.
Firstly exclude macroscopical pathology
Most patients, by the time they get to see me, have had all the routine tests done. These tests just test for macroscopic pathology such as major organ failure (anaemia, heart disease, cancer, liver failure, kidney failure and some gut problems). They do not test for minor organ failures (such as partial thyroid gland failure, partial adrenal gland failure, mild liver damage, poor ability to detox). None of these tests look for poor function of the brain or brain damage, nutritional tests are often absent or limited, hormone tests are usually incomplete and there are virtually no tests of micropathological function.
Having said that, there are often mild abnormalities in standard tests which have not been picked up on by the GP or consultant, but which are clinically important for the CFS sufferer. Results are given by a figure and there should also be a reference range next to this figure – that tells you if you are inside or outside the reference range. This reference range often varies from one lab to another.
The basic tests that most doctors do for their patients with chronic fatigue are:
• Haematology (full blood count – red cells, white cells and platelets)
• Inflammation in the blood – ESR, C reactive protein, plasma viscosity.
• Biochemistry (liver and kidney function)
• Blood sugar level
• Urine testing (for infection or kidney damage)
• Faecal occult bloods (looking for bleeding from the gut)
• Thyroid stimulating hormone (only looks for primary thyroid failure – most thyroid problems in CFS are secondary to poor pituitary function)
• Ferritin (iron), B12, folic acid and calcium
• Perhaps a serum magnesium – which is a completely useless test! This is because serum levels are maintained at the expense of levels inside cells. A serum magnesium is just an ITU (Intensive Therapy Unit) test!
• Autoantibody tests for autoimmunity.
Common abnormalities that can be shown by routine tests
The mild abnormalities I always look for in CFS in the above tests are:
• Low or low normal white cell count – can be a sign of poor immune function which most commonly is secondary to nutritional deficiencies, such as low zinc, low magnesium, low B vitamins, low essential fatty acids.
• Low or low normal platelet count – can be a sign of toxic stress
• Low MCV (mean corpuscular volume) suggesting iron or copper deficiency. Low iron is suggestive of HYPOCHLORHYDRIA, in which case other mineral deficiencies are also likely.
• High MCV suggesting B12, folic acid or HYPOTHYROIDISM
• A high blood sugar or a low blood sugar suggests there may be a tendency to HYPOGLYCAEMIA (a pre-diabetic tendency). A normal blood sugar tells you very little! Normal ranges of blood glucose have been changed because so many people now have carbohydrate intolerance. A normal blood sugar should be between 4-6mmol/l. High blood sugar is now associated with toxic stress because chemicals cause insulin resistance.
• Low potassium. Potassium varies according to diet! Low potassium means there is a lack of vegetables in the diet. Bananas may be rich in potassium but they are high glycaemic index, so beware!
• High normal bilirubin – may be Gilbert’s syndrome suggesting poor ability to detoxify.
• High normal or abnormal liver enzymes – suggesting liver damage, usually from chemicals, or poor nutritional status.
• High urea or creatinine suggesting dehydration
• Low urea or creatinine suggesting low protein diet
• Low glomerular filtration rate suggesting poor kidney function – could be due to allergy or toxic damage but may indicated poor mitochondrial function.
• A TSH tells you very little about thyroid status! It is essential to see the actual level of thyroid hormones in the blood.
• Low levels of B12 can be due to HYPOCHLORHYDRIA or MALABSORPTION
• High uric acid can point to poor ANTIOXIDANT status. See GOUT.
• Raised cholesterol could mean low levels of vitamin D or hypothyroidism.
• Low levels of calcium likely to mean low levels of vitamin D.
The routine tests which I nearly always do initially and which have important implications for management
1. Mitochondrial function profile (p. 17 ) – this is a batch of tests to identify the mitochondrial problem. This test has important implication for treatment; this test includes:
- ATP profiles – looks at levels of ATP, how well energy is released from ATP, the rate of production of ATP from ADP and movement of ATP and ADP across mitochondrial membranes (translocator protein function - could be blocked by toxins or pH changes). Also gives us an objective measure of the level of disability.
- Plasma cell-free DNA – a measurement of cell damage and antioxidant status in CFS
- Red cell NAD levels – a measure of the efficiency of Kreb’s citric acid cycle. Levels can be corrected with niacinamide 500mgs daily and acetyl L carnitine.
- Co-enzyme Q10 levels – the most important antioxidant inside mitochondria. In CFS levels are nearly always deficient
- Superoxide dismutase – three types measured, indicates levels of zinc, copper and manganese, also gene studies to give an indication of toxic damage. SODase is a major antioxidant in all cells.
- Red cell magnesium – done as part of the ATP profile or can be done separately.
- Glutathione and glutathione peroxidase (also indicates selenium status).
2. Thyroid function profile (free T4, Free T3 and TSH).
More esoteric tests which have implications for management
- Microrespirometry - looks in detail at ADP to ATP conversion (see sample result on p. 20
- Further investigation of poor translocator protein function Translocator protein studies (p.21)
- Cardiolipin studies looks at the structure of mitochondrial membranes (p. 22 )
- Calcium studies – calcium levels inside cells often too high.
- Adrenal stress profile – salivary levels of cortisol and DHEA over 24 hours
- Salivary Melatonin levels – it is common to get poor melatonin production and therefore poor sleep in CFS. This is a further reflection of the inadequate HPA axis in CFS.
- Lactate dehydrogenase studies – if there is evidence of cell damage, this indicates where the damage is coming from eg liver or muscle.
- Red cell Carbonic anhydrase – indicates hyperventilation
When gut symptoms suggest tests
- Gut fermentation test – to look for evidence of fermentation by bacteria or yeast. Irritable bowel syndrome may be caused by food allergy or gut dysbiosis. Low levels of short chain fatty acids can mean insufficient probiotics in the gut.
- Salivary VEGF test for hypochlorhydria – if there are symptoms of poor digestion or “too much acid”.
- Urine hydrogen sulphide test – some people ferment food to produce hydrogen sulphide and this can inhibit mitochondrial function. See HYDROGEN SULPHIDE AND CFS, FERMENTATION IN THE GUT AND CFS
- Parasitology at the London School of Hygiene and Tropical Medicine – detects worms, amoebae, giardia, blastocystis hominis.
- Comprehensive Digestive Stool Analysis – ability to digest and gut flora. Parasitology can also be done as part of this test.
- Short chain polypeptides – if the result is abnormal, it suggests leaky gut syndrome.
- Early morning Short chain fatty acids and/or tests of Fructose intolerance – indicate a tendency to HYPOGLYCAEMIA
Looking for toxic stress
- Fat biopsy for pesticides and/or for volatile organic compounds (VOCs). A fat biopsy is very easy to do – easier than a blood test! A green needle and 10ml syringe is used – the green needle is pushed into buttock fat, suction applied with the syringe, then needle withdrawn. The amount of fat inside the bore of the needle is sufficient to do the test.
- Sauna sweat test.
- Kelmer test (urine test) for mercury load – anybody with mercury fillings will have mercury on board – the question is how much? How hard does one have to work to get rid?
- Translocator protein studies.
- DNA adducts – looks to see if toxins have stuck onto DNA – if so, this is a pre-cancerous condition. This is a useful test to work out how much damage has been done to the body as a result of toxic stress and therefore how much work has to be put into a detox regime. If abnormal then it should be repeated following a detox regime to make sure there are improvements.
Looking for sensitivity to chemicals
- Lymphocyte sensitivity test for chemicals, heavy metals, silicones, VOCs. This is helpful if you suspect that you are reacting to one/some/all of those substances, in other words you are sensitive to them. I often use this where there is a silicone implant to help decide if it should be removed. Where there is sensitivity, there will be toxicity, and vice versa. Indeed, multiple chemical sensitivity is usually triggered by toxicity.
More recently John McLaren-Howard has developed similar tests to diagnose electrical sensitivity.
Evidence of damage to cells
- Plasma cell-free DNA – this is nearly always abnormal in CFS and can be for any one of the following reasons:
-
- There is poor antioxidant status (see Co-enzyme Q10, SODase),
-
- There is ongoing toxic stress (such as from pesticides, volatile organic compounds, heavy metals etc),
-
- There is immune activation (as for example in acute infection),
-
- There is very poor mitochondrial function (see mitochondrial function) score but the patient is forced to do some muscular activity just in order to live.
-
- The patient is not pacing well – i.e. pushing too hard and this is resulting in cell damage. However some people who are very disabled have no choice – just the energy required to exist will cause tissue damage. So people with the worst mitochondrial function score often have high cell free DNAs even though they are doing almost nothing.
This can be investigated further with LDH studies, which tells us where the damage is coming from.
Tests not worth doing either because the result is worthless or the test is unreliable
Tests for food allergy – at best these are 70% accurate.
B12 – occasionally picks up pernicious anaemia, but regardless of the level I almost routinely prescribe injections to improve fatigue syndromes. B12 provides “instant” antioxidant cover. It has no toxicity. I like to see blood levels above 2000 (at this levels many GPs recommend stopping treatment!).
Hair analysis – does not reliably detect heavy metal toxicity and can be very misleading with trace elements. Useless for allergies.
There is no point doing the tests I list below before starting nutritional supplements. This is because deficiencies are pandemic!
B vitamin profile
Red cell Magnesium
Essential fatty acids
Vitamins A, C and E
Vitamin D3 levels (a bit expensive!)
There is no point doing a test unless it has implications for management – either one needs the test to make the diagnosis or to determine management options. Always ask this question when requesting a test or it is money wasted!
Tests ask very specific questions – there are literally hundreds of tests available, it is a case of picking the right one dependent on the symptoms and signs. If your doctor does not ask the right questions with his tests, then the results will not be relevant to recovery.
Where there are symptoms pertaining to a specific area such as the gut, tests need to be done to exclude ulcer disease, gall bladder disease, cancer and so on.
My general principle for tests of nutritional status is that I always advise sufferers to continue with their usual nutritional supplement programme when doing a test of nutritional status. This way I can assess if the current nutritional regime is adequate or not. I simply need to know what the patient is taking when interpreting such tests of nutritional status.
In CFS the problem is micro-pathology (intracellular, immune and biochemical problems), i.e. problems inside cells and on cell membranes. This is why standard medical tests do not come up with abnormalities.
A vital test in chronic fatigue syndrome
The central problem of chronic fatigue syndrome is mitochondrial failure resulting in poor production of ATP. ATP is the currency of energy in the body and if the production of this is impaired then all cellular processes will go slow. It is not good enough to measure absolute levels of ATP in cells since this will simply reflect how well rested the sufferer is. The perfect test is to measure the rate at which ATP is recycled in cells and this test has now been developed by the brilliant medical biochemist Dr John McLaren-Howard. He calls it “ATP profiles”. It is a test of mitochondrial function.
Not only does this test measure the rate at which ATP is made, it also looks at where the problem lies. Part A measures levels of ATP in the cell. Release of energy from ATP is a magnesium dependent process and the first part of the test studies this aspect (I refer to this aspect of the test as Part A– this corresponds to the labels in Figure 3 below).
The second aspect of the test (Part B) measures the efficiency with which ATP is made from ADP in the mitochondrion. If this is abnormal then this could be as a result of magnesium deficiency, of low levels of Co-enzyme Q10, low levels of vitamin B3 (NAD) or of acetyl L-carnitine. It is also possible that ADP to ATP conversion is blocked and this is also seen on this part of the test.
The third possibility is that the protein which transports ATP and ADP across mitochondrial membranes is impaired and this is also measured (Part C).
Acetyl-L-carnitine
Fuel
CoQ10
Part C– crossing mitochondrial membrane Part A – ATPlevels
ATP
Mitochondrion
NAD
Magnesium
ADP
Energy
Oxygen
Part B - ADPto ATPconversion
Figure 3
The joy of the ATP profiles test is that we now have an objective test of chronic fatigue syndrome which clearly shows this illness has a physical basis. This test clearly shows that cognitive behaviour therapy, graded exercise and anti-depressants are irrelevant in addressing the root cause of this illness.
To get the full picture I recommend combining this test with measuring levels of the front line anti\- oxidants Co-enzyme Q10, Superoxide dismutase (SODase), and glutathione peroxidase together with NAD (a functional test of vit B3 levels) and L-carnitine. See ANTIOXIDANTS.
Cell-free DNA is very useful because it measures tissue damage. When cells are damaged and die, they release their contents into the blood stream – cell-free DNA measures the extent of this damage. I believe this equates to how ill one feels – or malaise. The levels which come back are similar to those from patients recovering from major infections, trauma, surgery or chemotherapy – so this test puts CFS firmly in the realms of major organic pathology. Where there is tissue damage, the immune system is activated for healing and repair – this requires energy and can produce distressing symptoms such as PAIN and INFLAMMATION.
SODase is an important antioxidant which mops up the free radicals produced in all the inefficient chemical reactions in the cells. Dr McLaren-Howard also looks at the genes which code for the different types of SODase! It is common to find blockage or polymorphisms typical of toxic stress. See INFLAMMATION.
Dr McLaren-Howard has recently developed a serum L-carnitine test and made it available in September 2009. I have now included it in the Mitochondrial Function Profile.
In fact, all of these above blood tests have now been combined as a Mitochondrial function profile and can be ordered from my practice – see details below p. To order any test123.
One other important co-factor in the production of energy in cells is D-ribose. It is used up so quickly by cells that measuring levels is unhelpful, but low levels of ATP imply low levels of D- ribose. .
Therefore, the cost of the Mitochondrial function profile, which will now include the mitochondrial function studies (ATP profiles), levels of Co-enzyme Q10, glutathione peroxidase, zinc copper SODase, manganese SODase and extracellular SODase together with NAD levels, cell\- free DNA and L-carnitine is £225, plus £70 for the letter of interpretation to the GP.
John McLaren-Howard now has specialist equipment to refine these tests further, particularly in respect of oxidative phosphorylation. See Practical Details p. 123 should you wish to order this test
Implications for Treatment
Many patients I see get well with my standard work up with respect to vitamins and minerals, diet, pacing and sleep, i.e. the foundations of recovery. All these things must be put in place to repair and prevent ongoing damage to mitochondria so allowing them to recover. For mitochondria to recover they need all the essential vitamins, minerals, essential fatty acids and amino acids to manufacture the cellular machinery to restore normal function. The mitochondrial function tests then allow us to identify lesions which can be corrected by attention to nutritional supplements, improving antioxidant status, detoxing, hyperventilation or whatever. CFS sufferers have limited reserves of physical, mental and emotional energy and this test allows us to direct those energies into the most fruitful line of approach. (see p. 24 for the interpretation of the mitochondrial function test results)
Examples of some test results
ATP profiles
This patient has low levels of ATP (1), low magnesium (2), poor conversion of ADP to ATP (3) with blockage of the active sites (4) together with poor translocator protein function (5) – no wonder there is severe fatigue!
A closer look at oxidative phosphorylation with micro-respirometry studies chart
A closer look at translocator protein studies chart
Cardiolipin Studies – a closer look at mitochondrial membranes chart
Anti-oxidant studies chart
A2) Thyroid and Adrenals
A lab test for identifying adrenal fatigue is a saliva test. It’s important to take samples of the saliva at different times of the day in order to establish the true cortisol rhythm and DHEA levels. Samples are taken in the morning (6am-8am), midday (12pm-1pm), late afternoon (4pm-5pm) and nighttime (10pm-midnight). Cortisol should be at the highest in the morning and the lowest at night.
Taking your body temperature when you wake up in the morning and finding that your temperature is below 97.8 degrees Fahrenheit can help to detect adrenal and/or thyroid problems
Please note that adrenal fatigue (exhaustion) has three different stages before it reaches failure. People in stage one of adrenal fatigue have a high amount of cortisol overall and at least one cortisol reading that is higher than it should be. An overall high count and a spike at an inappropriate time of the day indicates there is a problem. Cortisol must be kept under control because it eats muscle when at an excessively high level.
Stage two of adrenal fatigue is commonly misdiagnosed and can even go undiagnosed entirely. This primarily happens because a person’s total cortisol level is normal in stage two! The key indicators in this stage are the DHEA level and a low level of cortisol in the morning, midday, or afternoon. The trouble with properly identifying adrenal fatigue in stage two is that cortisol levels are often normal at night and the overall reading usually averages in the normal range as well. Again, cortisol should be at the highest in the morning and lowest at night. If a client is experiencing low cortisol levels when it should be at its peak, there is a problem.
Stage three of adrenal fatigue is the easiest to identify. The DHEA level is low and most cortisol levels are borderline low or low throughout the day. And of course, the total cortisol level is low as well. Low nighttime cortisol is a major marker for late stage three adrenal fatigue.
There are some tests that can be taken at home which tell you if adrenal fatigue is part of your problem. For example, go into an indoor room that is away from the natural sunlight (a room with no windows or, at the very least, with the shades lowered) with a small flashlight. Shine the light at a 45-degree angle towards your eye and you will see your pupil shrink (the pupil is the black center of your eye). The light of the flashlight will cause the pupil to shrink and it should remain constricted while the light is being pointed at your eye. You likely have adrenal problems if you see your pupil pulsing (alternating between being bigger and smaller). While this simple test shouldn’t replace an actual diagnosis, it does point to what could be the source of your issues and it would be something to further investigate with a health professional.
Another test is I recommend involves an electronic blood pressure cuff (the Omron® blood pressure cuff can be purchased online for around $50-60). Place the blood pressure cuff on your arm as you normally would when measuring your blood pressure but lay down on your back for 5-10 minutes before taking the measurement. Have someone write down what the measurement is. Then stand up as fast as you can, take your blood pressure again, and write down that number. You are looking for the difference in blood pressure numbers between lying down and standing. This is called an orthostatic measurement.
To illustrate, let’s say someone’s measurement is 120/80 when laying down and jumps to 130/85 immediately after standing. That’s good! The body naturally increases blood pressure when standing because gravity places more demands on our bodies. It is normal and healthy to see both the systolic rate (the top number) and the diastolic rate (the bottom number) increase 5-10 mmHg when going from laying down to standing. What if the rate doesn’t go up? For example, let’s say a person’s lying down blood pressure rate is 120/80 but it goes down to 110/80 immediately after standing. That’s bad. When this occurs, I often find the person has adrenal dysfunction and toxicity issues. Similarly, people who become light headed or dizzy when rising from a lying or sitting position also tend to have adrenal dysfunction and toxicity issues.
Conventional practitioners generally determine if a patient has thyroid problems by testing their TSH level. What I find interesting is that TSH (thyroid stimulating hormone) is not even manufactured by the thyroid! It’s actually manufactured by the pituitary gland and is meant to communicate with the thyroid. Low TSH indicates hyperthyroidism (overactive) and high TSH suggests hypothyroidism (low functioning).
Conventional testing says that “normal” values for TSH are typically .5 to 5 µ/mL. I believe that is too big of a range. I would not use the conventional bell curve that is used to determine the “normal range.” Instead, I recommend all practitioners and those who suspect they have thyroid dysfunction to use the optimal values that are between 1.8 and 3 µ/mL. The bell curve used to show the “normal” range is established by sick people! Think about it: who has their TSH tested? People who are displaying symptoms of having a dysfunctioning thyroid! To be on the edges of what is considered normal in that group is not optimal.
Like I said earlier, TSH communicates and works with the thyroid. The pituitary gland in the brain releases TSH which then stimulates the thyroid gland. The thyroid gland then produces its T4 hormone (and a small amount of T3), which is then converted to the T3 hormone primarily in the liver. T3 is the active form of the thyroid hormone and is the most important.
To take it to another level, there is a difference between Total T4 and Total T3 vs. Free T4 and Free T3. The body’s cells can only use the free forms of the hormone and Free T3 is the most important. Your body uses proteins to transport T4 & T3 hormones in the blood stream. Your body breaks up the proteins and allows the T3 to be absorbed at the cellular level (which makes it Free T3).
T4 is converted to T3 primarily in the liver and this is typically a problem for most people with hypothyroidism. During times of stress the body converts T4 into Reverse T3 (RT3) instead of T3. This is a normal process that typically is very short lived. When the body is under extreme physical, chemical and/or emotional stress this conversion of T4 into Reverse T3 becomes chronic and is very dangerous.
The leading cause of hypothyroidism is caused by an autoimmune condition called Hashimoto’s Disease, which was the first to be recognized as an autoimmune condition in 1912. Hashimoto’s Disease causes the body to attack its own thyroid gland tissues. Testing thyroid antibody levels (TPO and TG) reveal this problem. The most common symptom of the disease is feeling worse even with thyroid replacement hormone treatment. Another symptom is when lab tests show both hypothyroid and hyperthyroid levels at different times.58 When diagnosing a client with potential thyroid problems I always recommend a complete thyroid panel that includes at least: TSH, Free T4, Free T3, Reverse T3 and Thyroid Antibodies. Depending on what is found in the lab tests, there are different protocols we could follow to heal the thyroid.
Most doctors don’t run Reverse T3 or Antibody testing because their treatment would be the same regardless of the results. They typically give a prescription synthroid (or generic Levothyroxine), which is a T4 hormone replacement. If the patient is seeing an alternative medicine practitioner they will typically be switched to Armour thyroid, which is a bio-identical T3/T4 hormone from pigs, not just T4. A recent issue that has emerged is that the manufacturers of Armour thyroid are reducing their production costs by adding gluten as a filler. If you need a bio-identical T3/T4 hormone, I recommend that you find a compound pharmacy to specifically make it for you and eliminate the gluten filler because research has shown a correlation between gluten intolerance and Hashimoto’s
A3) Heavy Metals
Conventional testing for heavy metals consists of drawing blood to see what’s in the blood stream. The problem is that heavy metals will only appear in the bloodstream if there was an acute exposure within the last week. For example, if you broke a thermometer and had your blood tested two days later, mercury would likely be found in your bloodstream. This kind of testing is not accurate for determining the effects of a lifetime chronic metals. The target of heavy metals is not the blood stream. That means that if you grew up in a home with leaded pipes but were not exposed to lead in the last week, a standard blood test for lead would come up negative but there would still be lead stored up in your body (and specifically your bones). Standard blood tests miss the heavy metals that are being stored in your body. of exposure or exposure to heavy
Hair analysis is another testing method that practitioners use. However, while hair analysis has some accuracy for minerals, it is not useful for detecting heavy metals. Also, some practitioners muscle test for heavy metals. I caution against this type of testing for heavy metals. I am not against muscle testing in general, but it is not useful regarding heavy metals. For instance, mercury has a high affinity for brain tissue (specifically the hypothalamus and pituitary gland). When someone is muscle testing they are challenging the nervous system, including the brain. Since mercury is a neurotoxin that targets the brain, the accuracy of muscle testing would be impacted by any mercury present in the brain at the time of testing. I think of mercury as the heavy metal of deception. My wife had a blood test and a hair analysis for heavy metals that came back negative. She was also muscle tested and heavy metals were shown to not be a major issue. Those results were inaccurate and it caused more suffering until someone told us how to properly test for heavy metals.
The best test that is currently available is a heavy metal urine challenge test. When being given this test, you take a true heavy metal chelator like DMPS, DMSA, or EDTA and your urine is then collected to be analyzed. The chelator pulls heavy metals out of the body through the liver, kidneys, and urine. In this test, the urine is sent in and inspected for the presence and amount of twenty different heavy metals. There are very specific instructions needed for this test to make sure it is performed correctly and to ensure that it doesn’t cause the individual any harm. Go to a trusted health professional with experience in testing and treating heavy metal toxicity to have this test properly administered.
A4) The Digestive Tract (Digestion Testing)
A5) Biotoxins (Lyme and mold)
Years ago, the C4a biotoxin marker test was great because the National Jewish Laboratory was used to process the C4a results. Today, other laboratories often handle the analyzing of the samples for this test and their results are not as clinically accurate. The National Jewish Laboratory had a normal range of less than 2,800 while the new testing states that levels are normal when they are less than 700. That is a huge shift and I don’t believe it is backed up by science. In fact, it just muddies the water and makes properly identifying biotoxic illness more difficult. Also, the C4a is a general biotoxin marker, so it does not specify between mold or Lyme disease. As I previously mentioned, the VCS test (Visual Contrast Sensitivity) can indicate biotoxin levels and is therefore more accurate and useful.
6i) Exposure to mold
An exposure to mold incurred while inhabiting a residence thirteen years ago. Ongoing exposure in carpets. Ongoing exposure in food. My condition initially began immediately after cleaning a garage. I also took many naps using a moldy pillow. Lymes usually is existing and going on with parsites, molds and other biofilms, leaky gut, etc. http://www.helladelicious.com/diy/2012/06/biofilms-parasites-mold-and-electromagnetic-frequencies/
The Truth about Mold
While it is easy to grasp the concept of toxins in our food and water, you may be less aware of another factor in your environment that can have serious repercussions for your health and wellness: molds.
Molds are a form of fungus, usually microscopic, that live and reproduce on organic matter such as plants or animals. While the word “mold” tends to have a negative connotation, it actually describes a diverse group of organisms, some beneficial and some harmful. Most of us are aware that mold plays a critical role in our ecosystem. When living things die, mold sets in and makes them biodegradable. Without it, our land and oceans would be bursting with all of the dead plants and animals from years gone by. Mold works in a miraculous way to get rid of filth.
Mold consumption impacts the diet aspect of the Complete Healing Formula™. That’s not to say that all molds are bad for you. Some of them are actually beneficial. Many delicious and healthy cheeses owe their existence to healthy molds. The species Penicillium roqueforti is the key mold that gives Gorgonzola, Stilton, and the aptly named Roquefort cheeses their distinct flavors and appearances. Beyond these three, many other cheeses likewise require other safe, edible kinds of molds in the mix to craft their appealing flavors.
But not all molds are beneficial to your dietary balance. On the contrary, we also encounter several toxic and dangerous forms of mold in our daily lives. Your food pantry, your bread, your fruit basket, the rind of your orange, and the walls of your kitchen themselves are just a few places where these toxic molds can grow—with dangerous and sometimes even life-threatening repercussions for your health.
Estimates suggest that there are anywhere from tens of thousands to hundreds of thousands of mold species. Covering them all in this chapter is simply impossible. Fortunately, it’s also unnecessary. The most valuable things to understand are why certain molds are dangerous and how you can identify them.
Some molds are visible; others are invisible. Some are helpful; others are extremely dangerous. Regardless of the mold, however, most require certain conditions to spread and thrive. Once you know those conditions, you can avoid them and work toward greater balance in your diet.
The next few pages will explain how molds form, cover the different types of molds that can adversely affect your health, and show you how to manage mold consumption in your diet.
The Dangers of Mold
What are molds, how do they spread, and why are they harmful to our overall health? Molds are composed of pervasive roots—specifically, from stalks rising out of those roots that are capped off with spores. We can see these spores with the naked eye. The spores are what give molds their individual appearances and colors, and they are also the source of the molds’ dangerous effects.
Mold spores spread through the environment through the air. Certain molds, such as those found in some buildings, give off spores that cause allergic reactions and respiratory problems. The presence of mold in a home is rightly a cause for grave concern. Until the molds are eliminated, and their spores cleared from the atmosphere, the environment is toxic.
Many molds have a more pervasive and dangerous effect on our health than simple allergies. Several types of molds produce “mycotoxins,” which, as their name suggests, are extremely toxic. Worse, many molds have extremely intricate root systems, which allow mycotoxins to penetrate far deeper into a substance than the visible spores lead us to believe. Each grain, fruit, tea and coffee plant, herb, and vegetable has its molds— and, odds are, you’re eating them.
Aflatoxin
Aflatoxin is one of the more pervasive and toxic molds out there. This is no surprise given the conditions in which it thrives best. Aflatoxin is found primarily on corn and peanuts, both of which are staples of the modern American diet.
This mold is recognized by the USDA as a cancer-causing poison. So it comes as no surprise that Dr. Hulda Clark’s research uncovered aflatoxin in virtually all of her cancer patients. Aflatoxin also appeared in all of Dr. Clark’s cases of hepatitis and cirrhosis. This mold attacks the body’s immune system, leaving the gates of our defenses wide open to pathogens.
Aflatoxin is not easily cleared from the body because it weakens and kills portions of the liver—the organ that is meant to detoxify our systems. Large doses or continued exposure to this mold will harm your health through its detrimental effects on the liver. That said, it can take weeks for aflatoxin’s effects to be realized, and it is both tasteless and scentless. So how can you know if your food is moldy?
In addition to thriving on corn and peanuts, aflatoxin is also found in your cereal, bread, pasta, nuts, maple syrup, orange juice, and other foods. The good news is that it is not found in dairy, fresh-washed produce, or water. Goods produced in bakeries that are left open to air also don’t contain aflatoxin, and the same is true for products made with carefully screened, deseeded wheat.
In short, given the common American diet, the possibility that you are consuming foods riddled with aflatoxin is very likely unless you take the proper steps to avoid this moldy invader. Dr. Clark advises preparing your own food, testing the foods you can’t prepare yourself, treating foods for molds whenever you can, and getting rid of the rest of it. One of the most important things to understand is that you can’t kill molds through the basic heating or reheating of food. Foods containing aflatoxin must be boiled for several minutes—at a temperature much higher than the boiling point—or else be baked at an even higher temperature in order to kill this mold. So if your food can’t be heated to an elevated temperature, this method will not kill the aflatoxin.
Some industrial research journals suggest treating food ingredients with hydrogen peroxide or metabisulfite, a reducing agent. While the introduction of these chemicals may kill the mold, however, that’s not their only effect. They also damage the nutritional value of your food—not to mention its flavor.
The only natural way to ensure that your food isn’t infested with aflatoxin, as Dr. Clark suggests, is through the use of vitamin C. Be advised that you should use whole-food vitamin C for this, not ascorbic acid. Ascorbic acid is not true vitamin C, but rather a chemical compound, as I will discuss later in this book. Only real vitamin C will have the purifying effect on your food that Dr. Clark identifies.
When baking your own bread, Dr. Clark advises adding a bit of vitamin C to the dough to keep it free of mold for a longer time. In both powdered and liquid forms, vitamin C is an easy way to quickly ensure the safety of your food. Still, be sure to consume the bread quickly, or slice and freeze it to prevent the resurgence of the aflatoxin.
Purchasing commercially available bread is dangerous, since vitamin C can’t be added before baking, and you can’t be sure how long the bread has been sitting on the shelves in a store or bakery since it was made. Other foods are also easy to treat with vitamin C. Rice and pasta can be cleansed of aflatoxin simply be adding vitamin C during or immediately after cooking.
Vinegar can be detoxified as well simply by adding some vitamin C before refrigerating it. You can even rid honey of mold if you heat it slightly and add a few tablespoons of vitamin C to the container.
Some foods, like nuts, need a slightly different treatment. Simply sprinkling vitamin C on nuts or corn will not remove the aflatoxin from these foods because they have already been penetrated by molds. Nuts have to be washed and covered with water that has been mixed with vitamin C powder. After five minutes, the vitamin C has detoxed the nuts and they can be dried in the oven using low heat.
Interestingly, many cultures traditionally treat corn in a way that naturally clears it of aflatoxin. The process that these cultures use is called “nixtamalization,” which involves soaking and cooking corn in a limewater solution. This alkalizes the corn, and the presence of vitamin C in the limewater rids it of aflatoxin.
Avoid the harmful effects of aflatoxin by steering clear of the common foods where this mold appears whenever you can, to ensure it doesn’t enter your system. However, keep in mind that, because the foods on which aflatoxin thrives are so common, a preventative treatment cleanse is also necessary to avoid ingesting this cancer-causing organism. I’ll talk more about cleanses in chapter 15.
Zearalenone
Zearalenone, or “zear” is another common and dangerous mold to avoid. Like its cousin aflatoxin, zear is often found in commercial cereal grains and processed foods such as popcorn, corn chips, and brown rice. Zear can lower your immunity, just as aflatoxin does. It furthermore keeps your body from being able to detoxify benzene, which Dr. Clark says is
common in AIDS sufferers. In addition, this mold is linked with estrogendependent
diseases, including breast cancer.
Another mycotoxin, zear is an anabolic and estrogenic metabolite. The mold appears as extra estrogen in animals’ bodies. Many animal studies have shown this mold to have negative impacts on reproductive health, such as infertility and in-utero death.
But such negative effects are not limited to animals. Even beyond breast cancer, Dr. Clark found in her research that zear speeds up the maturing process in females, and could cause PMS, ovarian cysts, and infertility. In males, even small amounts of zear ingested daily could dramatically affect maturation. Whether the toxin stimulates additional estrogen to develop or functions just like estrogen is not yet clear.
High heat is not effective when it comes to purging foods of zear. If your immunity is compromised or you experience any of the other effects noted above, Dr. Clark advises going off moldy food suspects that may contain zear right away.
Ergot
Ergot is a mold whose effects are unusual and felt very fast. It is immune to heat and highly toxic to children. At any age, however, erratic behavior can be a consequence of ingesting ergot. Irrational thoughts, surreal ideas, and unusual emotions are significant red flags. Those who are commonly sick may also be experiencing high levels of this toxin. According to Dr. Clark, the effects of ergot also include paranoia, hearing voices, and even seizures.
If you notice any of these erratic behaviors in yourself or someone you are close to, it would be a good idea to make dietary changes to reduce your intake of ergot. For example, erratic behavior in children is often written off as allergies, when in truth ergot toxicity could be to blame. If you find your child behaving like “Jekyll and Hyde,” Dr. Clark suggests eliminating cold cereals, nuts and nut butters, store-bought baked goods, soy, honey, and syrups for three weeks.
Replace those foods with hot cereals, home-baked goods, potatoes, and honey with added vitamin C. Because alcohol together with ergot is more toxic than each is on its own, alcohol heightens the negative effects of ergot. It appears that alcohol also drives ergot deeper into the tissues. Dr. Clark has found ergot and aflatoxin in beer and wine, and suggests that perhaps some inebriated behaviors are the result of this mold and alcohol combination.
If you intend to consume foods that may contain ergot, Dr. Clark notes that you can detoxify this dangerous mold easily in about ten minutes using Vitamin C. She also notes that honey should be detoxified right away before consumption.
Other Molds to Avoid
Aflatoxin, zearalenone, and ergot are only a few of the toxic molds we need to reduce or eliminate in our diets. There are several other molds to be aware of as well.
Cytochalasin B
Cytochalasin B, or “cyto B,” is another fungus that lowers immunity, which it does by impeding cell division. For example, portions of the liver that are dead are unable to regenerate as they normally would in the event of a toxic encounter. Cyto B it is found mainly in pasta.
Kojic Acid
Kojic acid prevents the body from being able to detoxify wood alcohol, which results in damage to the pancreas, pancreatic fluke infestation, and even diabetes. Dr. Clark advises against eating potato skins and points out that this mold is also found in regular coffee.
T-2 Toxin
Dr. Clark has found T-2 toxin in every case of high blood pressure and kidney disease. She notes that it is found in dried peas and beans, but that this dangerous mold can be detoxified by adding vitamin C to the soaking water for these foods for five minutes. She adds that you should discard the imperfect peas and beans first, as an extra safety measure.
Sorghum Molds
Sorghum molds are found in sorghum and millet. Elderly people are more susceptible to these mold toxins, which cause hemorrhaging and appetite loss, and make it hard to swallow. Dr. Clark advises against buying sorghum syrup, and says that you should rinse millet in water with vitamin C or add vitamin C to the water before cooking.
Patulin
Patulin is the major fruit mold toxin. It is dangerous because the mold that produces it can grow in patches in your intestine. According to Dr. Clark, E. coli and shigella can permeate the colon wall and begin to invade your body, spreading to areas of injury and tumor sites.
Patulin is found in many common fruits when they are bruised. Those with bowel disease or cancer should not consume fresh fruit besides bananas and lemons for a few weeks. After that, all fruit should be carefully inspected for bruising, and Dr. Clark warns to be thorough in the inspection: even a single soft grape can reinfect you.
Mold and Your Diet
The following are foods Dr. Clark says should be carefully considered prior to consumption:
Crackers: Children should not be fed crackers ever as they are notoriously moldy. Make your own treats in the oven.
Dried fruits: These are highly moldy and should be soaked in vitamin C water and refrigerated or frozen. Overripe fruit should not be baked or preserved.
Peanut butter: Nut butters bought in a store can’t be detoxified, so you should make your own.
Tea: Tea sold in bags is very moldy, so it is better to buy tea in bulk. Store tea in the double plastic bag it comes in, which will also prevent antiseptics in the bag itself. When using fresh herbs, only half as much is required to make tea, which should be done using a sterile
bamboo strainer.
Maple syrup: Pure maple syrup contains aflatoxin and other molds that you can often see. The aflatoxin can be removed with vitamin C, but the other molds need to be exposed to high heat too. You can bring the syrup to a near boil in its original jar without the lid and
then refrigerate.
Hot cereal: It is easy to spot the mold here and remove all of the dark shriveled pieces. By adding salt and honey while cooking, you can detoxify your hot cereal grains further. Grains shouldn’t sit in your cupboard for more than six months, and should not be refrigerated
(only frozen) if not kept in the cupboard.
Against the Grains
According to Dr. Clark, our grain consumption should be very limited. Many molds in pastas, breads, and cold cereals can’t be seen or smelled. Potatoes are a preferable option, as you eat them just the way they were harvested. When grains are processed, it opens them to a variety of molds. Potatoes should be scrubbed prior to eating, and all eyes should be removed.
Coexisting with Mold
Mold could be called a necessary evil. While it is vital to the balance of the environment, if not carefully monitored, it can make us very sick in a variety of ways. It is not complicated to co-exist with mold, but it does require diligence on our parts to make sure that what we put into our bodies is as safe as it can be.
Keep in mind that you don’t have to go to extremes with this all at once. The first step is knowledge and awareness. Once you have that, you can start taking small steps to reduce your exposure to molds, then build on it over time. This is only one part of the bigger picture when it comes to managing excesses, deficiencies, and stagnations in your diet.
Now you’re aware of the serious threats that toxic and moldy foods pose to our dietary balance, and how they can undermine the Wellness Model of Health™. But there is one more culprit when it comes to sabotaging health through diet: inflammatory foods. The next chapter will take you through everything you need to know about these foods, and show you how you can eliminate them from your diet to promote greater wellness.
Chapter Review
Toxic foods harm our white blood cells and weaken our immune systems.
Five common immunosuppressants you should try to avoid most in foods are: polychlorinated biphenyls (PCBs), benzene, asbestos, azo dyes, and heavy metals.
Molds are a form of fungus, usually microscopic, that live and reproduce on organic matter such as plants or animals.
Some forms of mold are toxic and dangerous, and can be found in common foods we eat.
Mold spores spread through the environment through the air.
Some foods that commonly contain mold include: crackers, dried fruits, peanut butter, tea, maple syrup, and hot cereal, as well as pastas, breads, cold cereals, grains, and potatoes.
Recommended Resources (not accepted medical science)
ElectroCleanse
Developed by the Dr. Clark Research Association, the ElectroCleanse is a powerful tool that can aid you in the recovery of many major medical disorders. Find out more at www.losethebackpain.com/productreviews/electrocleanse.html.
Dr. Clark Research Association You can learn more about the tools available to clear toxins from your system from the Dr. Clark Research Association at www.drclark.com.
Clark Therapy by Ignacio Chamorro Balda
You can get even more information about the tools and methods that have arisen from Dr. Clark’s work in the book Clark Therapy by Ignacio Chamorro Balda.
Lyme Disease Testing (see Appendix Lymes)
A6) Vitamin D K1 and K2 deficiency
Micronutrient test available through a laboratory called SpectraCell that measures 33 vitamins, minerals, and antioxidants in your body. I am a fan of this test because it measures the vitamins, minerals, and antioxidants inside your cells. As I mentioned earlier, I recommend that clients take the Vitamin D3 test (technically called 25-hydroxy Vitamin D). This testing measures the amount of Vitamin D3 that is floating in your bloodstream. However, it does not measure how much Vitamin D3 is inside of your cells. So why would I run a Vitamin D3 test along with a micronutrient test when the micronutrient test looks at the amount of Vitamin D3 that is inside of the cell? I’ve found that clients, especially clients who have very seve r e symptoms, have a Vitamin D3 level within the recommended 60-100 ng/mL range because they have been supplementing with Vitamin D3, but their micronutrient level is low. Clinically, this indicates that there is inflammation at the cellular level and the Vitamin D3 is not able to get into the cell at an optimum level. This is why knowing both numbers is so important! Treating someone with a Vitamin D deficiency is very different than treating someone with a generalized cellular inflammatory problem. Vitamin K2 is also extremely important and has a close relationship with Vitamin D3. While there is currently no standard blood test for Vitamin K2, the micronutrient test does test for Vitamin K2!
Tests to analyze the following: Vitamins Minerals Vitamin A, Vitamin B1, Vitamin B2, Vitamin B3, Vitamin B6, Vitamin B12, Vitamin C, Vitamin D3, Vitamin K2, Biotin, Folate, Pantothenate Calcium, Magnesium, Zinc, Copper
Amino Acids Asparagine, Glutamine, Serine
Antioxidants
Carbohydrate Metabolism Fatty Acids Alpha Lipoic Acid, Coenzyme Q10, Cysteine, Glutathione, Selenium, Vitamin E, Total Antioxidant Function, Chromium, Fructose Sensitivity, GlucoseInsulin Metabolism, Oleic Acid
Metabolites Choline, Inositol, Carnitine
Biotoxin Testing
A7) Cardiovascular Testing (Good and Bad Cholesterol)
A8) Male & Female Sex Hormone Testing
A9) Allergy Testing
A10) Methylation Testing
A11) Hair Testing
From: 'Hair Mineral Analysis' https://www.utopiasilver.com/hair-mineral-analysis/?wpam_id=7
A mineral analysis is a test which measures the mineral content of your hair.
- Mineral content of the hair reflects the mineral content and condition of the body’s tissue.
- If a mineral deficiency, excess, or imbalance exists in the hair, it usually indicates the same within the body.
- For example: If your hair reveals an calcium level above normal, then your calcium level within the body may be elevated also.
- This can often be caused by either a consumption of too much of the wrong kinds of calcium or consumption of even the right kind of calcium but not in the proper ratio of magnesium.
- In this case, a strong tendency exists for a build up in the arteries resulting in Arteriosclerosis (hardening of the arteries due to calcium plaque buildup), in the joints causing Arthritis, and in the muscle tissue causing stiff and sore muscles.
- Why do a Hair Mineral Analysis?
- Hair mineral analysis is a wise investment for almost everyone as it can prevent you from spending money on supplements you may not need. It allows you to target your deficiencies without blindly scatter-shooting.
- Mineral deficiencies and imbalances, frequently lead to metabolic dysfunctions before any symptoms become manifest.
- If you can predict such a dysfunction by a mineral analysis, it may be correctable before it develops into a full blown health problem
- Hair analysis opens up a whole new vista for the solving of your own particular problem by recognizing your biochemical individuality.
- An analysis also helps to save money spend on supplements, because you are able to more narrowly target what your body actually needs rather than scatter-shooting with supplements you may not need.
- The procedure is easy:
- It simply takes a small snippet of hair about 1-1/2” long from the base of the hairline at the back of the neck.
- We then ship it to a laboratory specializing in mineral analysis and the test is performed for the essential minerals Calcium, Magnesium, Sodium, Potassium, Iron, Manganese, Zinc, Chromium, Selenium, Phosphorus, Nickel, Cobalt, Molybdenum, Lithium, and Boron. It also tests for the toxic metals Lead, Mercury, Cadmium, Arsenic, and Aluminum.
- The results are then returned to Dr. Ken and he will contact you for a comprehensive consultation with recommendations that should aid in correcting the problem areas.
Just as this condition affects everyone differently, so do the medications used to treat it. It's essential that you work closely with your doctor to find what's right for you. You should be familiar with the possible side effects and let your doctor know about any you may develop.
If you're on more than one medication (prescription or over-the-counter), let your doctor and pharmacist know so you can avoid negative interactions.
Test for Post Exertional NeuroImmune Exhaustion (PENE) & Post Exercise Malaise, and Muscle Weakness tests PDF
Cytokines, Chemokines and Their Receptors
Mark J. Cameron and David J. Kelvin.
https://www.ncbi.nlm.nih.gov/books/NBK6294
Introduction
The immune system is skilled in communication and designed to respond quickly, specifically and globally to protect an organism against foreign invaders and disease. The cytokine superfamily of proteins is an integral part of the signaling network between cells and is essential in generating and regulating the immune system. Much progress has been made recently in interpreting how the immune system communicates with, or is mediated by, cytokines and chemotactic cytokines (chemokines. These interacting biological signals have remarkable capabilities, such as influencing growth and development, hematopoiesis, lymphocyte recruitment, T cell subset differentiation and inflammation. This chapter provides brief synopses for a comprehensive list of immune-related cytokines and chemokines. Information such as gene cloning and mapping details, protein characteristics and expression, receptor usage, source and target cells, major biological functions and knockout phenotype is described for each cytokine and chemokine. With an approach that organizes cytokines and chemokines into interacting groups with related physical and/or functional properties, this chapter aims to highlight the capability of this system to maintain widespread impact and functional complementation while not sacrificing regulation and specificity of action. A more complete understanding of these properties may lead to more advanced means of correcting improper cytokine\- or chemokine-mediated immune responses, such as those causing autoimmune disease.
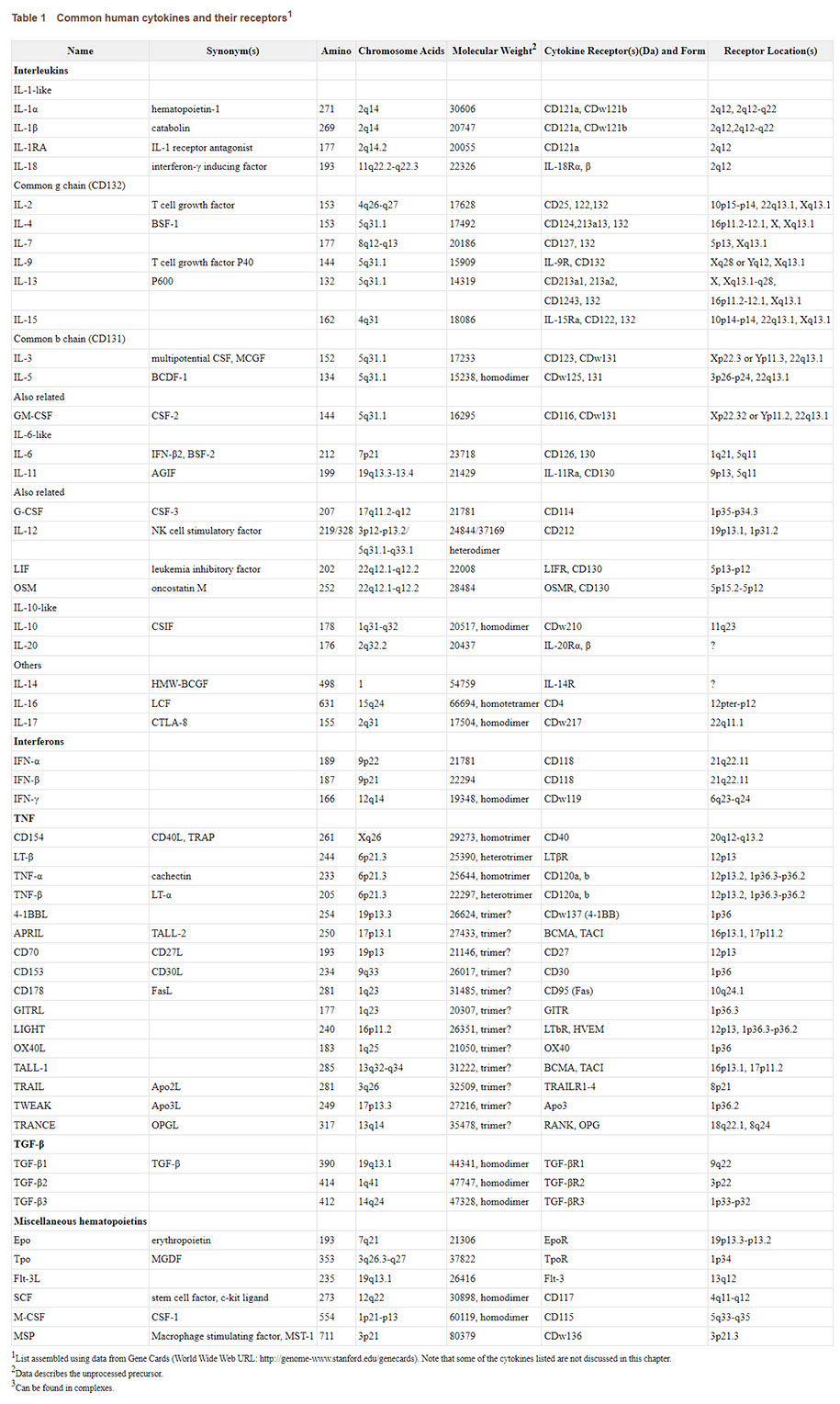
click here to open larger version of chart in larger window to view or download
Detailed and reliable communication must occur through a complex system of network connections to accomplish a task at a modern workstation. In parallel, the immune system is an interdependent biological network charged with developmental tasks and the responsibility of protecting its host against injury and infection. An immune cell within a given microenvironment can respond to signals received through its receptors with its own protein-based language that will influence the cell itself (autocrine effect or other cells throughout the organism (paracrine effect. The language of cytokines is critical in this communication. Cytokines are small soluble factors with pleiotropic functions that are produced by many cell types as part of a gene expression pattern that can influence and regulate the function of the immune system.
The term cytokine was proposed by Cohen et al in 1974^1 to replace lymphokine, a term coined in the late 1960's to denote lymphocyte-derived soluble proteins that possess immunological effects.^2 Since the latter designation misleadingly suggested that lymphocytes were the only source for these secreted proteins, the term cytokine slowly became preferred. Following the introduction of this general term, the Second International Lymphokine Workshop held in 1979 proposed the interleukin (IL system of nomenclature to simplify the growing list of identified cytokines. Ironically, this partially adopted system introduced confusion in that the interleukins, presently numbering at least 23, affect many cell types but their name implies that they act only among leukocytes. As a result, modern cytokine nomenclature is a mix of the widely accepted, but slightly misleading, interleukin designations and other proteins still known by their original names. A good example of these potential points of confusion is the chemotactic cytokine (chemokine IL-8, which is produced by and targets a wide variety of cell types including leukocytes and nonleukocytes.
As this chapter unfolds, repeated mention of a number of cytokines and chemokines will make it clear that these proteins can be part of a bigger immune program, e.g., T cell subset differentiation. Mature CD4 and CD8 T cells leave the thymus with a naive phenotype and produce a variety of cytokines. In the periphery, these T cells encounter antigen presenting cells (APCs displaying either major histocompatibility complex (MHC class I molecules (present peptides generated in the cytosol to CD8 T cells or MHC class II molecules (present peptides degraded in intracellular vesicles to CD4 T cells. Following activation, characteristic cytokine and chemokine secretion profiles allow the classification of CD4 T helper (Th cells into two major subpopulations in mice and humans.^3 ^-^^7 Th1 cells secrete mainly IL-2, interferon-γ (IFN-γ and tumor necrosis factor-β (TNF-β, whereas Th2 cells secrete mainly IL-4, IL-5, IL-6, IL-10 and IL-13. Th1 cells support cell-mediated immunity and as a consequence promote inflammation, cytotoxicity and delayed-type hypersensitivity (DTH. Th2 cells support humoral immunity and serve to downregulate the inflammatory actions of Th1 cells. This paradigm is a great example of an integrated biological network and is very useful in simplifying our understanding of typical immune responses and those that turn pathogenic. For example, the failure to communicate “self” can lead to a loss of tolerance to our own antigens and prompt destructive immune responses to self-tissues and autoimmune disease. Autoimmunity, the major focus of this book, is the underlying mechanism of a set of conditions, such as type 1 diabetes mellitus, multiple sclerosis and rheumatoid arthritis. Autoimmune diseases may be caused in part by cytokine\- and chemokine-mediated dysregulation of Th cell subset differentiation. The main factors affecting the development of Th subsets, aside from the context in which the antigen and costimulatory signals are presented, are the cytokines and chemokines in the stimulatory milieu. A better understanding of the properties and interactions of the individual cytokines and chemokines that play a role in Th cell activation may lead to more advanced treatments for autoimmune disease.
The proceeding sections will introduce many of the currently identified cytokines and chemokines, along with their receptors. You will find that cytokines and chemokines with related structure and/or function are clustered into groups of interdependent homologues, e.g., the IL-1-like cytokines. A particular group of cytokines or chemokines can exhibit functional redundancy with, and widespread impact on, other groups of cytokines or chemokines, e.g., IL-1-like cytokines and IL-6-like cytokines. Interestingly, this can occur while maintaining several regulatory features, such as internal checkpoints and specificity of action. It is therefore hoped that this chapter may serve as more than a brief catalogue of the field of cytokines, chemokines and their receptors, but may also highlight the remarkable capabilities of this interacting network of biological signals.
Cytokines, their Receptors and their Genes
Table 1 table/A13506/?report=objectonlyintroduces the human cytokines and lists some of their properties, such as receptor usage and physical characteristics. Each human cytokine described in Table 1 table/A13506/?report=objectonly has a murine counterpart so the basic list can be used interchangeably in regards to terminology. Hundreds of cytokines have been identified. In the interest of conciseness the table includes only common cytokines with recognized immune function, many of which are discussed in more detail below. Excluded are the ‘growth factors’, neurobiological proteins and ‘trophins’, for example. It is also beyond the scope of this chapter to describe how cytokines signal through their receptors in any detail. One popular cytokine signaling mechanism used by cytokines such as IL-2, IL-4, IL-6, IL-7, IL-10, IL-12, IL-13, IL-15 and the interferons, however, begins with dimerization of the appropriate receptor chains upon ligand binding. Following this, different types of receptor-associated Janus family tyrosine kinases (Jak are activated which phosphorylate the receptor chains and allow the recruitment and activation of other kinases and transcription factors, such as those of the signal transducer and activator of transcription (Stat family. This promotes the rapid translocation of these proteins to the nucleus and stimulation of target gene transcription (see references 8 and 9 for more details on cytokine signaling.
Common human cytokines and their receptors1.
IL-1-Like Cytokines
Firstly, the interleukins are comprised mostly of hematopoietic growth factors and can be further divided into groups of proteins as shown in Table 1 table/A13506/?report=objectonly. The IL-1-related group of pro-inflammatory cytokines consists of IL-1α, IL-1β, IL-1 receptor antagonist (IL-1RA and IL-18. IL-1α and IL-1βare produced mainly by mononuclear and epithelial cells upon inflammation, injury and infection.^10 These two proteins are of primary importance to the outcome of these challenges to the immune system in that they trigger fever, induce a wide variety of acute phase response (APR genes and activate lymphocytes.^10 IL-1α and IL-1β arise from two closely linked genes that, along with the IL-1RA gene, lie on human (and mouse chromosome 2.^10 ^,^^11 The two forms of IL-1 are quite similar in function since they both signal through the IL-1 type 1 receptor (IL-1-R1/CD121a.^12 Both proteins can also bind to the IL-1 type 2 receptor (IL-1-R2/CDw121b which does not appear to be involved in signaling, except as a possible decoy.^13 The IL-1 receptor genes are located on human chromosome 2 along with their ligands, albeit at a distance.
Murine knockout studies confirm the importance of IL-1 in fever responses and the APR. While at least three studies involving the IL-1β knockout mouse demonstrate that fever development is suppressed upon turpentine or lipopolysaccharide (LPS challenge,^14 ^-^^16 one study demonstrates that the role of IL-1β as a pyrogen is not obligatory and that its absence can in fact exacerbate an induced fever response.^17 The latter conflicting result may stem from differences in experimental protocol or reagents.^14 Knockout studies also show that while both forms of IL-1 can induce fever responses, fever induction is not reduced in IL-1α knockout mice, indicating that IL-1βcan compensate for IL-1α but not vice versa.^14 The role for IL-1 in the APR (a series of cellular and cytokine cascades in reaction to trauma or infection that help limit damage was confirmed in a localized tissue damage model of turpentine injection where challenged IL-1β-deficient mice did not develop an APR.^18 Accordingly, IL-1R1 knockout mice are irresponsive to IL-1 in the induction of IL-6, E-selectin and fever.^18 These mice also have a reduced APR to turpentine.^19
IL-1RA is produced by virtually any cell that can produce IL-1 and is similar in structure to IL-1β but lacks its agonist activity.^20 The different species of IL-1RA, a secreted form with a signal peptide and at least two intracellular forms, arise from alternative splicing of different first exons on chromosome 2.^20 ^,^^21 IL-1RA represents an intriguing example of a naturally occurring cytokine receptor antagonist. IL-1RA may be an acute phase protein that may serve to regulate the agonist effects of IL-1 during chronic inflammatory and infectious disease because its expression is influenced by cytokines, viral and bacterial products, bound antibody and acute phase proteins, such as IL-1, IL-4, IFN-γ and LPS.^20 Consistent with this notion are two studies of IL-1RA-deficient mice which exhibit growth retardation, an exacerbated fever response to turpentine injection, increased lethality following LPS injection and decreased susceptibility to *Listeria monocytogenes.*^14 ^,^^22 These observations verify the importance of balance in the IL-1 system in mediating these immune challenges.
IL-18, initially termed interferon-γ inducing factor (IGIF, is a pro-inflammatory cytokine that is encoded on human chromosome 11 and mouse chromosome 9.^23 IL-18 has been placed in the IL-1 group of interleukins because it bears structural homology to IL-1α and β, is converted into a mature form by IL-1β converting enzyme (ICE along with IL-1β and binds to the IL-18 receptor (IL-18R or IL-1R related protein.^23 The IL-18R resembles the IL-1R and transduces IL-1R signaling.^23 IL-18 shares biological function with IL-12 in that it induces IFN-γ secretion (in synergy with IL-12, enhances natural killer (NK cell activity and promotes inflammatory Th1 cell responses.^23 Accordingly, when IL-18^24 or its receptor^25 is knocked out, mice exhibit defective NK cell activity and Th1 responses. More recently, however, the role of IL-18 as a pro-inflammatory cytokine has been questioned because IL-18 can also potentiate regulatory Th2 responses, perhaps by inducing IL-4 production by natural killer T (NKT cells in certain situations.^26 ^-^^28
Common *γChain* Cytokines
Cytokines that utilize the common γ chain (γc/CD132 in their receptor comprise the next group of interleukins, namely IL-2, IL-4, IL-7, IL-9, IL-13 and IL-15. These diverse cytokines invoke lymphocyte activation and differentiation (the outcome of which can vary and possess some redundancy in biological function because of their common receptor subunit.^29 The γc itself cannot bind cytokines; however, new evidence suggests that it can be shed as a soluble negative modulator.^30 Indeed, γc-deficient mice are severely immunocompromised, as are humans with γc defects.^31 ^,^^32
IL-2 is expressed from a gene on human chromosome 4 or mouse chromosome 3 and is mainly secreted by activated T cells. IL-2 and the heteromultimeric IL-2 receptor (IL-2R complex (combinations of IL-2Rα/CD25, IL-2Rβ/CD122 and γc are upregulated on T cells following antigenic or mitogenic stimulation leading to clonal expansion. As such, IL-2 is commonly regarded as an autocrine or paracrine T cell growth factor but it actually has effects on many cell types, such as B cells, NK cells, macrophages and neutrophils.^29 ^,^^33 ^,^^34 The IL-2 knockout mouse exhibits immune dysregulation caused by defects in T cell responsiveness in vitro; however, only delays in normal T cell functionality were found in vivo.^35 ^,^^36 Interestingly, IL-2Rα\-^37 and IL-2Rβ-deficient^38 mice exhibit loss of T cell regulation and autoimmunity, indicating that proper IL-2 signaling may be required to induce regulatory T cells and/or eliminate abnormally activated T cells via the reversal of T cell anergy or apoptosis (programmed cell death induction, respectively.^39
The IL-4 gene is located on human chromosome 5 (along with the IL-3, IL-5, IL-9, IL-13 and granulocyte macrophage colony stimulating factor (GM-CSF genes and murine chromosome 11 (along with the IL-3, IL-5, IL-13 and GM-CSF genes. Short or long isoforms of IL-4 can exist arising from alternative splicing.^40 IL-4 is produced by activated T cells, mast cells, basophils and NKT cells and targets many cell types, including B cells, T cells, macrophages and a wide variety of hematopoietic and nonhematopoietic cells.^29 ^,^^41 Physiologic signal transduction via IL-4 depends on heterodimerization of the IL-4 receptor α chain (IL-4Ra/CD124, with γc and possibly the IL-13 receptor α chain (IL-13Ra/CD213a1.^42 IL-4 is the principal cytokine required by B cells to switch to the production of immunoglobulin (IgE antibodies, which mediate immediate hypersensitivity (allergic reactions and help defend against helminth infections.^41 IL-4 also inhibits macrophage activation and most of the effects of IFN-γ on macrophages. However, the most important biological effect of IL-4 with respect to immune modulation is the growth and differentiation of Th2 cells. As described earlier, Th2 cells support humoral immunity and serve to downregulate the inflammatory actions of Th1 cells. Moreover, stimuli that favour IL-4 production early after antigen exposure favour the development of Th2 cells.^3 IL-13 is also associated with this subset of T cells.^43 Like IL-4, and along with the fact that it maps closely to IL-4 and shares receptor α subunits with IL-4, IL-13 is expressed by activated T cells, induces IgE production by B cells and inhibits inflammatory cytokine production.^44 These properties of IL-4 and IL-13 have been convincingly demonstrated in mice lacking the IL-4 or IL-13 gene. ^45 ^-^^48 These mice are deficient in the development and maintenance of Th2 cells.
The remaining γc cytokines, IL-7, IL-9 and IL-15, are potent hematopoietic factors expressed from genes on human chromosome 8 and mouse chromosome 3, human chromosome 5 and mouse chromosome 13, and human chromosome 4 and mouse chromosome 8, respectively. IL-7, expressed by stromal and epithelial cells, stimulates immature B cells, thymocytes and mature T cells via its receptor consisting of the IL-7 receptor α chain (IL-7Rα/CD127 and the γc.^49 ^-^^51 Knocking out IL-7 or IL-7Rα/CD127 causes severe defects in thymic T cell and B cell development consistent with the critical roles that IL-7 and its receptor play in maturation of the immune system.^51 ^-^^56 IL-9 promotes the growth of mast cells, B cells and other T cells and is mainly expressed by activated T cells, especially Th2 cells.^29 ^,^^43 ^,^^57 Confirming only the role of IL-9 in enhancing mast cells, the recently generated IL-9 knockout mouse exhibits normal T cell (Th2 responses but not characteristic mast cell expansion upon lung challenge.^58 IL-15, produced by activated monocytes, epithelial cells, and a variety of tissues, shares biological activities with IL-2 in that it stimulates NK cells, B cells and activated T cells.^29 ^,^^59 ^-^^61 The IL-15 receptor (IL-15R consists of combinations of IL-15Rα, IL-2Rβ/CD122 and γc. Similarities in function between IL-2 and IL-15 are partially due to receptor subunit sharing. A recent study, however, provides evidence that IL-2 and IL-15 control different aspects of primary T-cell expansion in vivo. IL-15 is critical for initiating T cell divisions, whereas IL-2 can limit T cell expansion by decreasing γc expression and rendering cells susceptible to apoptosis.^62 The α chain ligand specificity and broad cellular expression range of IL-15 allows for differential activity even outside of the immune system.^29 IL-15\- and IL15Ra-deficient mice were recently generated. Initial studies confirm the role of IL-15 in NK cell stimulation and indicate a role for IL-15 in peripheral CD8 T cell maintenance upon immune challenge.^63 ^,^^64
Common *β* Chain Cytokines
Cytokines that utilize the common β chain (βc/CDw131 in their receptor comprise the next group of interleukins, namely IL-3, IL-5 and GM-CSF. The genes for IL-3, IL-5 and GM-CSF are closely linked and lie on human chromosome 5 and mouse chromosome 11.^65 Like the γc cytokines, these associated (but not particularly homologous at the amino acid sequence level βc cytokines overlap in biological function because of their common receptor subunit.^65 When the βc is mutated, normal hematopoiesis is noted but impaired immune responses can be observed that are most likely due to a loss of responsiveness to IL-5 and GM-CSF, rather than IL-3.^66 ^,^^67
IL-3, originally termed multicolony stimulating factor (multi-CSF, is produced by activated T cells and stimulates both multipotential hematopoietic cells (stem cells and developmentally committed cells such as granulocytes, macrophages, mast cells, erythroid cells, eosinophils, basophils and megakaryocytes.^68 ^-^^70 The human IL-3 receptor consists of CD123 and βc/CDw131. The mouse IL-3 receptor has an additional β chain called βIL-3, the function of which can be compensated for by CD123 if knocked out.^67 Knocking out CD123 itself also has little effect on hematopoiesis.^71 On the other hand, if IL-3 is knocked out, mast cell and basophil development upon challenge is affected,^66 as well as some forms of DTH,^72 confirming a role for IL-3 in host defense and expanding hematopoietic effector cells.
IL-5, originally identified as a B cell differentiation factor, is produced mainly by activated T cells (especially Th2 cells and aids in the growth and differentiation of eosinophils and late-developing B cells.^73 ^-^^75 When IL-5 or CDw125 is absent, mice exhibit developmental defects in certain B cells (CD5/B-1 B cells and a lack of eosinophilia upon parasite challenge.^76 ^,^^77
Lastly, GM-CSF, as its name suggests, was originally found to stimulate granulocytes and macrophages. GM-CSF has since been found to be expressed by many cell types, including macrophages and T cells, and shares many of the functions of IL-3 in stimulating a variety of precursor cells, including macrophages, neutrophils and eosinophils.^78 ^-^^80 Interestingly, GM-CSF-deficient mice have normal hematopoietic development but suffer from pulmonary disease perhaps caused by a lack of lung surfactant clearance by alveolar epithelial cells or macrophages.^81
IL-6-Like Cytokines
IL-6 is the prototype cytokine representing the next group of interleukins. Most of the members of this group utilize the glycoprotein 130 (gp130 or CD130 receptor. IL-6, IL-11, leukemia inhibitory factor (LIF, oncostatin M (OSM, granulocyte colony-stimulating factor (G-CSF and IL-12 have partially overlapping functions and are key mediators in various immune processes including hematopoiesis and the APR. CD130-deficient mice exhibit embryonic lethality, a finding that appears to be linked to a significant role for CD130-dependent signaling in homeostasis.^82
IL-6, with its gene situated on human chromosome 7 and mouse chromosome 5, utilizes the CD130 receptor and the IL-6 receptor α chain (IL-6Ra/CD126. The IL-6Rα/CD126 can exist in a soluble form and serves as an important cofactor by extending the cytokine's half-life.^83 IL-6 was originally characterized as a differentiation factor of B cell hybridomas.^84 ^,^^85 Producers of IL-6 include fibroblasts, endothelial cells, macrophages, T cells (Th1 and B cells. IL-6 is a primary inducer of fever, hormones, acute phase proteins and T and B cell expansion upon injury and infection.^86 It can also act as a cofactor in hematopoiesis by increasing GM-CSF and macrophage colony stimulating factor (M-CSF expression.^87 IL-6-deficent mice exhibit a severely blunted APR following infection or injury,^88 ^,^^89 problems in early hematopoiesis and T and B cell function and Th1 development.^90 Interestingly, IL-6 can nonetheless act as an anti-inflammatory agent in some instances.^91
IL-11, originally identified as a pleiotropic stromal cell-derived cytokine, is encoded on chromosome 19 in humans and chromosome 7 in mice.^92 ^,^^93 IL-11 also utilizes the CD130 receptor along with the IL-11 receptor α chain (IL-11Rα. IL-11 is produced by, and has effects on, many hematopoietic and nonhematopoietic cell types.^94 ^,^^95 IL-11, like IL-6, is known to stimulate acute phase protein synthesis in the liver.^94 ^,^^95 IL-11 also collaborates with other cytokines we have already discussed, such as IL-3, IL-4, IL-7, IL-13 and GM-CSF, to stimulate (by shortening cell-cycle time the proliferation of hematopoietic stem cells and progenitor cells and induce the differentiation of megakaryocytes.^94 ^,^^95 The collaborative nature of IL-11 in vivo may explain why knockout studies have yet to identify a defective phenotype (at least in the hematopoietic compartment associated with a lack of IL-11 signaling.^96 Interestingly, IL-11 could also be an anti-inflammatory mediator as it inhibits macrophage pro-inflammatory cytokine production and can exert protective effects in several disease models.^91
LIF is a ligand for CD130 and the LIF receptor (LIFR. LIF is associated with the differentiation of many cell types.^91 ^,^^97 ^,^^98 In this regard, LIF can both inhibit the differentiation of embryonic stem cells and promote the survival of hematopoietic precursors. LIF can stimulate inflammatory cytokine production. Its expression can be upregulated or downregulated in response to inflammatory cytokines such as IL-1 and TNF or regulatory cytokines such as IL-4, respectively. LIF is therefore often classified as a pro-inflammatory cytokine; however, recent evidence may suggest otherwise in some situations.^91 LIF knockout mice display several phenotypes depending on the disease model.^91 This may be due to the observation that loss of LIF expression perturbs the establishment of a normal pool of stem cells, but not the terminal differentiation of these cells.^99 Unlike IL-6, LIF can also stimulate the hypothalamic-pituitary-adrenal axis in response to stress and disease. This property has been elegantly demonstrated in a recent study of the LIF knockout mouse where mice did not respond to immobilization-induced stress with the normal indicators.^100 It is also interesting to note that the genes for LIF and OSM lie in tandem on human chromosome 22 and mouse chromosome 11 and are transcribed in the same orientation.^101 ^,^^102 OSM is a very similar cytokine produced mainly by activated macrophages and T cells with inflammatory and growth factor properties.^101 ^,^^102
G-CSF (or colony stimulating factor-3 is produced by fibroblasts and monocytes and stimulates granulocyte progenitor cells and neutrophils.^103 ^-^^105 The G-CSF gene is located on human chromosome 17 and mouse chromosome 11 and creates two active polypeptides (differing by only three amino acids by differential mRNA splicing.^103 The G-CSF receptor (G-CSFR is expressed on multipotential hematopoietic progenitor cells and in cells of the myeloid lineage.^104 The importance of G-CSF in granulocyte differentiation and neutrophil development has been verified in G-CSF\- and G-CSFR-deficient mice. These mice have lower numbers of circulating neutrophils, a decrease in granulocytic precursors and impaired terminal differentation of granulocytes.^106 ^,^^107
In discussing the IL-6-like cytokines, it bears to mention the heterodimeric cytokine IL-12. IL-12 was originally called NK cell stimulatory factor and can be regarded as a cytokine and soluble receptor complex.^108 ^-^^110 The “cytokine” subunit, commonly known as IL-12α or p35, is coded for on human and mouse chromosome 3, shows homology with the IL-6-like cytokines and is not active on its own. The “soluble receptor” subunit, called IL-12β or p40, is coded for on human chromosome 5 and mouse chromosome 11, is a member of the cytokine receptor superfamily with homology to IL-6Ra/CD126 and has activity via the IL-12 receptor (IL-12R/CD212 when partnered with IL-12a. While both soluble subunits are required for biological activity, the two components are differentially regulated.^111 IL-12 is produced by APCs and has immunoregulatory effects on NK cells and T cells, two cell types that express the IL-12R.^112 IL-12 plays a critical role in cell-mediated immunity by acting as a requisite cytokine in pushing the balance between Th1 cells and Th2 cells towards Th1-type predominance. It is therefore no surprise that IL-12-deficient mice are defective in mounting an IFN-γ\- or Th1-mediated immune response and/or respond with default Th2 responses when stimulated with antigen or infected with parasites or bacteria.^113 ^-^^115 An interesting note on IL-12 is that a new composite cytokine has been described in mice and humans that consists of a novel a subunit, p19, that combines with IL-12β to form a unique cytokine called IL-23.^116 IL-23 has similar biological functions to IL-12 in that it can induce IFN-γ expression by T cells for example, yet it can act distinctly through an unidentified novel receptor subunit.^116
IL-10-Like Cytokines
IL-10, IL-19 and IL-20 are members of the next related group of interleukins, those with homology to IL-10. The genes for these cytokines are closely linked on human and mouse chromosome 1.^117 ^,^^118 Originally identified as human cytokine synthesis inhibitory factor (CSIF, IL-10 plays a major role in suppressing inflammatory responses. It does this by inhibiting the synthesis of IFN-γ, IL-2, IL-3, TNF-α and GM-CSF by cells such as macrophages and Th1 cells.^119 ^,^^120 However, there is also evidence that IL-10 can act as a stimulator of thymocytes, mast cells and B cells.^120 Monocytes and T cells (Th2 cells are considered to be the main sources of IL-10, although many other cell types can be made to produce IL-10 including B cells, mast cells and keratinocytes.^120 The participation of IL-10 in limiting Th1 cell responses and favoring Th2 cell development has been explored in IL-10 knockout mice. Mice that are deficient in IL-10 spontaneously develop chronic intestinal inflammation caused by uncontrolled cytokine production from dysregulated macrophages and Th1 cells.^121 ^,^^122 IL-19 and IL-20 have been recently identified as IL-10 homologues. IL-19 is under patent application and not yet described while IL-20 appears to stimulate keratinocytes via its unique receptor.^118
Interferons
The interferons are a family of cytokines that play a pivotal role in pathogen resistance. There are two types of interferons, type I and II, that signal through different receptors to produce distinct, but overlapping, cellular effects.^123 The pleiotropic cytokines IFN-α, originally referred to as leukocyte interferon, and IFN-β, originally referred to as fibroblast interferon, are type I interferons that are secreted by virus-infected cells.^124 ^-^^128 Infection by most viruses causes a reaction in the host that includes innate and adaptive immune responses, such as the production of cytokines, increased expression of MHC class I and cytotoxic T cell mobilization. IFN-αand IFN-β, coded for by genes on human chromosome 9 and mouse chromosome 4, appear to be central players in innate immune responses.^128 IFN-αand IFN-β also have the unique ability to regulate adaptive T cell responses, perhaps directly by stimulating production of IFN-γ by activated T cells^129 or indirectly by inhibiting IL-4-inducible gene expression in monocytes.^130 These properties have been verified in knockout mice. Mice lacking the type I IFN receptor (CD118 exhibit impaired antiviral defenses and are deficient in promoting IFN-γ production by T cells.^129 ^,^^131
IFN-γ, also known as immune interferon or type II interferon, is secreted by activated T cells (Th1 cells and NK cells.^123 It was originally identified as an antiviral agent and its gene was mapped to human chromosome 12 and mouse chromosome 10.^123 ^,^^132 ^,^^133 IFN-γ signals through its own CDw119 receptor and has many biological functions. For example, IFN-γ can stimulate macrophages, increase antigen processing and expression of MHC molecules, promote an Ig class switch to IgG2a antibody secretion, and control the proliferation of transformed cells.^123 The immunomodulatory function of IFN-γ, however, has become a major research focus for this cytokine. IFN-γ secretion is the hallmark of proinflammatory Th1 cells but its exact role in T cell subset differentiation remains unclear. Th1 responses are associated with cell-mediated immunity and can best deal with intracellular invaders. Mice with mutations in IFN-γ^134 or IFN-γ receptor^135 expression show decreased macrophage and NK cell activity and increased susceptibility to many intracellular pathogens and viruses. Cell-mediated immune responses can still develop in IFN-γ knockout mice even though enhancements in Th2-type responses can be observed.^136 ^,^^137 As discussed above, IL-12 plays a critical role in eliciting Th1 responses. IFN-γ may act in synergy with IL-12 to accelerate development of the Th1 cell subset and also repress Th2 cells either directly or indirectly.^123
Tumor Necrosis Factors
The TNF family is another example of a large group of interrelated cytokines that has stimulated a vast amount of scientific study.^138 ^,^^139 Most of this work has centered on the TNF family members' shared properties as cell death effectors.^140 The TNF family has been expanding a great deal recently so we have chosen five representative proteins, TNF-α, TNF-β, lymphotoxin (LT\-β, LIGHT (an acronym for homologous to lymphotoxins, exhibits inducible expression, and competes with HSV glycoprotein D for HVEM, a receptor expressed by T cells and Fas ligand (FasL/CD178, to describe in more detail. It appears that all the TNF family members act in trimeric form.^138 ^,^^139 Also, with the exception of TNF-β, the TNF ligands are formed as type II transmembrane proteins. Signaling by TNF family members is quite different than other cytokines we have discussed (see reference 138 and 140 .
TNF-α, with its gene on human chromosome 6 and mouse chromosome 17 in close linkage to TNF-β, LT-β and MHC genes, is a pro-inflammatory cytokine that was originally identified as a tumour cell killer.^141 ^-^^143 TNF-α can be found in a membrane bound or soluble form following proteolytic processing. TNF-α shares a receptor with TNF-β (CD120a, b, which is expressed on virtually all cell types except erythrocytes. TNF-α is produced mainly by activated macrophages, NK cells and T cells (mainly Th1 cells.^139 The most potent inducer of TNF-α is lipopolysaccharide (LPS, a microbial agent. TNF-α plays a role in endothelial activation and lymphocyte movement and is one of the crucial mediators in acute and chronic inflammatory conditions, such as autoimmunity, toxic shock and tuberculosis.^139 ^,^^144 It is also a direct pyrogen and can indirectly alter hormone and IL-1 secretion to induce fever. Like other members of the TNF family, TNF-α can induce apoptosis (programmed cell death in some targets.^140
TNF-β, also known as LT-α or LT, is derived from T and B cells and shares 30% homology at the amino acid level with TNF-α.^142 ^,^^145 TNF-β can exist as a true secreted homotrimeric protein or as a heterotrimeric membrane-associated complex with LT-β.^139 Like TNF-α, TNF-β plays a role in endothelial activation, tumour cell killing, apoptosis and mediation of inflammation. While occasional qualitative and quantitative differences have been demonstrated between the actions of TNF-α and TNF-β, the unique functions of TNF-β have not been fully elucidated.^138
LT-β is a type II membrane protein that can anchor TNF-β in a heterotrimeric complex.^146 LT-β utilizes the LT-β receptor (LT-βR and the herpes virus entry mediator (HVEM.^147 HVEM is a host-encoded receptor that is a member of the tumour necrosis factor receptor family and is exploited by herpes simplex virus (HSV for entry. The same receptors can also be bound by LIGHT, a recent addition to the TNF family. LIGHT is produced by activated T cells, encoded on chromosome 16 in humans and chromosome 17 in mice and capable of both stimulating T cells and causing apoptosis depending on receptor expression.^147 LT-β, however, is produced by activated T and B cells much like TNF-β and is involved in lymph node development.^139
As a testament to their important roles as immune mediators, TNF-α, TNF-β and LT-β knockout studies indicate that these three cytokines are required for normal lymphocyte compartmentalization in the spleen (summarized in reference ^148 . TNF-α\- and TNFR1/CD120a-deficient mice lack follicular dendritic cells and fail to form B cell follicles. TNF-β and LT-β knockout mice exhibit similar defects in the spleen and also show impaired development of other lymphoid organs such as lymph nodes and Peyer's patches. These findings may stem from a role for the TNF-α and membrane TNF-β/LT-β heterotrimer in providing developmental cues to stromal cells to produce the chemokines necessary for lymphoid tissue organization.
FasL, newly assigned to CD178, is located on human and mouse chromosome 1.^149 ^,^^150 Like TNF-α, FasL can undergo proteolytic processing and exist as a soluble mediator. FasL is produced by T cells and is a key mediator of lymphocyte apoptosis and tolerance when associated with its receptor Fas/CD95. Most types of immune cells, as well as many nonlymphoid tissues, express Fas and/or FasL either constitutively or following activation. The Fas system is therefore very important in immune homeostasis and its powerful role must be tightly regulated or dangerous immune reactions and cancers would occur. Two very useful murine models have allowed a good dissection of the ‘death’ roles Fas and FasL play in immunity.^151 ^,^^152 The lpr (lymphoproliferation mouse has a mutation in Fas that prevents Fas-induced apoptosis and causes complex defects in the B and T cell lymphoid compartments. Similarly, gld (generalized lymphoproliferative disease mice are mutated in FasL and suffer the same immunoregulatory defects. The role of FasL in killing Fas-expressing T cells is especially evident in the testes, an area of immune privilege that can accept allografts and xenografts, where FasL expression by Sertoli cells is likely responsible for maintaining an immune barrier or immune tolerance.^153
TGF-β
The transforming growth factor (TGF\-β family consists of more than 30 members. TGF-β1, 2 and 3 are particularly interesting as they are remarkably multifunctional and indispensable, at least in the mouse. These homodimeric proteins are expressed by and have effects on many cell types. They are involved in development, immune regulation, immune tolerance, carcinogenesis, tissue repair and the generation and differentiation of many types of cells. As such, the TGF-β cytokine family represents an excellent example of a point of integration for multiple information networks, i.e., the immune and developmental programs. These functions cannot be completely outlined here and the reader is directed to several reviews for more details.^154 ^-^^156 While the three isoforms of TGF-β are expressed under the control of unique promoters, they share a sequence identity of 70–80%, have similar cell targets and signal through the same serine-threonine kinase receptors (TGF-βR1, 2 and 3 in a manner that is unique from other cytokines.
TGF-β1 is the most abundant form of TGF-β and as such is often plainly referred to as TGF-β. It was originally identified for its ability to promote the growth of fibroblasts and assigned to chromosome 19 in humans and to chromosome 7 in mice.^157 ^,^^158 The human and mouse homologues differ by only one residue in their amino acid sequence. TGF-β1 is produced by every leukocyte lineage and has profound regulatory effects on a myriad of developmental, physiological and immune processes.^154 In general, TGF-β1 possesses both pro\- and anti-inflammatory activity depending on the presence of other growth factors and the activation or differentiation state of the target cell.^154 For example, at a site of developing inflammation TGF-β1 can modulate the expression of adhesion molecules, act as a chemoattractant, and orchestrate the immune response by suppressing or activating leukocytes.^154 ^,^^159 ^,^^160 This orchestration by TGF-β1 also applies to the Th cell subset paradigm. TGF-β1 can alter the production of, and response to, cytokines of both Th subsets and can therefore skew Th1 or Th2 immune responses as it sees fit depending on the composition of the inflammatory environment.^154 In fact, TGF-β1 secretion is a hallmark of a new candidate regulatory T cell subset called Th3 that also secretes IL-4 and IL-10.^161 ^-^^163 With such widespread responsibilities, it is no surprise that TGF-β1 knockout mice exhibit immune dysregulation and succumb to a progressive wasting syndrome shortly after birth.^164 ^-^^166 This mortal phenotype is characterized by changes in lymphoid organ architecture, including both the shrinking of the thymus and the swelling of lymph nodes, enhanced proliferation in vivo and defective mitogen responses in vitro. These mice also exhibit massive infiltrations of lymphocytes and macrophages in many organs resembling those found in autoimmune disorders.
TGF-β2, encoded on human and mouse chromosome 1, was originally identified as a suppressor of glioblastoma-derived T cells but is better known for its essential role in the developmental pathways of many tissues.^167 Accordingly, TGF-β2-deficient mice exhibit perinatal mortality and a wide array of tissue defects including craniofacial, skeletal, heart, eyes, ears and urogenital anomalies.^168 Likewise, TGF-β3, encoded on human chromosome 14 and mouse chromosome 12, appears to have an important role in certain developmental pathways as evidenced by TGF-β3-deficient mice that show severe defects in palate and lung morphogenesis and early death.^169 ^-^^170
Chemokines, their Receptors and their Genes
Chemokines are a family of low molecular weight chemotactic cytokines that regulate leukocyte migration through interactions with seven-transmembrane, rhodopsin-like G protein-coupled receptors.^172 ^-^^174 Chemokines have significant structural homology and overlapping functions and can often bind to more than one receptor. In general, ligand binding results in chemokine receptor activation hallmarked by the phosphorylation of carboxyl-terminal serine/threonine residues, dissociation of heterotrimeric G proteins, generation of inositol trisphosphate, intracellular calcium release and activation of protein kinase C (PKC.^175 With additional activation of the Ras and Rho families of guanosine triphosphate (GTP\-binding proteins, chemokine receptors mediate multiple signaling pathways that regulate a wide variety of cellular responses.^175
The chemokine field has developed at a rapid pace. This growth has caused classification headaches similar to those experienced by cytokine researchers decades ago. A classification system has been introduced to reduce confusion regarding the nomenclature of these molecules.^172 ^,^^174 Depending on the positions (or in one group the presence of the first two cysteine residues in the primary structure of these molecules, the chemokine family can be divided into four groups as outlined in Table 2 table/A13516/?report=objectonly. Unlike the cytokines listed in Table 1 table/A13506/?report=objectonly, the human chemokines listed in Table 2 table/A13516/?report=objectonly do not completely represent the murine chemokines because there are many differences in chemokine terminology between the two species and no matching homologues in some cases (see reference 172 and 174 for more details. The C group of chemokines (lacks cysteines one and three has been recently described and consists of at least two ligands (XCL, namely lymphotactin/XCL1 and SCM-1β/XCL2, which both bind XCR1.^176 Lymphotactin, coded for on human chromosome 1, attracts lymphocytes but not monocytes or neutrophils. The human CC chemokine group (no intervening amino acid includes at least 27 members (CCL, most of which are encoded on human chromosome 17, that bind at least 10 receptors (CCR. CC chemokine targets include monocytes, T cells, dendritic cells, eosinophils and NK cells. Representative CC chemokines include monocyte chemotactic protein (MCP\-1/CCL2, macrophage inflammatory protein (MIP\-1a/CCL3, MIP-1β/CCL4, regulated upon activation normally T expressed and secreted (RANTES/CCL5 and eotaxin/CCL11. The CXC group of human chemokines (one amino acid lies between the first two cysteines includes at least 14 ligands (CXCL. CXC chemokines are mostly encoded on human chromosome 4, bind at least five receptors (CXCR and mediate mainly neutrophil chemotaxis. The CXC chemokine group can be divided into two main categories based on the presence of the tripeptide Glu-Leu-Arg (ELR motif preceding the CXC motif. Representative CXC chemokines include IL-8/CXCL8 (ELR, monokine-induced by IFN-γ (MIG/CXCL9 (nonELR, IFN-γ inducible protein-10 (IP-10/CXCL10 (nonELR and stromal cell-derived factor-1 (SDF-1/CXCL12 (nonELR. Lastly, the sole CX3C chemokine (three intervening amino acids, namely fractalkine/CX3CL1, is encoded on human chromosome 16, binds CX3CR1 and attracts T cells and monocytes but not neutrophils.^177
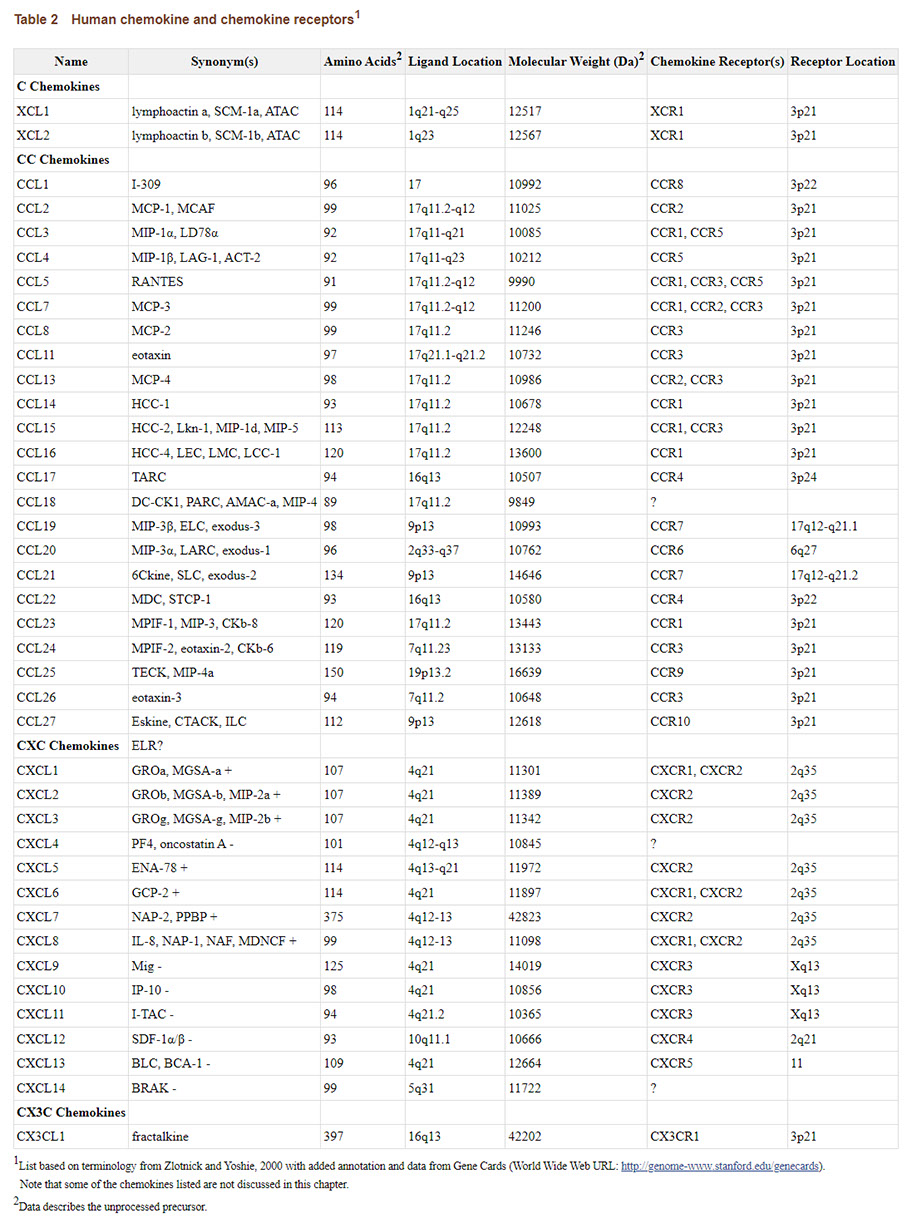
click here to open larger version of chart in larger window to view or download
Human chemokine and chemokine receptors1.
Our understanding of the roles of chemokines in physiological and pathological processes has advanced significantly. It has become clear that in addition to wound healing, metastasis, angiogenesis/angiostasis, cell recruitment, lymphoid organ development, and lymphoid trafficking,^172 ^,^^173 chemokines are fundamental in mediating innate and adaptive immune responses by their ability to activate cells of the immune system.^178 ^-^^180 As with the cytokines, chemokine gene disruption studies have confirmed most of these biological functions. For example, the MIP-1a/CCL3 (a monocyte and T cell chemoattractant knockout mouse was the first to be generated. While developmentally normal with no apparent lymphoid or myeloid defects, these mice were reduced in their ability to mount an inflammatory response to influenza infection.^181 In keeping with the role of eotaxin/CCL11 in attracting eosinophils, eotaxin/CCL11-deficient mice are reduced in their ability to mount eosinophil responses upon antigen challenge.^182 SDF-1/CXCL12-mutated mice exhibit a normal T cell compartment but have dramatic defects in B cell lymphopoiesis and myelopoiesis at the level of the bone marrow.^183 This result supports the critical role of SDF-1/CXCL12 as a modulator of progenitor cell development in the bone marrow. Knocking out the CXCR2 gene leads to impaired neutrophil migration in response to CXC chemokines, increases in circulating neutrophil numbers, and a dramatic increase in B cells.^184 ^,^^185 Knocking out another CXC chemokine receptor, CXCR5, leads to perturbations in B cell colonization of secondary lymphoid tissues indicating the importance of BCA-1/CXCL13 in B cell coordination.^186 ^,^^187 CCR7-deficient mice exhibit impaired lymphocyte migration, delayed antibody responses, no contact or delayed type hypersensitivity and defects in lymphoid architecture signifying an important role for CCR7 signaling in coordinating primary immune responses.^188 Lastly, mutating CCR1, CCR2 or CCR5 in mice impairs monocyte functions such as chemokine-dependent chemotaxis and alters the balance of Th1 or Th2 cytokine responses upon challenge with Th class-specific antigens or pathogens.^189 ^-^^194 With this result, it is interesting to speculate that chemokines play a pivotal role in regulatory and inflammatory responses just like cytokines. For example, chemokines and their receptors have been associated with predominant Th1 or Th2 responses as eluded to earlier.^6 ^,^^195 ^-^^204 This association is evidenced by the linkage of MIP-1a, CXCR3 and CCR5 to Th1-type cells and MCP-1, CCR3, CCR4, and CCR8 to Th2-type cells. Along with cytokine-cytokine receptor interactions, chemokine-chemokine receptor interactions may modulate and stabilize the extent of leukocyte migration to and the nature of inflammation at a developing pathological site. Considering the power of chemokines in recruiting immune cells, these proteins may augment immune responses (helpful or dangerous via normal immune surveillance mechanisms and may even determine the phenotype of responding cells (e.g., Th1 versus Th2 cells.
Concluding Remarks
As introduced earlier, the immune system is essentially a network supersystem utilizing specialized languages for communication between cells. This chapter focused on only the powerful language of cytokine and chemokine signaling but others exist such as hormone, neurotransmitter, complement and allergic mediator production. At their discretion, immune cells can listen to or send these signals as required to reach cells in the immediate microenvironment or throughout the organism. Just as miscommunication can crash modern electronic networks, the information super-highway of the immune system is not without its vulnerabilities. The knockout models discussed above exemplify the dramatic consequences of man-made alterations to immune network communication. The permanent absence of a particular cytokine at a whole-body level, however, may mask more subtle defects in the role of the conventional signaling component. Similarly, natural defects in communication appear to drive the pathogenesis of autoimmunity. In cases such as this, however, headway is being made in understanding how the immune system communicates and many therapies are being developed that may reset dangerous crashes and return an organism to ‘online’ protective status. A new understanding of the language used by cells of immune system to achieve this protection is emerging and cytokines and chemokines will certainly be at the heart of our progress in communication.












