Page Synopsis: Xyrem, for instance appears promising. This page is a 'kitchen sink' where I put all the CFS players in the game on the page, unranked. The therapies I recommend have their own pages. This exhaustive list is for therapies to try if the other (paged) therapies fail. Also it may educate you to find medicine more specific to your condition. All that to say, this page is extremely long and perhaps not required reading
Skill Level 5
Relevance:4 Technical Level:3
With all the medicines to try, surely something must help as other patients have been helped
page 33 CFS> ALLOPATHIC MEDICINES > OTHER MEDICINES
page 32
page 34
Intravenous Cyclophosphamide in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. An Open-Label Phase II Study
https://www.frontiersin.org/articles/10.3389/fmed.2020.00162/full
Results: The overall response rate by Fatigue score was 55.0% (22 of 40 patients). Fatigue score and other outcome variables showed significant improvements compared to baseline. The SF-36 Physical Function score increased from mean 33.0 at baseline to 51.5 at 18 months (all patients), and from mean 35.0 to 69.5 among responders. Mean steps per 24 h increased from mean 3,199 at baseline to 4,347 at 18 months (all patients), and from 3,622 to 5,589 among responders. At extended follow-up to 4 years 68% (15 of 22 responders) were still in remission. Patients positive for HLA-DQB1*03:03 and/or HLA-C*07:04 (n = 12) had significantly higher response rate compared to patients negative for these alleles (n = 28), 83 vs. 43%, respectively. Nausea and constipation were common grade 1–2 adverse events. There were one suspected unexpected serious adverse reaction (aggravated POTS) and 11 serious adverse events in eight patients.
Conclusion: Intravenous cyclophosphamide treatment was feasible for ME/CFS patients and associated with an acceptable toxicity profile. More than half of the patients responded and with prolonged follow-up, a considerable proportion of patients reported ongoing remission. Without a placebo group, clinical response data must be interpreted with caution. We nevertheless believe a future randomized trial is warranted
![]()
Preclinical evaluation of the abuse potential of Pitolisant, a histamine H3 receptor inverse agonist/antagonist compared with Modafinil
https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1111/bph.12149
Histamine H3 autoreceptors control histamine synthesis and release from tuberomamillary neurons, a brain system involved in the control of wakefulness, attention, learning and other cognitive functions (Schwartz et al., 1991; Haas and Panula, 2003; Lin et al., 2011). Therefore the use of H3 receptor inverse agonists, a class of compounds reversing the high constitutive activity of the native receptors (Morisset et al., 2000), appears as a useful therapeutic approach to enhance wakefulness in states of excessive daytime sleepiness such as narcolepsy, obstructive sleep apnoea or Parkinson's disease (Lazewska and Kiec-Kononowicz, 2010; Kuhne et al., 2011; Leurs et al., 2011).
The first compound of this class to be introduced in the clinics, PitolisantINN (formerly named tiprolisant, BF2.649, [1-{3-[3-(4-chlorophenyl)propoxy]propyl}piperidine, hydrochloride]), a potent and highly selective non-imidazole histamine H3-receptor inverse agonist (Ligneau et al., 2007b), constitutes a promising tool for the treatment of narcolepsy as shown in an animal model of this pathology, the orexin−/− mouse as well as in clinical trials (Lin et al., 2008, Schwartz, 2011). Dopamine-releasing agents currently used to fight against daytime somnolence in narcolepsy comprise amphetamine derivatives, sodium oxybate and Modafinil which both suffer, to a variable degree, from abuse liability
Colloidal silver
Drink a quart of colloidal silver a day for 30 days and you can get rid of most anything that is a virus. 10 days is enough for almost everything, but when a threat is very serious 30 days will make sure
![]()
THE 12-STEP SHOEMAKER PROTOCOL
Very Severely Ill "ME/CFS" Patient Gets a New Diagnosis, New Treatment Approach & Major Improvement | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
![]()
Therapeutic Treatment of Long Covid as applied to chronic fatigue syndrome
1) BC 007
2) Tollovid
3) Extracorporeal Apheresis
4) Ivermectin
5) ct38
7) Transcranial Direct Current
8) Long COVID: Latest on Research and Treatments
9) https://www.healthrising.org and https://phoenixrising.me
1) BC 007
1a) Further patients benefit from drug against Long COVID › Friedrich-Alexander-Universität Erlangen-Nürnberg
https://www.fau.eu/2021/08/27/news/research/further-patients-benefit-from-drug-against-long-covid
1b) Berlin Cures...? Could BC 007 Help With Long COVID and ME/CFS?
https://www.healthrising.org/blog/2021/12/30/bc-007-berlin-cures-long-covid-chronic-fatigue-syndrome
1c) BC 007 Long Covid 2022
1d) bc 007 chronic fatigue syndrome
1e) BC 007 - AdisInsight
https://adisinsight.springer.com/drugs/800047946
1f) Seite nicht vorhanden - Universitätsklinikum Erlangen
https://www.augenklinik.uk-erlangen.de/forschung-und-lehre/recover-projekt/medien
1g) BC 007: New drug combats fatigue | In Good Shape - The Health Show | DW | 06.03.2022
https://www.dw.com/en/bc-007-new-drug-combats-fatigue/av-60915684
1h) BC007_miracle_in_need_of_explanation_141221.pdf
https://www.kinder-verstehen.de/wp-content/uploads/BC007_miracle_in_need_of_explanation_141221.pdf
2) Tollovid
2a) Tollovid chronic fatigue syndrome
2b) Case Study #2: PASC (Long COVID) and its resolution with Tollovid®
2c) Amazon.com: Tollovid ™ Maximum Protection Natural Dietary Supplement for Immune Support : Health & Household
https://www.amazon.com/Tollovid-Maximum-Protection-Natural-Supplement/dp/B09G7VFB58
2d) Fenben LAB Fenbendazol 444mg, Purity >99%, by Fenben Lab, Certified Third-Party Laboratory Tested, Analysis Report Included, 90 Caps: Amazon.com: Industrial & Scientific
2e) Todos Medical Releases Preliminary Data From IRB-Waived Tollovid® Market Research Study in Acute and Long COVID :: Todos Medical Ltd. (TOMDF)
2f) Tollovid™ + Long COVID: Exploring Viral Persistence
https://todosmedical.com/long-covid-data-report
2g) Todos Medical Reports 2nd Long COVID Case Study and
3) Extracorporeal Apheresis
3a) Chronic post-COVID-19 syndrome and chronic fatigue syndrome: Is there a role for extracorporeal apheresis?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8209771
3b) extracorporally filtered and cleaned with the use of Heparin, which is then removed again before the blood is being fed back into the body. The Heparin binds to various inflammation inducing components in the blood plasma
3c) Apheresis
4) Ivermectin
4a) FLCCC Alliance (Front Line COVID-19 Critical Care Alliance, Long Covid therapy protocol including Ivermectin
https://covid19criticalcare.com/covid-19-protocols/i-recover-long-covid-treatment
I-RECOVER Long COVID Treatment
Long Haul COVID Syndrome (LHCS)—commonly known as long COVID—is characterized by prolonged malaise, headaches, generalized fatigue, sleep difficulties, hair loss, smell disorder, decreased appetite, painful joints, dyspnea, chest pain and cognitive dysfunction.
Up to 80% of patients experience prolonged illness after COVID-19. Long COVID is not only seen after COVID infection but is also being observed in some people who have received vaccines (likely due to monocyte/microglia activation by the spike protein from the vaccine). Long COVID may persist for months after the acute infection and almost half of patients report reduced quality of life.
Patients may suffer prolonged neuropsychological symptoms, including multiple domains of cognition. A puzzling feature of long COVID is that it is not predicted by initial disease severity; it frequently affects mild-to-moderate cases and younger adults who did not require respiratory support or intensive care.
The symptom set of long COVID is, in the majority of cases, very similar to chronic inflammatory response syndrome (CIRS)/myalgic encephalomyelitis/chronic fatigue syndrome. An important differentiating factor from CIRS is the observation that long COVID continues to improve on its own, albeit slowly in the majority of cases.
Another important observation is that long COVID includes more young people compared to severe COVID, which affects older people or persons with co-morbidities.
Long COVID is highly heterogeneous and likely results from a variety of pathogenetic mechanisms. Furthermore, it is likely that delayed treatment (with ivermectin, etc.) in the early symptomatic phase results in a high viral load (high spike protein load), which increases the risk and severity of long COVID.
The approach outlined in the I-RECOVER: Long COVID Treatment Protocol is a consensus based on a collaboration led by Dr. Mobeen Syed (“Dr. Been”), Dr. Tina Peers, and the FLCCC Alliance. The approach should be individualized according to the patient’s clinical signs and symptoms.
As with all FLCCC protocols, aspects may change as scientific data and clinical experience in this condition evolve. Thus it is important to check back frequently to receive notification of any protocol changes
5) ct38
5a) Clinical trial provides preliminary evidence of a cure for myalgic encephalomyelitis / chronic fatigue syndrome (ME/CFS) and Long Covid
5b) AXA1125 ct38 New “Long Covid” Treatment Looks to Improve Patient Feeling and Function
7) Successful Treatment of Post-COVID Symptoms With Transcranial Direct Current Stimulation
8a) Long COVID: Latest on Research and Treatments
8b) Long Covid patients, in search of relief, turn to private company
https://www.nbcnews.com/health/health-news/long-covid-patients-private-company-help-rcna9035
8c) A systematic review of nutraceutical interventions for mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome - PMC
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7890871
8d) Successful treatment of prolonged COVID-19 with Bamlanivimab in a patient with severe B-Cell aplasia due to treatment with an anti-CD20 monoclonal antibody: A case report - PubMed
https://pubmed.ncbi.nlm.nih.gov/34868871
8e) Long COVID treatment protocol - Google Search
https://www.google.com/search?sxsrf=ALiCzsb1PyMGKqg_DGsxnF12Np6dzCNNoA:1658769392714&q=Long+COVID+treatment+protocol&sa=X&ved=2ahUKEwjz1KrDxZT5AhWjD0QIHd09Bh0Q1QJ6BAgqEAE&biw=1498&bih=961&dpr=0.9
8f) Treatment for COVID | Johns Hopkins Medicine
https://www.hopkinsmedicine.org/health/conditions-and-diseases/coronavirus/coronavirus-treatment-whats-in-development
8g) Treating patients with long COVID
https://www.apa.org/monitor/2021/07/treating-long-covid
8h) 11 things doctors have learned about long COVID
https://health.ucdavis.edu/news/headlines/11-things-doctors-have-learned-about-long-haul-covid/2022/02
8i) Can Long COVID Be Treated? - The Atlantic
https://www.theatlantic.com/magazine/archive/2021/04/unlocking-the-mysteries-of-long-covid/618076/
8j) Successful treatment of prolonged COVID-19 with Bamlanivimab in a patient with severe B-Cell aplasia due to treatment with an anti-CD20 monoclonal antibody: A case report - ScienceDirect
https://www.sciencedirect.com/science/article/pii/S2213007121002227
8k) One U.K. trial is transforming COVID-19 treatment. Why haven't others delivered more results? | Science | AAAS
https://www.science.org/content/article/one-uk-trial-transforming-covid-19-treatment-why-haven-t-others-delivered-more-results
8l) Frontiers | Case Report: Neutralization of Autoantibodies Targeting G-Protein-Coupled Receptors Improves Capillary Impairment and Fatigue Symptoms After COVID-19 Infection
https://www.frontiersin.org/articles/10.3389/fmed.2021.754667/full
9) https://www.healthrising.org and https://phoenixrising.me
9a) https://www.healthrising.org
9b) Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums
9c) Chronic Fatigue Syndrome (ME/CFS) Research | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/forums/chronic-fatigue-syndrome-me-cfs-research.15
9d) Treatment | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/forums/treatment.11
9e) Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/#getting-better.1
9f) Recovery Stories | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/forums/recovery-stories.66/
9g) Health News | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/forums/health-news.101/
9h) General Discussion | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums
https://www.healthrising.org/forums/forums/general-discussion.109/
9i) https://phoenixrising.me
10) https://forums.phoenixrising.me
![]()
Endotherapia GEMSP
Endotherapia (GEMSP) as a customized treatment for ME/CFS
https://forums.phoenixrising.me/threads/endotherapia-gemsp-as-a-customized-treatment-for-me-cfs.51962
mentioned alongside Rituximab in this paper from Molecular Neurobiology as a potential treatment for ME/CFS. Early trials have shown good results in MS (1), ALS (2), and RA (3) without toxicity. Followup showed continued benefit in MS patients (4)
Endotherapia is a subligual tablet with a blend of fatty acids, antioxidants, aminco acids, and radical scavengers customized to one's immunological blood work, brain imaging, and symptoms. It's delivered via poly-L-lysine (which allows for better cell permeability). The end result is a reduction in oxidative stress and inflammation, and an improvement in neuroprotection.
I can see this treatment fitting in well with the "refill the tank" step of Dr Naviaux's proposed 3 step protocol.
Endotherapia was developed by professor Michel Geffardat at the IDRPHT in France.
Here is a breakdown of the ingredients used in Endotherapia by disease. The first article suggests using the MS preparation (GEMSP) for ME/CFS. I imagine it would be further customized based on the individual.
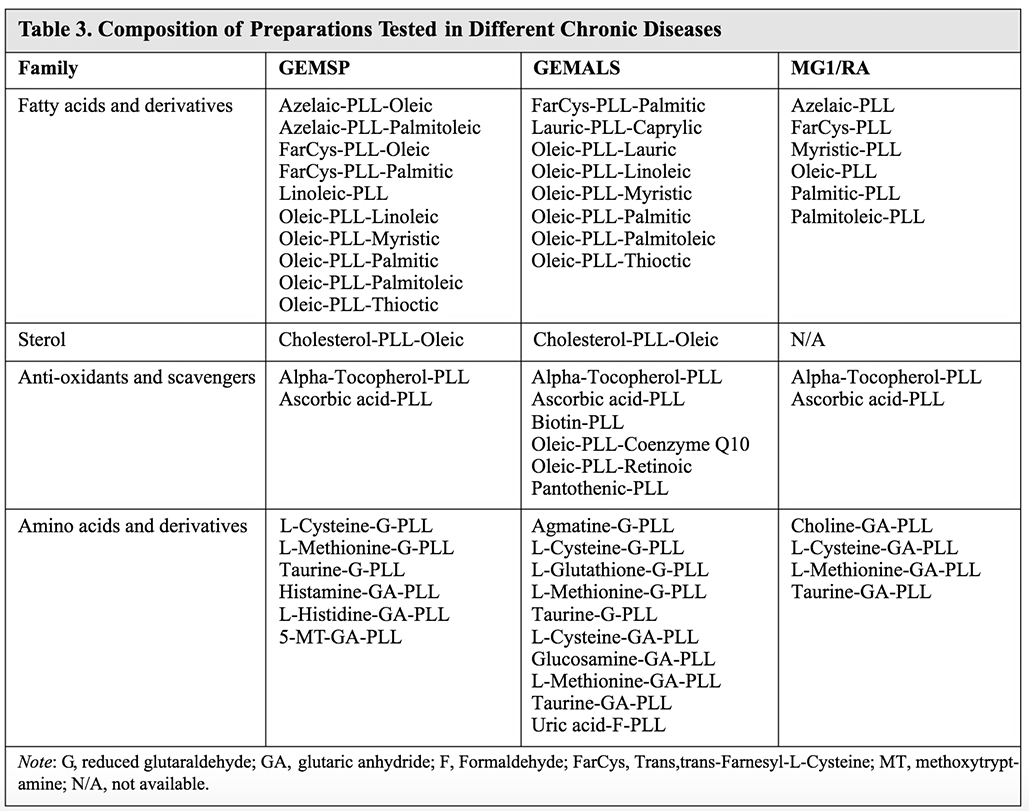
![]() xclick here to close and return to reportclick for full size, click 'x' button to closeingredients used in Endotherapia
xclick here to close and return to reportclick for full size, click 'x' button to closeingredients used in Endotherapia
More on Endotherapia
From "The Emerging Role of Autoimmunity in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/cfs)"
Endotherapia is an immunopathological strategy addressing pathology which seems to underpin chronic incurable diseases whose etiology is multifactorial.
It involves the combination of an evaluation of circulating immunoglobulins directed against specific neo-epitopes that created ROS elevation.
GEMSP is a preparation of numerous small molecules, including fatty acids, anchorage molecules, antioxidants, radical scavengers, amino acids, ligated to linear chain of poly-L-lysine (PLL) which are non-immunogenic and inhibit inflammation and O&NS processes. Each individual linkage affords significant advantages.Importantly, it prevents metabolic degradation of the linked molecules and enables a long half-life and confers stability on the various linked chemical entities. Membrane permeability is increased and the induction of various viral and bacterial components. These features combine to induce neuroprotection.
Full article
And "Endotherapia: A New Frontier in the Treatment of Multiple Sclerosis and Other Chronic Diseases"
Endotherapia is a new biomedical and therapeutic approach for the treatment of chronic diseases, including autoimmune, neurodegenerative, and proliferative diseases. It is based on a pathophysiological concept that takes into account genetic predisposition and immunological events, together with bacterial and environmental factors.
It includes: a) clinical aspects, paraclinical exams (Magnetic Resonance Imaging, MRI),and biological examination, allowing an exact diagnosis of the disease; b) the identification of specific circulating antibodies in the serum of patients suffering from chronic diseases; and c) the use of therapeutic tools,such as small compounds linked to poly-L.Lysine(PLL), whose physiological actions are well known.Here, we focus on two specific aspects of Endotherapia:1) the identification of circulating antibodies as a means to follow up on chronic pathology and 2) the therapeutic drugs used against those pathologies [MS, amyotrophic lateral vv(ALS), and rheumatoid arthritis (RA)
Full article
An ALS patient who traveled from Australia to France for the treatment reports good results:
For me, I am now entering into week 12 of my Endotherapy medication. I take it 3 times a day. In terms of results, I was advised (based on previous patients) not to expect to notice too much in the first 3 months. So, I impatiently complied with the regime.
So far so good...
Within myself I can definitely say that I feel as though any progression of the disease has slowed considerably. I could almost say that it's likely at a stand-still (but I'm trying not to get too excited too early). Energy levels are rising and very rarely do I need to rest during the day. My friends and family - especially some I haven't spoken to in a while- have commented on many occasions that my speech is a lot clearer and has picked up speed. I have noticed this also, however it is not yet consistent. On occasions where I am exhausted my language reverts back to a mild and sometimes moderate speech deficit (slurred, slow, and mispronounced in nature - comparable to my prior baseline). On the up side, every other day feels like I've gained a little more of my ‘self’ back
![]()
GcMAF
DESCRIPTION
GcMAF is a naturally occurring substance in the human body which destroys pathogens by activating macrophages. The acronym stands for Gc (a vitamin D binding protein) Macrophage Activating Factor.
BACKGROUND
In the early 1990s, Dr. Nobuto Yamamoto, director of the Division of Molecular Immunology and Immunotherapy at the Socrates Institute for Therapeutic Immunology in Philadelphia, Pennsylvania, discovered a substance that inhibited tumor production in mice. Throughout the 1990s Dr. Yamamoto continued his research, expanding it to cases of cancer in humans. But it wasn't until 2008 that Dr. Yamamoto published his groundbreaking study on breast cancer. In this study, weekly injections of GcMAF were given to 16 breast cancer patients. Within three months the tumors were eradicated, with no recurrence over the next four years.
Subsequent studies with GcMAF used for colorectal and prostate cancer yielded similar results. In all cases the tumors disappeared with no recurrence. The rationale behind the success of GcMAF is that when the naturally occurring Gc protein is destroyed by cancer cells (more specifically by an enzyme called nagalase) it hamstrings the immune system's ability to make sufficient tumor-destroying macrophages. The result is an immunosuppressed state which allows the cancer to spread. Injecting GcMAF into cancer patients restores the compromised immune system, which then successfully combats the cancer. CFS Treatment Guide Verrillo/395
The implications for other immune compromised patients are enormous. In 2009 Dr. Yamamoto published a study demonstrating that after fewer than 18 weekly administrations of GcMAF, HIV infection was also completely eradicated. According to the study, "no recurrence occurred and their healthy CD + cell counts were maintained for 7 years."
USES IN CFS/ME
Given the spectacular results of the Yamamoto studies one would have expected to have seen front-page spreads in the New York Times. However, apart from Reuters, the news agencies barely took notice. As of today, no clinics in the U.S. are using GcMAF as a treatment for cancer. Several prominent CFS/ME physicians, however, have begun using GcMAF for patients who test high in nagalase.
Dr. Kenny De Meirleir treated 108 of his CFS/ME patients with weekly administration of GcMAF. This group of patients showed high amounts of nagalase, which Dr. De Meirleir notes can be produced by intestinal bacterial infections as well as herpes and retroviral infections. (Dr. Chia also points out that nagalase can be elevated as a result of enteroviral infections, which produce small intestinal bacterial overgrowth (SIBO) leading to subsequent immune system dysregulation.) After an average of 15 weeks of treatment, 68 of the 108 patients reported significant improvement in fatigue, sleep, pain, cognitive impairment, orthostatic intolerance, and digestive disturbances. (See below for a link to Dr. De Meirleir's presentation.)
Because GcMAF causes an increase in immune system activation, Dr. De Meirleir recommends starting with a very low dose of GcMAF. Some CFS/ME patients have undiagnosed infections which could lead to Immune Reconstitution Inflammatory Syndrome (IRIS). Once the immune system is stimulated, symptoms due to co-infections can worsen. Of Dr. De Meirleir's 108-patient cohort, 20-30% of them experienced IRIS.
Dr. Cheney has also begun to treat patients with GcMAF, as well as with a natural yogurt probiotic MAF (MAF 314) developed by Professors Ruggiero and Pacini in Italy. GcMAF demonstrated a response rate of 79% (15 out of 19 patients), which is similar to Dr. De Meirleir's results. The oral MAF 314 demonstrated a response rate of 76% over a period of only 28 days.
PROTOCOL:
There are several protocols currently in use. Most CFS physicians begin with 0.20 - 0.25 ml via injection (IM) weekly. Dr. Cheney starts his severely ill patients at a much lower dose administered sublingually, then gradually increases the dose. Typically, the full course of treatment is 8-20 weeks. In order to be effective, GcMAF requires adequate levels of vitamin D. Patients should be tested for vitamin D levels prior to beginning treatment. (Optimal ranges fall between 42 and 60). Patients should also be tested for nagalase levels before treatment and on a monthly basis after beginning GcMAF.
Physicians may recommend concurrent antiviral treatment with Nexavir if the viral load is high. Artesunate may also be prescribed, as well as adjunctive supplementation with B vitamins. CFS Treatment Guide Verrillo/396
Anti-inflammatory drugs, such as corticosteroids (prednisolone, prednisone, etc.) and NSAIDs (ibuprofen, aspirin, etc.) should be avoided while taking GcMAF as these will interfere with the treatment. Morphine analogs (oxycodone, tramadol, etc.), beta blockers, and cytotoxic medications (Sendoxan, Vepesid, Taxol, etc.) should be avoided. Aspartame and carrageenan, two food additives, can also block GcMAF.
GcMAF is contraidicated for patients with MS.
PROS AND CONS
GcMAF is an experimental drug, which means not much is known about its effects on the CFS/ME population other than the few studies performed by Drs. De MeirLeir and Cheney. As with other medications, patients report a wide range of responses, from feeling significantly worse to an almost miraculous recovery of strength and energy. Frequently, a patient will notice improvement over the first six weeks, and then experience a decline. This may be due to exhaustion of vitamin D reserves. For this reason, continuing supplementation with vitamin D may be advised.
AVAILABILITY AND COST
Drs. Cheney, Enlander and De Meirleir are currently using GcMAF with their CFS/ME patients. The price for 2.2 ml of GcMAF (about 8 doses at .25 per dose) is roughly $1000 ($800 euros). Because of the risk of IRIS, it is not recommended that CFS/ME patients take GcMAF without the supervision of a knowledgeable physician. MAF 314 can be obtained from Dr. Cheney's clinic for $3500. Dr. Enlander is currently developing a less expensive form of probiotic MAF (MAF 378) in New York. The test for nagalase levels can be ordered by physicians from Health Diagnostics. It costs $65. GcMAF must be refrigerated
TESTING
Health Diagnostics and Research Institute (formerly Vitamin Diagnostics, Inc.)
South Amboy Medical Center
540 Bordentown Ave., Suite 2300
South Amboy, New Jersey 08879
Telephone: (732) 721-1234
Fax: (732) 525-3288
Testing for nagalase.
SUPPLIERS
GcMAF
Clos de Balade 21
1140 Evere
Brussels
Belgium
Website: http://www.gcmaf.eu/info/
BGLI Bio Group Laboratories
Tel: 31-3576-00-176 (GMT+2) (Netherlands)
Website: http://www.bgli.nl/ (There is a contact form on the site) CFS Treatment Guide Verrillo/397
FURTHER READING
Dr. Kenny De Meirleir's talk on GcMAF and its use in treating CFS/ME: http://cfspatientadvocate.blogspot.com/2011/11/mt-sinai-mecfs-conference-de-meirleir.html
Dr. Cheney's GcMAF studies: http://www.cheneyclinic.com/gcmaf-studies-presented-at-iacfsme-meetings-in-ottawa/833
Excellent information on GcMAF, including where to find clinics in Europe that use GcMAF, patient forums, and purchasing information: http://www.gcmaf.eu/info/
European lab that offers testing for nagalase: http://www.europeanlaboratory.nl/
Phoenix Rising forum threads on GcMAF discussing Kenny De Meirleir's use of GcMAF, where to purchase, and how to obtain testing for nagalase: http://forums.phoenixrising.me/showthread.php?6019-GcMAF-for-XMRV-Gc-protein-derived-macrophage-activating-factor-anyone-taking-it/page116
and
http://forums.phoenixrising.me/showthread.php?6019-GcMAF-for-XMRV-Gc-protein-derived-macrophage-activating-factor-anyone-taking-it/page117
Patient thread on MAF 314: http://phoenixrising.me/forums/showthread.php?14838-MAF-314
"Who Responds to GcMAF." Very technical discussion of gene types http://www.cfscentral.com/2011/01/who-responds-to-drug-gcmaf.html
Good article about cancer and GcMAF by Bill Sardi http://www.thenhf.com/article.php?id=633
Another good follow-up article by Bill Sardi: http://www.thenhf.com/article.php?id=771
Cancer and GcMAF: http://www.center4cancer.com/glyco-protein.php
Professor Ruggiero's website on GcMAF and MAF 314 http://www.marcoruggiero.org/pdf/Oct%2022.pdf
“Compassionate Use Treatment of CFS with GHP (GcMAF)” Dr. Paul Cheney, Sept. 2011. http://www.gcmaf.nl/documents/research/Compassionate%20use%20Treatment%20of%20CFS%20with%20GHP%20(%20GcMAF%20).pdf
Dr. Cheney's pilot study of GcMAF.
PATIENT EXPERIENCES
A Cheney patient blog about her experience with GcMAF. This blog is very detailed, with information about dosage, testing and patient responses. http://nopostergirl.com/2011/04/16/the-post-appointment-post/
Cheney patient blog on GcMAF http://blogwormwood.blogspot.com/2011/05/gcmaf.html
RESEARCH
Yamamoto N, Suyama H, Yamamoto N, Ushijima N. “Immunotherapy of metastatic breast cancer patients with vitamin D-binding protein-derived macrophage CFS Treatment Guide Verrillo/398
activating factor (GcMAF).” Int J Cancer. 2008 Jan 15;122(2):461-7. http://www.ncbi.nlm.nih.gov/pubmed/17935130 (Abstract)
Yamamoto N, Suyama H, Koga Y. “Immunotherapy of metastatic colorectal cancer with vitamin D-binding protein-derived macrophage-activating factor, GcMAF.” Cancer Immunol Immunother. 2008 Jul;57(7):1007-16. http://www.ncbi.nlm.nih.gov/pubmed/18058096 (Abstract)
Yamamoto N, Suyama H, Yamamoto N, “Immunotherapy for Prostate Cancer with Gc Protein-Derived Macrophage-Activating Factor, GcMAF.” Transl Oncol. 2008 Jul;1(2):65-72. http://www.ncbi.nlm.nih.gov/pubmed/18633461 (Abstract)
Yamamoto N, Ushijima N, Koga Y. “Immunotherapy of HIV-infected patients with Gc protein-derived macrophage activating factor (GcMAF).” J Med Virol. 2009 Jan;81(1):16-26. http://www.ncbi.nlm.nih.gov/pubmed/19031451
EPOGEN (PROCRIT)
DESCRIPTION
Epogen is human erythropoietin, a glycoprotein that controls red blood cell production in bone marrow.
BACKGROUND
Epogen has been approved for treating anemia caused by kidney failure or chemotherapy, and after certain types of surgery in order to decrease the need for blood transfusions. Epogen has also been used to treat orthostatic hypotension, a condition in which blood pressure drops upon standing, causing light-headedness, dizziness or fainting.
USES IN CFS/ME
Dr. Hugh Calkins, a cardiologist at Johns Hopkins, has observed that CFS/ME is closely associated with neurally-mediated hypotension (NMH). He found that 90% of CFS/ME patients have some form of NMH. This observation was independently confirmed by Dr. David Streeten who discovered that among two groups of patients with orthostatic intolerance (OI), one had an abnormally low volume of red blood cells, and another had low plasma circulation. As it turned out, both of these were people with CFS/ME. Dr. Streeten treated these patients using protocols and medications for OI, including Florinef, beta-blockers and epogen to raise standing blood pressure. It wasn't until he was contacted by Dr. Bell, whose CFS/ME patients were exhibiting the same symptoms, that Dr. Streeten realized he had successfully treated a group of CFS/ME patients. Since that time, most doctors in the CFS/ME community have incorporated NMH treatments into their protocols.
In an important study conducted at the University of Miami, Hurwitz et al observed that 60-70% of CFS/ME patients show below normal red blood cell volume. The authors concluded that “the findings indicate that lower cardiac volume levels, displayed primarily by subjects with severe CFS, were not linked to diminished cardiac contractility levels, but were probably a consequence of a co-morbid hypovolaemic condition.” This study was significant because it proved that diminished blood volume was pervasive among CFS/ME patients. Unfortunately, while Procrit increased red blood cell volume, fatigue and exercise intolerance did not improve in the treated group.
PROTOCOL
Very few CFS/ME doctors use Procrit. Dr. Shoemaker treats his patients with 8,000 units of Procrit twice a week for five doses and then decreases the dosage to 4,000 to 6,000 every three to five days. This rather intensive protocol has not gone without criticism from doctors who point out that the “off label” use of Procrit for non-anemic patients is risky.
PROS AND CONS
Procrit is by no means a proven treatment for the correction of low blood volume in CFS/ME. In fact, even weeks after correcting low red blood cell volume in CFS/ME patients, Hurwitz et al noted that there was no corresponding reduction in symptoms. Procrit includes a boxed warning that “ESAs [Erythropoiesis-Stimulating Agents ] increase the risk of death, myocardial
CFS Treatment Guide Verrillo/389
infarction, stroke and thrombosis.” Needless to say, CFS/ME patients should give careful thought to the possible risks before embarking on a protocol that includes Procrit.
FURTHER READING
Safety update from the makers of Procrit: http://www.procrit.com/
CFS/ME Forum review of treatments for NMH in CFS/ME: http://www.ncf-net.org/forum/orthostatic98.htm
Fall 2002 CFIDS Chronicle Q&A with Dr. Hurwitz about Procrit. http://www.cfids.org/archives/2002/2002-4-article01.asp
RESEARCH
Hurwitz, Barry E., Virginia T. Coryell, Meela Parker, Pedro Martin, Arthur LaPerriere, Nancy G. Klimas, George N. Sfakianakis and Martin S. Bilsker. “Chronic fatigue syndrome: illness severity, sedentary lifestyle, blood volume and evidence of diminished cardiac function.” Clinical Science (2010) 118, (125–135) (Printed in Great Britain) http://www.clinsci.org/cs/118/cs1180125.htm
![]()
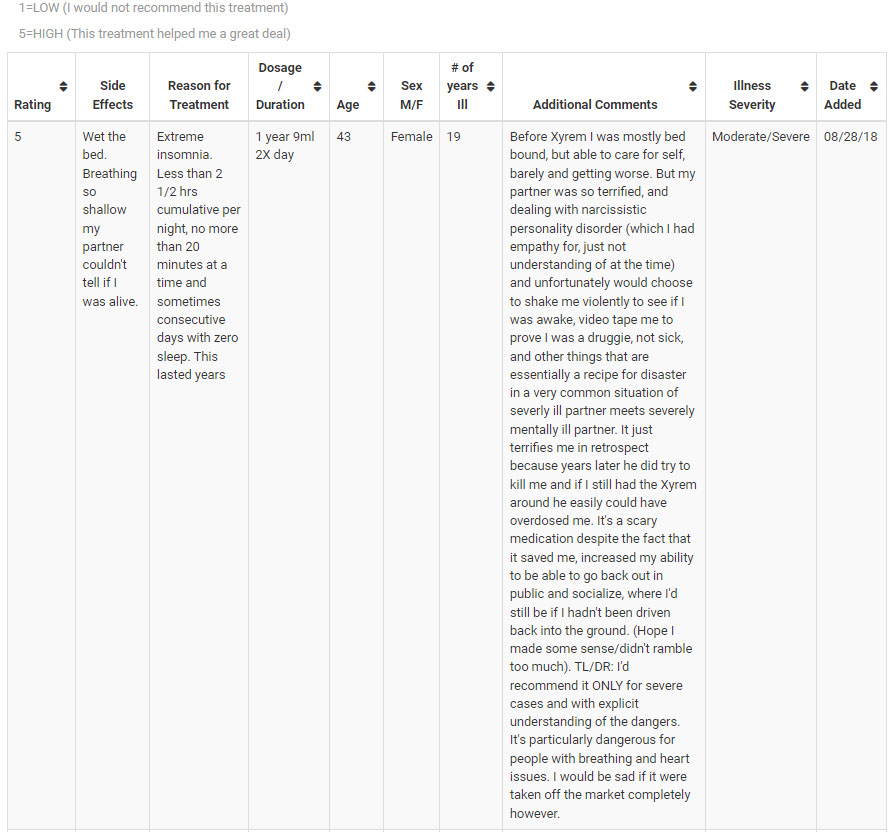
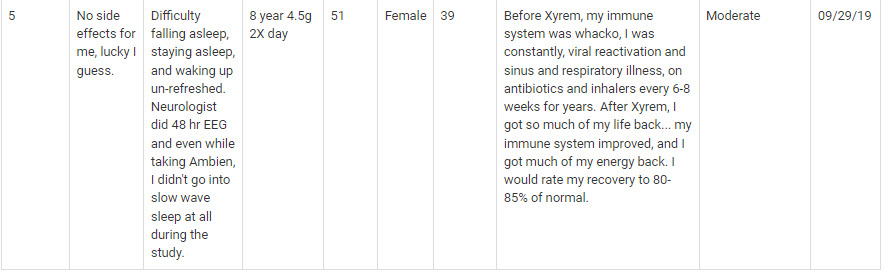
Xyrem
Xyrem (Sodium Oxybate)
XyremXyrem ( gamma-hydroxybutyric acid or GHB https://phoenixrising.me/myalgic-encephalomyelitis-chronic-fatigue-syndrome-mecfs-treatments/sleep/a-prescription-for-sleep/treating-chronic-fatigue-syndrome-mecfs-and-fibromyalgia-xyrem
a neurochemical involved in regulating metabolism which is also able to affect sleep. Sodium oxybate is the active ingredient in Xyrem. Xyrem has been approved to treat narcolepsy (severe daytime sleepiness) and cataplexy (sudden muscle weakness).
Zyrem was developed by the Office of Orphan Products Development (OOPD) – a department of the FDA dedicated to producing drugs for rare conditions. Acquired by Jazz Pharmaceuticals in the US in 2005 Xyrem is currently approved to treat narcolepsy. Currently undergoing Phase III trials for fibromyalgia (FM), Xyrem is also being studied in CFS, Parkinson’s, schizophrenia, essential tremor and others.
Xyrem May Work in ME/CFS/FM Because..
It is able to reduce the frequency of abnormal brainwaves (called alpha intrusions) that appear to impair deep sleep in many CFS and fibromyalgia patients. It is also one of the only drugs known to improve both sleep and reduce pain. Xyrem may enhance the activity of two neurotransmitters, dopamine and serotonin, both of which may be deficient in ME/CFS as well as growth hormone production. The highest concentrations of GHB are found in two areas of the brain; the hypothalamus and basal ganglia, that are of interest to CFS and FM researchers.
ME/CFS Physicians Report
Dr. Teitelbaum flatly states “Xyrem is the most effective way known to increase deep sleep and raise growth hormone”. Dr. Peterson reported that to his ‘amazement’ Xyrem helped with both sleep and pain in his patients with sleep disorders. Drs. Ross and Marion Hauser call it ‘probably one of the safest and most effective sleep aids that we know of.” They believe it may enhance growth hormone levels. Dr. Klimas notes that Xyrem it induces ‘slow wave’ sleep – the type of sleep most ME/CFS patients have the most trouble achieving.
Chronic Fatigue Syndrome and Fibromyalgia Studies
Currently in Phase III Clinical Trials for FM, Xyrem has been the focus of several extensive studies.A large 2012 trial found that from 42-50% of patients reported a greater than 30% reduction in pain. A 2011 trial containing over 500 patients found that from 55-60% of patients experienced a 30% drop in pain and significantly reduced fatigue and sleep disturbances. Subjective sleep quality was increased in a 2009 FM study.
A 2010 Spitzer retrospective study found that 60% and 75% of 118 CFS/FM patients experienced significant reductions in pain and/or fatigue. Two studies have found improved sleep and about a thirty percent reduction in fatigue and pain scores in fibromyalgia. Of particular interest was Xyrem’s abiity to reduce the frequency of anomalies observed in both FM and ME/CFS during sleep called alpha intrusions. Alpha intrusions involve the appearance of unusual high frequency brainwave patterns that are believed to disrupt deep sleep.
Dose
Dr. Teitelbaum recommends 9 cc’s (4.5 grams) at bedtime and then about 4 hours later if needed. Xyrem is fast acting and should be taken in bed.
Side Effects
Xyrem can be habit forming. Patients in clinical trials reported confusion (2.5%), depression (3.5%), incontinence at some point (7%), sleepwalking (4%). Headache (22%), nausea (21%) and dizziness (17%) and others were also found.
Warning
Do not take other sleep enhancing substances (alcohol, pain medication, muscle relaxants, sedative hypnotics, etc.) when taking Xyrem. Xyrem should be discontinued gradually. Rinse well with water and swallow after taking as Xyrem can damage tooth enamel.
Others
GHB is known as the GHB is known as the date rape drug because of its ability to induce amnesia when combined with alcohol. It can only be obtained from a special compounding pharmacy. According to Dr. Staud, Xyrem’s cost is now up to about $30,000 a year. Jazz Pharmaceuticals has hiked the price up 220% since 2008 and some analysts expect another 70% boost by 2014.
Pain. 2011 May;152(5):1007-17. Epub 2011 Mar 11.Sodium oxybate reduces pain, fatigue, and sleep disturbance and improves functionality in fibromyalgia: results from a 14-week, randomized, double-blind, placebo-controlled study.Russell IJ, Holman AJ, Swick TJ, Alvarez-Horine S, Wang YG, Guinta D; Sodium Oxybate 06-008 FM Study Group.
Pain Pract. 2010 Jan-Feb;10(1):54-9.Treatment of the narcoleptiform sleep disorder in chronic fatigue syndrome and fibromyalgia with sodium oxybate. Spitzer AR, Broadman M.
Arthritis Rheum. 2009 Jan;60(1):299-309. Sodium oxybate relieves pain and improves function in fibromyalgia syndrome: a randomized, double-blind, placebo-controlled, multicenter clinical trial. Russell IJ, Perkins AT, Michalek JE; Oxybate SXB-26 Fibromyalgia Syndrome Study Group.
Scharf MB, Baumann M, Berkowitz DV, J Rheumatol. 2003 May;30(5):1070-4. The effects of sodium oxybate on clinical symptoms and sleep patterns in patients with fibromyalgia.
Jacob Teitelbaum, MD., 2007. From Fatigued To Fantastic 3rd. ed., Avery Publishing.’
Sodium oxybate [Xyrem] for the treatment of Fibromyalgia – Source: Expert Opinion on Pharmacotherapy, Jun 16, 2011. ProHealth.com by Roland Staud
Wikipedia: Xyrem
TREATMENT DATABASEhttps://ammes.org/treatment/xyrem
Xyrem (sodium oxybate), also known as the “date rape drug,” is a central nervous system depressant. Chemically, Xyrem is the equivalent of gamma hydroxobutyric acid (GHB), a naturally occurring substance found in the central nervous system. Xyrem's use for medical purposes is highly restricted. The only approved use of Xyrem is for narcolepsy, a rare condition in which people suddenly fall asleep during the day. In 2010 the makers of Xyrem, Jazz Pharmaceuticals, submitted a New Drug Approval to the FDA for fibromyalgia. Approval was denied. Xyrem is currently listed as an “orphan drug” (a drug used for rare conditions).
USES IN ME/CFS: Xyrem has sometimes been used for treating the intractable insomnia experienced by many patients. Because of its potential for illegal use, physicians and patients who wish to use Xyrem must be registered with Jazz Pharmaceuticals. Registration includes a precise set of instructions for how to take Xyrem. These include not getting up after ingestion and using the bathroom before ingestion. Side effects include nausea, dizziness, headache, vomiting, sleepiness, and bed-wetting (for those who did not use the bathroom first
Prescription Treatments for ME/CFS https://livingwithchronicfatiguesyndrome.wordpress.com/2016/10/15/treatments-for-mecfs
It seems you are missing the most effective medication for CFS and Fibromyalgia which I believe is Xyrem. I’m sure it’s because 95% of us will have it denied by our insurance company because it’s so expensive because it’s not approved for our diagnosis. Without this medication I’m totally bedridden. My pain has improved by 95% and fatigue by about 60%. I still can’t work full time but I’m not housebound or bedridden. I worry every month that it will be taken away because my wonderful life that I have again would change for the worse again. I can’t wait until 2023 when it will be generic!
Shanee
How did you get it approved? I thought it was only indicated for Narcolepsy. Can you tell me anymore about your experience. How’s your sleep?
andrejuthe
Dear Hope, Xyrem is a name for GHB which is a precursor for among other things, GABA (gamma-butyric Acid) and you can buy GABA without problem. Now, GABA has low bioavalability but you kan make it into liposomes and take it nasally. Try it an compare it with the effect of Xyrem. Perhaps you can get the same effect with GABA
![]()
Treatment of the narcoleptiform sleep disorder in chronic fatigue syndrome and fibromyalgia with sodium oxybate https://pubmed.ncbi.nlm.nih.gov/20629967
This study investigates the response of the underlying sleep disorder associated with Chronic Fatigue Syndrome (CFS) and fibromyalgia (FM) to treatment. We retrospectively reviewed 118 cases clinically consistent with CFS or FM, treated in a neurology practice. Abnormal findings on sleep studies and associated human leukocyte antigen markers, and a clinical pattern suggestive of narcolepsy, are present in a high proportion of patients. When considered appropriate based on the clinical picture and test results, treatment with sodium oxybate was offered to these patients. Sixty percent of patients treated with oxybate experienced significant relief of pain, while 75% experienced significant relief of fatigue. We postulate that the response to oxybate in CFS and FM suggests a disturbance of sleep similar to narcolepsy. These findings support this novel approach to intervention and further research. The inability to distinguish CFS and FM by testing and response to treatment suggests that they may represent variations of the same disorder or may be closely related disorders
Xyrem (Sodium Oxybate) for Fibromyalgia https://www.verywellhealth.com/jzp-6-sodium-oxybate-716074
Clinical trials on FMS have consistently shown that the drug can significantly improve sleep quality and reduce pain. A 2013 study (Spaeth) concluded that it had a good long-term safety profile as well.
A 2010 study (Spitzer) suggested it may be effective in ME/CFS as well, but this was the first study of this drug for ME/CFS
Treatment with Flumazenil (GABAA receptor antagonist)
Treatment with Flumazenil (GABAA receptor antagonist) (click to open) An antidote for hypersomnia | Emory University | Atlanta, GA](http://news.emory.edu/stories/2012/11/antidote_for_hypersomnia/) Researchers at Emory University School of Medicine have discovered that dozens of adults with an elevated need for sleep have a substance in their cerebrospinal fluid that acts like a sleeping pill. The results are published in the journal [Science Translational Medicine](http://stm.sciencemag.org/content/4/161/161ra151 "science translational medicine hypersomnia"). Some members of this patient population appear to have a distinct, disabling sleep disorder called "primary hypersomnia," which is separate from better-known conditions such as sleep apnea or narcolepsy. They regularly sleep more than 70 hours per week and have difficulties awakening. When awake, they still have reaction times comparable to someone who has been awake all night. Their sleepiness often interferes with work or school attendance, and conventional treatments such as stimulants bring little relief. "These individuals report feeling as if they’re walking around in a fog — physically, but not mentally awake," says lead author David Rye, professor of neurology at Emory University School of Medicine and director of research for Emory Healthcare’s Program in Sleep. "When encountering excessive sleepiness in a patient, we typically think it’s caused by an impairment in the brain’s wake systems and treat it with stimulant medications. However, in these patients, the situation is more akin to attempting to drive a car with the parking brake engaged. Our thinking needs to shift from pushing the accelerator harder, to releasing the brake." In a clinical study with seven patients who remained sleepy despite above-ordinary sleep amounts and treatment with stimulants, Emory researchers showed that treatment with the drug flumazenil can restore alertness, although flumazenil’s effectiveness was not uniform for all seven. Alertness was gauged through the psychomotor vigilance test, a measurement of reaction time. Flumazenil is usually used in cases of overdose of benzodiazepines, a widely used class of sedatives such as diazepam (Valium) and zolpidem (Ambien). Evidence in the paper suggests that the sleep-inducing substance in patients’ cerebrospinal fluid is not a benzodiazepine drug, even though flumazenil counteracts it. Identifying the mysterious "somnogen", which appears to be produced by the body, could give scientists greater insight into how our brains regulate states of consciousness such as alertness and sleep. "Primary hypersomnias are disabling and poorly understood. This study represents a breakthrough in determining a cause for these disorders and devising a rational approach to therapy. Further research is required to determine whether or not the results apply to the majority of patients," says Merrill Mitler, a program director at the National Institute of Neurological Disorders and Stroke, part of the National Institutes of Health. The team of researchers involved in this effort includes Rye, Andrew Jenkins, assistant professor of anesthesiology, and Kathy Parker, previously at Emory and now at University of Rochester Medical Center. The paper describes how samples of patients’ cerebrospinal fluid (CSF) contain a substance that enhances the effects of the brain chemical GABA (gamma-amino butyric acid). GABA is one of the main inhibitory chemicals of the nervous system — alcohol, barbituates and benzodiazepines all enhance the effects of GABA. In the laboratory, the size of the effect on GABA receptor function is more than twice as large in the hyper-sleepy patients, on average, than in control samples. "In some of the more severely affected patients, we estimated the magnitude of the GABA-enhancing effect as nearly equivalent to that expected for someone receiving sedation for outpatient colonoscopy," Rye says. "This is a level of impaired consciousness that many subjects had to combat on almost a daily basis in order to live their usual lives." The ICSD-2 (International Classification of Sleep Disorders) terms this disorder "primary hypersomnia" and the proposed DSM-V describes it as "major hypersomnolence disorder." Its prevalence is unclear. The Emory team’s findings could potentially provide a biological definition and a treatment for an under-recognized sleep disorder. The patients in the group examined in the paper have received a variety of diagnoses, including idiopathic hypersomnia and narcolepsy without cataplexy. Cataplexy is a sudden loss of muscle tone, sometimes triggered by surprise or strong emotion, characteristic to narcolepsy. Other members of the group are simply considered "long sleepers" (more than 10 hours per day). In addition, the identity of the GABA-enhancing substance is not yet known, although Rye and Jenkins are devising strategies to pin it down. Based on its size and sensitivity to certain enzymes, it could be a peptide, similar to but not the same as the hormones oxytocin or hypocretin. In the laboratory, Jenkins and his colleagues have shown that the sleep-inducing substance can act on GABA receptors that are not sensitive to benzodiazepines. "Previous studies with flumazenil indicate that it does not have a wake-promoting effect on most people, so its ability to normalize vigilance in this subpopulation of extremely sleepy patients appears genuinely novel," Rye says. Other Emory authors include postdoctoral fellows Amanda Freeman and Jacqueline Fairley, data analyst Prabhjyot Saini, Donald Bliwise, professor of neurology, Michael Owens, professor of psychiatry and behavioral sciences, Lynn Marie Trotti, assistant professor of neurology, James Ritchie, professor of pathology and laboratory medicine and Paul Garcia, assistant professor of anesthesiology. Parker, Rye and Jenkins are co-inventors on patent rights held by Emory University. Emory and the inventors could potentially receive royalties derived from the intellectual property related to this research. The research was supported by the Woodruff Health Sciences Center Fund, the National Institute of Neurological Disorders and Stroke (NS055015 and NS050595) and the National Institute of General Medical Sciences (GM073959), James Sumner and the Arthur Williams Jr. Foundation. Reference:D.B. Rye, D.L. Bliwise, K. Parker, L.M. Trotti, P. Saini, J. Fairley, A. Freeman, P.S. Garcia, M.J. Owens, J.C. Ritchie and A. Jenkins. Modulation of vigilance in the primary hypersomnias by endogenous enhancement of GABA(A) receptors. *Science Trans. Med* 4, 161ra151 (2012). |||How flumazenil's effects were discovered{nl}An Atlanta woman came to Emory’s sleep center in 2005. Her sleep requirements – up to 16 hours per day -- gradually increased so much that she needed to take leave of absence from her job. Stimulants (modafinil and amphetamines) prescribed by doctors had a temporary benefit. However, tolerance to these medications required increasing doses that made her uncomfortable, elevated her blood pressure and produced rebound sleepiness, such that she’d sleep for 30 or even 57 hours continuously.{nl}Analysis of her CSF revealed biological activity that enhances the effects of GABA. In the laboratory, her CSF’s GABA-enhancing effects were reversible with flumazenil.{nl}Based on these results, the Emory team reasoned that flumazenil could form a treatment for the Atlanta woman. She found that it made her feel awake for the first time in years, and long-term treatment with flumazenil has allowed her to return to work.{nl}Flumazenil is normally delivered intravenously. Working with manufacturer Roche, Emory investigators, led by Parker, obtained permission from the FDA for long-term sublingual delivery of flumazenil for the Atlanta woman.{nl}This success drove Rye and his colleagues to examine CSF samples from other sleep clinic patients, and then to study flumazenil’s effects in a small group of patients with similar symptoms.{nl}{nl}From: The sleep switch: hypothalamic control of sleep and wakefulness{nl}Clifford B. Saper, Thomas C. Chou and Thomas E. Scammell| More than 70 years ago, von Economo predicted a wake-promoting area in the posterior hypothalamus and a sleep-promoting region in the preoptic area. Recent studies have dramatically confirmed these predictions. The ventrolateral preoptic nucleus contains GABAergic and galaninergic neurons that are active during sleep and are necessary for normal sleep. The posterior lateral hypothalamus contains orexin/hypocretin neurons that are crucial for maintaining normal wakefulness. A model is proposed in which wake\- and sleep-promoting neurons inhibit each other, which results in stable wakefulness and sleep. Disruption of wake\- or sleep-promoting pathways results in behavioral state instability. During World War I, the world was swept by a pandemic of encephalitis lethargica, a presumed viral infection of the brain that caused a profound and prolonged state of sleepiness in most individuals. The victims could be awakened briefly with sufficient stimulation, but tended to sleep most of the time. A Viennese neurologist, Baron Constantin von Economo, reported that this state of prolonged sleepiness was due to injury to the posterior hypothalamus and rostral midbrain1. He also recognized that one group of individuals infected during the same epidemic instead had the opposite problem: a prolonged state of insomnia that occurred with lesions of the preoptic area and basal forebrain. von Economo further hypothesized that lesions of the posterior diencephalon could cause the disease we now call narcolepsy, in which individuals have a tendency to fall asleep at inappropriate times. Based on his observations, von Economo predicted that the region of the hypothalamus near the optic chiasm contains sleep-promoting neurons, whereas the posterior hypothalamus contains neurons that promote wakefulness. In subsequent years, his observations on the sleep producing effects of posterior lateral hypothalamic injuries were reproduced by lesions in the brains of monkeys2, rats3 and cats4; and the insomnia producing effects of lateral preoptic–basal forebrain injuries were demonstrated in rats3 and cats5. Injections of the GABA-receptor agonist muscimol into these areas in cats produced results similar to that of the lesions, suggesting that wakefulness is promoted by neurons in the posterior lateral hypothalamus and sleep by neurons in the preoptic area6. However, the basic neuronal circuitry that causes wakefulness was only clearly defined in the 1980s and early 1990s, and the pathways responsible for the hypothalamic regulation of sleep began to emerge only in the past five years. This article focuses on these hypothalamic switching mechanisms. Other recent publications are available that discuss the homeostatic and circadian control of sleep7, the contributions of brainstem cholinergic–monoaminergic interactions to rapid eye movement (REM)–non-REM (NREM) sleep oscillations8^–10^, and the role of the dopaminergic system in sleep regulation11. Our model of the hypothalamic switching circuitry provides an effector mechanism by which many of these other systems produce or prevent sleep. The cholinergic and monoaminergic substrates of arousal In the years after World War II, Moruzzi, Magoun and many others contributed to identifying an ascending pathway that regulates the level of forebrain wakefulness12. Transection of the brainstem at the midpons or below did not reduce arousal, whereas slightly more rostral transections at a midcollicular level caused an acute loss of wakefulness. The wakepromoting outflow from this crucial slab of tissue at the rostral pontine–caudal midbrain interface was traced by anatomical and physiological techniques through the paramedian midbrain reticular formation to the diencephalon, where it divided into two branches. One pathway innervated the thalamus, and the second extended into the hypothalamus. Although this arousal system was termed the ascending reticular activating system, in fact its origins were identified only recently by the availability of modern neuroanatomical tracer methods combined with immunohistochemistry (Fig. 1). The main origin of the thalamic projection from the caudal midbrain and rostral pons was identified as the cholinergic pedunculopontine and laterodorsal tegmental nuclei (PPT–LDT)^13–15^. This population of cholinergic neurons projects in a topographic fashion to the thalamus, including the intralaminar nuclei16^–18^, but also to the thalamic relay nuclei and the reticular nucleus of the thalamus. The reticular nucleus is thought to play a key role in regulating thalamic activity, and the cholinergic influence is thought to be crucial in activating thalamocortical transmission19. Fig . 1. The ascending arousal system sends projections from the brainstem and posterior hypothalamus throughout the forebrain. Neurons of the laterodorsal tegmental nuclei and pedunculopontine tegmental nuclei (LDT and PPT) (blue circles) send cholinergic fibers (Ach) to many forebrain targets, including the thalamus, which then regulate cortical activity. Aminergic nuclei (green circles) diffusely project throughout much of the forebrain, regulating the activity of cortical and hypothalamic targets directly. Neurons of the tuberomammillary nucleus (TMN) contain histamine (HIS T), neurons of the raphé nuclei contain 5-HT and neurons of the locus coeruleus (LC) contain noradrenaline (NA). S leep-promoting neurons of the ventrolateral preoptic nucleus (VLPO, red circle) contain GABA and galanin (Gal). The activity of the PPT–LDT neurons varies with different behavioral states. During wakefulness, when the cortical electroencephalogram (EEG) shows low-voltage fast activity, many PPT–LDT neurons fire rapidly (Table 1). As the individual goes to sleep, the EEG waves become slower and larger; during this period, few PPT–LDT neurons are active. Periodically during the night, the individual enters a very different state of active sleep, in which there are rapid eye movements (REM sleep), a loss of muscle tone, except for the muscles involved in respiration, and a low-voltage fast EEG, which resembles a waking state. The PPT–LDT are released from tonic monoamine-mediated inhibition and hence fire rapidly during REM sleep8^–10,20^. If the thalamocortical system is activated in both wakefulness and REM sleep, what is the difference between these two states? One key distinction is the activity in the hypothalamic branch of the ascending arousal system (Fig. 1). Cell groups in the caudal midbrain and rostral pons that contribute to this projection include the noradrenergic locus coeruleus and the serotoninergic dorsal and median raphé nuclei, as well as the parabrachial nucleus21. Their axons run through the lateral hypothalamus, where they are joined by histaminergic projections from the tuberomammillary nucleus (TMN). Other neurons in the lateral hypothalamic area, some of which contain the peptide neurotransmitters orexin (also known as hypocretin)^22 ^or melanin-concentrating hormone23, join this projection, as do axons from the basal forebrain cholinergic nuclei (Fig. 1). Each of these pathways projects diffusely to the cortex of the entire cerebral hemisphere. |||EEG Fast, low voltage Slow, high voltage Fast, low voltage{nl}Eye movement Vision related Slow, infrequent Rapid{nl}Muscle tone ↑↑ ↑ 0{nl}LDT/PPT ↑ 0 ↑↑{nl}LC/DR/TMN ↑↑ ↑ 0{nl}VLPO cluster 0 ↑↑ ↑? VLPO extended 0 ↑? ↑↑{nl}Orexin/hyprocretin ↑↑ 0? 0?{nl}^aFiring rates are as follows: two arrows = rapid firing, one arrow = slower firing, 0 = little or no firing. Question marks represent hypothesized firing patterns for which there is as yet no firm evidence. Abbreviations: DR, dorsal raphé nucleus; EEG, electroencephalogram; LC, locus coeruleus; LDT, laterodorsal tegmental nuclei; NREM, nonrapid eye movement; PPT,{nl}pedunculopontine tegmental nuclei; REM, rapid eye movement; TMN, tuberomammillary nucleus; VLPO, ventrolateral preoptic nucleus.| The neurons in the monoaminergic cell groups have been closely studied for their relationship to behavioral state. Neurons in the locus coeruleus, the dorsal raphé nucleus and the TMN all fire at relatively characteristic rates, which are state dependent24^–27^. All three groups fire fastest during wakefulness, slow down with the EEG during NREM sleep, and nearly stop firing during REM sleep. Hence, the differences in the firing of the cholinergic and monoaminergic ascending arousal systems characterize and probably regulate the production of the different behavioral states (Table 1). ## The ‘off’ switch Because the firing of monoaminergic neurons is state dependent, understanding the sources of inputs to these cell groups provides a window into the mechanisms that regulate wakefulness. Sherin and colleagues have found two major inputs to the TMN core: (1) a population of diffusely distributed neurons in the lateral hypothalamic area; and (2) a dense cluster of neurons in the ventrolateral preoptic nucleus (VLPO cluster), surrounded medially and dorsally by a more diffuse extension from the nucleus (extended VLPO)^28,29^. Injections of an anterograde tracer have confirmed that the axons from the VLPO intensely innervate the cell bodies and proximal dendrites of the TMN, as well as less intensely innervating the dorsal and median raphé nuclei and the locus coeruleus29^,30^ (Fig. 2). The axons from the VLPO also terminate within the cholinergic basal forebrain and PPT–LDT groups, but do not appear to contact the cholinergic cell bodies. Nearly 80% of the retrogradely labeled VLPO neurons contain both the GABA-synthesizing enzyme glutamic acid decarboxylase and the peptide galanin29. Electron microscopy confirmed that the VLPO terminals onto TMN neurons were immunoreactive for GABA and make symmetric synapses29. Because galanin and animals were sleep deprived for 9 or 12 hours, to dissociate Fos expression from the circadian cycle. These animals showed the same correlation of Fos expression in the VLPO and sleep. However, the animals that failed to fall asleep following deprivation showed little or no Fos expression in the VLPO. Similar results have since been obtained in mice, cats, degus and Nile river rats (S. Gans *et al.,*unpublished)^36,37^. Electrophysiological recordings have similarly identified sleep-active neurons in the VLPO region38^,39^. The rate of firing of VLPO neurons was nearly doubled during sleep compared with waking, and it doubled again during the deep sleep that followed sleep deprivation. The firing rate of VLPO neurons was not increased after sleep deprivation until the animals actually slept, so VLPO firing rates probably are not related to the degree of sleepiness, but instead the production of sleep itself. The chemical identity of the sleep-active VLPO neurons has recently been determined by combining *in situ*hybridization for galanin with immunocytochemistry for Fos (S. Gaus *et al.*and J. Lu *et al.*, unpublished). In sleeping rats, 80% of the Fos-immunoreactive neurons in the VLPO cluster (and 50% in the extended VLPO) also contained galanin mRNA, and about half of the galanin mRNAcontaining neurons in both parts of the nucleus had a Fos-immunoreactive nucleus. Galanin-positive neurons of the VLPO were also sleep active in mice and cats (S. Gaus *et al.*, unpublished)^40. A galanincontaining cell group in the VLPO has also been identified in monkeys and humans (S. Gaus *et al.*, unpublished), so this system appears to be a uniform feature of mammalian brains. Is the VLPO necessary for sleep? To determine whether the VLPO neurons are necessary for producing sleep, Lu and colleagues produced small excitotoxic lesions in the lateral preoptic area by microinjecting ibotenic acid41. Although previous studies have demonstrated insomnia after injury to this region, these lesions injured fiber pathways3^,5^ ^or involved much of the preoptic area beyond the VLPO (Refs 42,43). In order to analyze the lesions, the numbers of remaining Fos-immunoreactive cell bodies in the VLPO cluster and the extended VLPO were compared with the changes in sleep behavior. In animals with more than 70% bilateral cell loss in the VLPO cluster, the amounts of both NREM and REM sleep two possible stable patterns of firing and a tendency to avoid intermediate states. Such properties would be very useful in sleep–wake regulation, as an animal that walked about while half asleep would be in considerable danger. GABA are known to inhibit both TMN and neurons of the locus coeruleus24^,31–33^, the descending projection from the VLPO is likely to be inhibitory in nature29^,34,35^. To determine the relationship between VLPO activity and sleep–wake behavior, the expression of Fos protein immunoreactivity was examined, as a marker of neuronal activity in the VLPO across the wake–sleep cycle28. The number of Fos-immunoreactive neurons in the VLPO correlated closely with the amount of sleep the animals experienced during the hour before death. Other were reduced by about 55% (Ref. 41). The loss of neurons in the VLPO cluster correlated closely with the loss of NREM (*r*=0.77), but did not correlate significantly with loss of REM sleep. However, the loss of Fos-immunoreactive neurons in the extended VLPO correlated closely with the loss of REM sleep (*r*=0.74), but did not show a significant correlation with the loss of NREM sleep. Conversely, when rats were exposed to a period of darkness during the day, a condition that doubles REM sleep time, there was a concomitant increase in Fos expression in the extended VLPO, but not the VLPO cluster (J. Lu *et al.*, unpublished). Anatomical studies have shown that the projections to the locus coeruleus, dorsal–median raphé, and the PPT–LDT arise predominantly from the extended VLPO, rather than the VLPO cluster (J. Lu *et al.*, unpublished)^30,44^. These observations suggest that the VLPO contains specific subregions that are specialized for the control of REM versus NREM sleep. ## The flip–flop and bistability The relationship between the VLPO and the major monoamine groups appears to be reciprocal. The VLPO is innervated by histaminergic axons from the TMN, noradrenergic terminals from the locus coeruleus and serotoninergic inputs from the midbrain raphé nuclei45. Recordings from individual VLPO neurons in hypothalamic slices show that they are inhibited by noradrenaline and by 5-HT (Ref. 46). No responses to histamine were recorded, but TMN neurons also contain GABA and galanin, which might inhibit the VLPO (Ref. 47). The model shown in Fig. 3 is based on the hypothesized mutual inhibition between the VLPO and the major arousal systems. Although the monoamine systems are emphasized, there might be other components of the arousal system that are not illustrated here, such as neurons in the lateral hypothalamic area, that would interact with the VLPO in a similar way. When VLPO neurons fire rapidly during sleep, they would inhibit the monoaminergic cell groups, thus disinhibiting and reinforcing their own firing. Similarly, when monoamine neurons fire at a high rate during wakefulness, they would inhibit the VLPO, thereby disinhibiting their own firing. This reciprocal relationship is similar to a type of circuit that electrical engineers call a ‘flip–flop’48. The two halves of a flip–flop circuit, by each strongly inhibiting the other, create a feedback loop that is bistable, with Fig . 2 . The projections from the ventrolateral preoptic nucleus (VLPO) to the main components of the ascending arousal system. Axons from the VLPO directly innervate the cell bodies and proximal dendrites of neurons in the major monoamine arousal groups. Within the major cholinergic groups, axons from the VLPO mainly innervate interneurons, rather than the principal cholinergic cells. Abbreviations: LC, locus coeruleus; LDT, laterodorsal tegmental nuclei; PPT, pedunculopontine tegmental nuclei; TMN, tuberomammillary nucleus; VLPO, ventrolateral preoptic nucleus. The blue circle indicates neurons of the LDT and PPT; green circles indicate aminergic nuclei; and the red circle indicates the VLPO. The self-reinforcing firing patterns of the flip–flop switch produce a degree of resistance to switching when one side is firing briskly. This stability avoids inappropriate changes in wake–sleep state when input signals to the VLPO and the monoaminergic cell groups fluctuate transiently over the course of the day. However, large scale influences, such as circadian sleep drive or accumulated homeostatic need for sleep might gradually shift the relative balance of mutual inhibition. When this pressure to change becomes great enough, the same feedback properties that allow the flip–flop circuit to resist change will suddenly give way and rapidly produce a reversal of firing patterns. The flip–flop switch therefore changes behavioral state infrequently but rapidly, in contrast to the homeostatic and circadian inputs, which change continuously and slowly. A crucial aspect of this bistable switch is that if the firing of neurons on either side is substantially weakened, the switch is less stable. For example, after lesions of the VLPO, the animals experience much more wakefulness, and the homeostatic drive for sleep might increase, forcing the balance in the circuit nearer to its transition point41. Thus, rats with VLPO lesions fall asleep more frequently, but because the self-reinforcing properties of the circuit are weaker, they switch back into wakefulness more frequently as well, with the result that both wake and sleep bouts are shorter after VLPO lesions. Fig . 3 . A model for reciprocal interactions between sleep\- and wakepromoting brain regions, which produces a flip–flop switch. Inhibitory pathways are shown in red, and the excitatory pathways in green. The blue circle indicates neurons of the LDT and PPT; green boxes indicate aminergic nuclei; and the red box indicates the VLPO. Aminergic regions such as the TMN, LC and DR promote wakefulness by direct excitatory effects on the cortex and by inhibition of sleep-promoting neurons of the VLPO. During sleep, the VLPO inhibits amine-mediated arousal regions through GABAergic and galaninergic (GAL) projections. Most innervation of the TMN originates in the VLPO core, and input to the LC and DR predominantly comes from the extended VLPO. This inhibition of the amine-mediated arousal system disinhibits VLPO neurons, further stabilizing the production of sleep. The PPT and LDT also contain REM-promoting cholinergic neurons. The extended VLPO (eVLPO) might promote REM sleep by disinhibiting the PPT–LDT; its axons innervate interneurons within the PPT–LDT, as well as aminergic neurons that normally inhibit REM-promoting cells in the PPT–LDT. Orexin/hypocretin neurons (ORX ) in the lateral hypothalamic area (LHA) might further stabilize behavioral state by increasing the activity of aminergic neurons, thus maintaining consistent inhibition of sleep-promoting neurons in the VLPO and REM-promoting neurons in the PPT–LDT. Unbroken lines represent neuronal pathways described in the text. Broken black lines indicate influences of specific regions on behavioral states. Abbreviations: DR, dorsal raphé nucleus; HIS T, histamine; LC, locus coeruleus; LDT, laterodorsal tegmental nuclei; PPT, pedunculopontine tegmental nuclei; REM, rapid eye movement; TMN, tuberomammillary nucleus; VLPO, ventrolateral preoptic nucleus. ## S tabilizing the flip–flop A similar deficit on the waking side of the mutually inhibitory flip–flop circuit might produce abrupt and unstable fluctuations in behavioral state in the disorder known as narcolepsy. Individuals with narcolepsy experience frequent and unwanted transitions into sleep during wakefulness, and they tend to awaken more frequently from sleep as well. When placed in a quiet environment, they fall asleep and transition into REM sleep far more rapidly than unaffected individuals. At times, they experience fragments of REM sleep intermixed with wakefulness, such as loss of muscle tone while awake, a condition known as cataplexy. The origin of narcolepsy was not understood until a dramatic series of events that unfolded during the past three years. In 1998, two groups of investigators simultaneously discovered a family of peptide neurotransmitters that was made by neurons in the lateral hypothalamus. Sakurai and co-workers identified two peptides in a screen for ligands for orphan G-protein-coupled receptors, which they named ‘orexin A and B’, because the peptides appeared to promote feeding49. de Lecea *et al.*, meanwhile, described two hypothalamic-specific mRNAs coding for the same peptides, which they termed ‘hypocretins’because they were hypothalamic peptides with sequence similarity to secretin50. However, when the full extent of the pathways containing the orexin/hypocretin peptides was revealed by immunocytochemistry51^–53^, it became clear that the orexin/hypocretin neurons, like the VLPO, innervated all of the components of the ascending arousal system (Fig. 4). Orexin 1 receptors were found in the locus coeruleus, orexin 2 receptors in the TMN and basal forebrain, and both types of receptors were found in the midbrain raphé nuclei and mesopontine reticular formation54^,55^. Because both receptors are mainly excitatory, these observations suggested that orexin/hypocretin might help maintain wakefulness by increasing the activity of the ascending arousal system. In 1999, Chemelli *et al.*produced orexin/hypocretin knockout mice53. These animals suffered intermittent attacks during the active (dark) period, in which they would suddenly fall onto their sides for a few minutes, then get up and resume their activities. Polysomnographic analysis showed that these periods of behavioral arrest consisted of episodes of atonia associated with an EEG that was consistent either with wakefulness (i.e. cataplexy) or REM sleep, findings that are suggestive of narcolepsy. Simultaneously, Nishino *et al.*found that canine narcolepsy was due to mutations in the gene for the type 2 orexin/hypocretin receptor56. The combination of these two findings provide overwhelming evidence that the loss of orexin/hypocretin signaling via the type 2 receptor is sufficient to produce the symptoms of narcolepsy. The absence of orexin in the hypothalamus and in the spinal fluid of humans with narcolepsy has subsequently been confirmed57^–59^. The orexin/hypocretin neurons probably play an important role in producing normal wakefulness. Kilduff and Peyron have hypothesized that these neurons might be active during wakefulness and REM sleep60, but we predict that these cells are predominantly wake active. Orexin neurons synthesize Fos protein during wakefulness, and the number of Fos-positive orexin-containing neurons correlates closely with the amount of wakefulness, whether it is naturally occurring, produced by sleep deprivation or caused by stimulant drugs, such as amphetamine or modafinil53^,61^. Extracellular recordings from neurons in the perifornical region, which contains the orexin/hypocretin cell bodies, confirm that cells in this area are predominantly wake active although some also fire during REM sleep (R. Szymusiak, unpublished). However, neither orexin-deficient animals nor narcoleptic humans have excessive amounts of sleep, but instead they have poor maintenance of both wakefulness and sleep, or dysfunctional switching. What, then, can be the role of the orexin/hypocretin neurons in maintaining behavioral state? Recent studies have shown that the orexin/hypocretin neurons might influence both sides of the flip–flop circuit by direct projections to both the monoaminergic and cholinergic arousal cell groups, and to the VLPO region. Orexin/hypocretin increases the firing of neurons in the locus coeruleus62, the dorsal raphé nucleus63 and the TMN (H. Hass, unpublished). Although VLPO neurons do not appear to contain orexin/hypocretin receptors53, injection of orexin/hypocretin into the preoptic area near the VLPO increases wakefulness and decreases both REM and NREM sleep64, suggesting a presynaptic mechanism of action (perhaps on monoaminergic axons). Orexin/hypocretin neurons therefore might act as a ‘finger’, pressing the flip–flop switch into the ‘wakeful’position, and preventing inappropriate switching into the ‘sleep’position. In the absence of such an influence, as seen in narcolepsy, the switch would be less stable, and more susceptible to sudden and inappropriate transitions. This model could also explain the rapid transitions into REM sleep, or fragments of REM sleep, that are seen in narcoleptics. The TMN, raphé nuclei and locus coeruleus contain orexin/hypocretin receptors54, and all three groups inhibit REM sleep10. In the absence of an excitatory orexin input, the weakened arousal influence and increased activity of the extended VLPO would allow earlier and more frequent transitions to the REM state. Interestingly, like the animals with VLPO lesions, destabilizing the switch in narcolepsy also results in more frequent awakenings from sleep. ## Concluding remarks Advances over the past five years have largely borne out the remarkable predictions of von Economo, which were made over 70 years ago on the basis of clinical observations. The occurrence of insomnia in individuals with lesions of the preoptic area and basal forebrain was almost certainly due to the involvement of the VLPO in these cases. The hypersomnolent individuals clearly had lesions of the ascending arousal pathways at the midbrain–diencephalic junction. And von Economo’s prediction that narcolepsy could be caused by lesions of the posterior diencephalon has been proven true by the recognition that this region contains the orexin/hypocretin neurons, the loss of which causes narcolepsy in humans. The recent progress in defining the components of the sleep switching system should allow us to understand better how slowly changing influences, such as homeostatic and circadian drives, can produce rapid and discrete changes in behavioral state.
Most common drugs used for CFS
- Bromocriptine
- Cerebrolysin
- Citalopram
- Donepizil
- Erythropoietin
- ISRIB
- Memantadine
- Methylphenidate
- Milnacipran
- Neuropeptide
- Neurotrophic
- Pioglitazone
- Peptides
Suramin
Suramin (https://www.healthrising.org/blog/category/treatment/drugs/suramin/ "Suramin is anti-purinergic drug usually used to treat African sleeping sickness and river blindness. Dr. Naviauw believes Suranim may be able to turn off the "cell danger response" in ME/CFS and autism. A small Suramin autism trial was successful. ") (2)
- Most common Drugs used for CFS (and CFS cofactors continued
- Abilify (4);
- Ampligen (16);
- Amytriptyline (2
- Anti-inflammatory (1);
- Antivirals (17);
- Ativan (1);
- Baclofen (1);
- Clonidine (2);
- Cortene (5);
- Cymbalta (4);
- Dextromethorphan (7);
- Doxepin (1);
- Enbrel (1);
- Flexeril (4);
- Heparin (1);
- Hormones (thyroid, testosterone, progesterone, estrogen, hydrocortisone) (4);
- Hydrocortisone (Cortef) (1);
- Intranasal (1);
- Ivabradine (6);
- IVIG (11);
- Ketamine (7);
- Klonopin (3);
- Low Dose Naltrexone (26);
- Lyrica (11);
- Memantine (1);
- Mestinon (2);
- Metformin (2);
- Mifepristone (4);
- Nimodipine (4);
- Opioid drugs (15);
- Propanolol (3);
- Quetiapine (1);
- Rituximab (7);
- Savella (5);
- Stimulants (5);
- Suramin (2);
- Tomnya (2);
- Xifaxin (2);
- Xyrem (1);
![]()
Classes of Drugs
Several categories of drugs are used to treat ME/CFS. They include:
Antimicrobial drugs (includes antiviral, antibiotic)
Antidepressants (SSRIs/SNRIs and tricyclic)
Anxiety or anxiolytic agents
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Blood-pressure medications
Experimental treatments
Anti-fungal drugs: Fluconazole, Itraconazole
Other drug treatments: Chelation, Cyclophosphamide, Prednisone, Trazodone, Tramadol
B-cell depletion: Rituximab
Immunomodulators and immunostimulants: Ampligen, Low dose naltrexone, Intravenous immunoglobulin, Staphylococcal vaccine, Interferon
Antivirals: Valganciclovir, Famciclovir, Valaciclovir, Acyclovir
Anti-inflammatory drugs: Sulfasalazine
Full list https://bra.in/8jkAZp
Because all of these medications are used for off-label purposes (meaning they're not FDA approved specifically for ME/CFS), your insurance company may not cover them.
![]()
Antimicrobial
"Antimicrobial" refers to a variety of drug types, including antivirals, antibiotics, antifungals, and antiprotozoals. Researchers say this condition makes your body constantly act as if it's fighting an infection. While no specific virus or bacteria has been linked conclusively to ME/CFS, some research supports the possibility of the Epstein-Barr virus (which causes mononucleosis), human herpes virus 6 (HHV-6, which causes roseola) and enteroviruses.
Ampligen (rintatolimod)
This experimental drug was rejected by the FDA and is not yet on the market for any use. Ampligen works by jump-starting your body's natural anti-viral pathway and regulating levels of RNase L (a substance in your cells that attacks viruses), which can be high in people with ME/CFS. Studies show Ampligen is more effective and has far fewer side effects than other drugs in its class. Manufacturer Hemispherx Biopharma is continuing trials of other conditions, hoping to someday win approval.
Valcyte (valganciclovir)
The antiviral valganciclovir treats HHV-6, which multiple studies have found in a significant percentage of people with ME/CFS. Small studies have had encouraging results, but experts agree that larger and better-designed studies need to be done before they can draw reliable conclusions.
Because researchers haven't identified a particular infection that leads to this condition, doctors don't usually prescribe other antimicrobials for it, unless you have an active infection.
![]()
Antidepressants
Just because antidepressants are a common treatment, it doesn't mean all the people taking them are depressed or have any kind of psychological condition. (While many people with the condition are clinically depressed, it's generally considered a resultof the symptoms and change in lifestyle and not a cause of the illness itself.) The most common types of antidepressants prescribed are SSRI/SNRIs and tricyclic agents.
SSRI/SNRI-Type Antidepressants
The reason antidepressants work is because they raise levels of important neurotransmitters that are low in some people with ME/CFS. These drugs are called selective serotonin reuptake inhibitors (SSRIs) or serotonin-norepinephrine reuptake inhibitors (SNRIs or NSRIs).
Serotonin helps process pain signals and is also important to your sleep-wake cycle, while norepinephrine (a type of adrenaline) is involved in the stress response and bursts of energy.
Examples of SSRIs and SNRIs are:
- Cymbalta (duloxetine)
- Prozac (fluoxetine)
- Zoloft (sertraline)
- Paxil (paroxetine)
- Effexor (venlafaxine)
- Desyrel (trazodone)
- Wellbutrin (bupropion)
- Tricyclic Antidepressants
Low doses of tricyclic agents sometimes improve sleep and relieve mild, widespread pain in people with ME/CFS. Some examples are:
- Adapin, Sinequan (doxepin)
- Elavil, Etrafon, Libitrol, Triavil (amitriptyline)
- Norpramin (desipramine)
- Pamelor (nortriptyline)
Be sure you're familiar with the side effects of any antidepressants you're taking, especially since many antidepressants come with a warning of heightened risk of suicidal thoughts and behaviors. If you decide to stop taking any of these drugs, talk to your doctor about how to properly wean off of them. Stopping cold turkey can lead to some potentially serious problems.
![]()
Anxiety
Doctors sometimes prescribe anti-anxiety drugs for those ME/CFS patients with panic disorder. They include:
- Xanax (alprazolam)
- Klonopin (clonazepam)
- Ativan (lorazepam)
Common side effects of anxiety drugs include sedation, amnesia, insomnia, muscle cramps, and convulsions. Stopping them also can lead to withdrawal symptoms.
![]()
NSAIDS
These drugs sometimes are used to relieve the pain and fever associated with ME/CFS. Several are available over-the-counter, including:
- Advil, Bayer Select, Motrin Nuprin (ibuprofen)
- Aleve, Anaprox, Naprosyn (naproxen)
- Feldene (piroxicam)
Your doctor may also prescribe other types of NSAIDs, and it's important not to combine different drugs in this class. That can put you at greater risk of developing dangerous side effects, including kidney damage and gastrointestinal bleeding.
![]()
Blood Pressure
A form of low blood pressure called neurally mediated hypotension (NMH) is common in people with ME/CFS. It's caused by an abnormal interaction between the heart and the brain, even though both organs are normal and healthy. Also called the fainting reflex, NMH can cause dizziness and fainting and is sometimes diagnosed by what's called a tilt table test.
Some people with diagnosed NMH take a low-blood-pressure medication called Florinef (fludrocortisone), while others take the high blood-pressure medication Tenormin (atenolol). If you're on Tenormin, you'll probably need to be watched for low blood pressure and may be advised to increase your salt and water intake.
Source: 2013 Solve ME/CFS Initiative. All rights reserved. Treatment FYI
![]()
From: 'Medications for Chronic Fatigue Syndrome' https://www.drugs.com/condition/chronic-fatigue-syndrome-cfs.html
Modafinil
Lisdexamfetamine
Amantadine
Duloxetine
Armodafinil
SSRI's SNRI's
Ritalin
Aderal
Viagra
Nicotine
Zantec
Modafinil is used for: Improving wakefulness in patients with excessive sleepiness associated with narcolepsy or other sleep disorders. It may also be used for other conditions as determined by your doctor.
Modafinil is a wakefulness-promoting agent. Exactly how it works is not known, but it is thought to work by altering the natural chemicals (neurotransmitters) in the brain.
Lisdexamfetamine is used for:
Treating attention deficit hyperactivity disorder (ADHD). It is also used to treat binge eating disorder (BED). It may also be used for other conditions as determined by your doctor.
Lisdexamfetamine is an amphetamine. Exactly how lisdexamfetamine works is not known. It affects certain chemicals in the brain that may help improve attention span and behavior.
Amantadine is used for:
Preventing and treating certain types of flu. It is used to treat Parkinson disease and uncontrolled muscle movements caused by some medicines. It may also be used for other conditions as determined by your doctor.
Amantadine is an antiparkinson and antiviral agent. How amantadine works against the flu is not known. It may block reproduction of the virus and decrease the ability of the virus to get into the cells. How amantadine works against Parkinson disease is not known. It may increase a certain chemical in the brain.
Duloxetine delayed-release capsules are used for:
Treating depression and generalized anxiety disorder. It is used for managing pain caused by fibromyalgia and diabetic peripheral neuropathy (DPN). Duloxetine delayed-release capsules are used for managing chronic musculoskeletal pain, including osteoarthritis and chronic low back pain. It may also be used for other conditions as determined by your doctor.
Duloxetine delayed-release capsules are a serotonin-norepinephrine reuptake inhibitor (SNRI). It works by restoring the balance of certain natural substances in the brain (serotonin and norepinephrine), which helps to improve certain mood problems and manage pa.
Armodafinil is used for:
Improving wakefulness in patients with excessive sleepiness from sleep apnea, narcolepsy, or shift work disorder. It may also be used for other conditions as determined by your doctor.
Armodafinil is a wakefulness-promoting agent. Exactly how it works is not known. Armodafinil affects certain chemicals in the brain that may affect sleep.
From: 'Amitriptyline for Fibromyalgia & Chronic Fatigue Syndrome' https://www.verywell.com/amitriptyline-for-fibromyalgia-mecfs-715765
Amitriptyline is a popular antidepressant that's available only in generic form in the U.S. It used to be sold under the brand name Elavil.
Amitriptyline is classified as a tricyclic antidepressant. For years, some doctors have considered it a front-line treatment for fibromyalgia(https://www.verywell.com/what-is-fibromyalgia-716143) and chronic fatigue syndrome(https://www.verywell.com/what-is-chronic-fatigue-syndrome-716113)(ME/CFS(https://www.verywell.com/myalgic-encephalomyelitis-me-715663)). However, this came about more from trial-and-error use than clinical studies.
Amitriptyline and other tricyclic drugs are thought to increase the amount of the neurotransmitters serotonin and norepinephrine that your brain can use. They do this by slowing down a process called "reuptake," which is when specialized cells absorb used neurotransmitters so they can be re-used elsewhere.
Other antidepressants, called reuptake inhibitors, use different mechanisms to achieve a similar effect.
Serotonin and norepinephrine are believed to be dysregulated in both fibromyalgia and ME/CFS.
Amitriptyline has a long history of use for ME/CFS, again despite a lack of clinical studies and because of real-world observations of improvement. Very little research has been done.
A 2012 study, however, did look at amitriptyline for ME/CFS and found that it was the only one among several antidepressants tested that inhibited mast-cell release of pro-inflammatory cytokines(https://www.verywell.com/what-are-cytokines-189894), which are believed to play a role in ME/CFS.
Dosage
For adults, a typical amitriptyline dosage can range from 40 mg up to 150 mg per day. It's generally divided into multiple doses.
It can take as long as a month for you to notice changes due to this medication.
Be sure to follow your doctor's instructions for taking this medication. If you want to quit taking it, don't just stop suddenly. Ask your doctor about the proper way to wean off of this drug.
There are many less common drugs such as scopolamine zantac360and choline
click links.html
\*This list not complete yet (please see 5 Treatment Protocols(brain://api.thebrain.com/zBeZ4L6q6n0BlcEIzuFxfQ/TIo6LQiJGVyzi58kchHAJA/5TreatmentProtocols))
Listing of therapies, protocols, drugs and supplements (in order of average effectiveness as reported by takers of a 'curetogether' poll) http://curetogether.com/Chronic-Fatigue-Syndrome/treatments/ae/
Plus add items nopt listed from report
From: 'Treatments for ME/CFS' https://livingwithchronicfatiguesyndrome.wordpress.com/2016/10/15/treatments-for-mecfs
# Prescription Treatments for ME/CFS
Azithromycin(https://livingwithchronicfatiguesyndrome.wordpress.com/2012/05/09/may-2012-a-treatment-update/)– Azithromycin is an antibiotic that has antiviral and immunomodulatory properties. It may be effective against a broad range of bacteria, many of which have been linked to ME/CFS. A study found that 58 out of 99 ME/CFS patients had a decrease in symptoms while taking Azithromycin. Dr. De Meirleir and Dr. Nicholson are both advocates of this antibiotic and have used it on ME/CFS patients with some success.
Azithromycin is generally fairly low in side effects although sometimes causing stomach upset. It is normally taken 3 times a day (away from food) at a dosage of 500mg on each occasion.
Dr. Brewer’s Protocol(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/09/15/dr-brewers-protocol/)– This protocol involves patients taking either a nasal version of Amphotericin B or a compounded Nystatin that has to be atomised. Patients should also take a chelating PX. A pilot study by Dr. Brewer found that 56 out of 151 ME/CFS patients could not tolerate the Amphotericin B. 88 out of the remaining 94 patients (93.6%) had a reduction in symptoms. Approximately a third of these 88 CFS patients reached remission. Since this pilot study, Dr. Brewer has used a compounded and atomised Nystatin due to it being safer than the nasal Amphotericin B. The theory behind Dr. Brewer’s Protocol involves treating the sinus reservoirs of mycotoxins that may be causing ME/CFS symptoms.
Since replacing Amphotericin B with Nystatin, Dr. Brewer’s Protocol has become safer for patients, with followers of the protocol rarely reporting nasal side effects. Patients experiencing die-off symptoms range from 30-40% according to Dr. Brewer. The appropriate dosages of the compounded and atomised Nystatin and the chelating PX are provided by the compounding pharmacy.
Clonazepam(https://livingwithchronicfatiguesyndrome.wordpress.com/2012/09/13/september-2012-a-treatment-update/)– This treatment is one of the most polarising ME/CFS treatments in existence. Clonazepam may benefit patients due to reducing the overstimulation of the brain and central nervous system. It also has potential effects as a sleep aid, neuroprotector and energy enhancer. Several ME/CFS specialists are advocates of Clonazepam under the right circumstances, such as Dr. Cheney. There are also many online reports of patients benefiting from Clonazepam.
The dark-side of Clonazepam involves countless ME/CFS patients’ online anecdotes stating that this drug has been the worst treatment they have ever tried as it has caused long term side effects. A dosage around the 0.5mg\- 1mg range is normally used on ME/CFS patients for sleep which is a lower amount than for other conditions. An even tinier dose is recommended by Dr. Cheney if the drug is used during the day with the motive of increasing the patient’s energy. Clonazepam shouldn’t be stopped suddenly and patients should gradually reduce the dose before ceasing treatment. The common side effects of Clonazepam include drowsiness and confusion. Some ME/CFS patients have reported other side effects such as a general worsening of their condition. As Clonazepam usage can be habit forming, patients often feel like they need to increase the dose to maintain efficacy which can be a dangerous process.
Dexedrine(https://livingwithchronicfatiguesyndrome.wordpress.com/2012/05/09/may-2012-a-treatment-update/)– Dexedrine may benefit ME/CFS patients due to alleviating cognitive impairment, reducing fatigue and increasing energy. A small study found 9 out of 10 ME/CFS patients had reduced fatigue after taking Dexedrine in comparison to 4 out of 10 patients in the placebo group. Dr. Teitelbaum is a supporter of this treatment, believing that it increases energy and blood pressure. Dr. Goldstein has written that 1/3^rd of ME/CFS patients will improve as a result of taking stimulants and he has recommended amphetamine salts.
One of the risks of Dexedrine is that prolonged usage may lead to addiction. Dr. Goldstein has warned that if specific neurotransmitters are low in an ME/CFS patient, stimulants may increase ME/CFS symptoms. Dr. Rowe has recommended that ME/CFS patients begin with a 5mg dosage in the morning and if no improvement is noted, the dosage be increased to 10-15mg. Some patients may find that 5mg is too high for them to tolerate.
DHEA(https://livingwithchronicfatiguesyndrome.wordpress.com/2009/08/25/prescription-medications-that-i-have-taken-for-cfs/)– DHEA is a hormone produced by the adrenal glands. A study found that the majority of the Japanese ME/CFS subjects had DHEA deficiency. Several studies have found the use of oral DHEA and intravenous vitamin C to be useful in treating ME/CFS. Another study found normal DHEA levels in ME/CFS patients but low blood levels of a hormone that causes the adrenal glands to release DHEA.
Dr. Cheney has found that DHEA is more effective in less severe cases of ME/CFS and that sometime symptoms may worsen if severely ill patients take this treatment. Dr. Myhill recommends Pregnenolone as an alternative to DHEA. Some doctors have experienced success in prescribing lower doses of DHEA such as doses less than 10mg. Another ME/CFS specialist recommends 50mg every second day. Palpitations, hair loss, acne and an upset stomach are some possible side effects.
Fludrocortisone(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/07/27/fludrocortisone-for-cfs/)– Fludrocortisone is a synthetically produced hormone. It may benefit ME/CFS patients with; hypotension, POTS, orthostatic intolerance or adrenal insufficiency. Its mechanism of action in ME/CFS patients could be due to; increasing blood volume, raising blood pressure and helping blood reach the bodies extremities. Three studies have been performed on ME/CFS patients taking Fludrocortisone with the ME/CFS patients’ level of improvement no better than the placebo group. According to Dr. Bell, Fludrocortisone is more likely to work on younger patients who are still somewhat active. Dr. Bell tries this treatment on almost all of his patients and says that it works well in approximately 25% of cases. If the drug doesn’t increase the ME/CFS patients’ activity levels by at least 50%, he stops the drug. Dr. Cheney believes that liquorice can have the same effect on patients as Fludrocortisone.
Many ME/CFS specialist recommend that Fludrocortisone dosages start at a very low amount such as a quarter of a 0.1mg tablet. Dr Rowe begins patients on a quarter of a tablet and if no side effects are noted, gradually increased this amount every 4-7 days to maximum of 2 tablets (0.2mg). Potassium and plenty of water should be used concurrently with this treatment. High blood pressure and depression are two possible side effects.
Gabapentin (Neurontin)(https://livingwithchronicfatiguesyndrome.wordpress.com/2016/04/13/gabapentin-neurontin-for-me/)– Gabapentin is a anticonvulsant drug that may benefit ME/CFS patients due to reducing pain, increasing energy and improving sleep. Its mechanism of action may be its ability as a calcium channel blocker to reduce the excretion of certain neurotransmitters that cause pain and stimulate the brain. Anecdotally, a number of ME/CFS patients have gained extra energy as a result of taking Gabapentin however in some of these cases the extra energy has worn off. Dr. Goldstein lists Gabapentin amongst his five most favoured treatments for ME/CFS. Dr. Teitelbaum uses Gabapentin for its sleep effects and Dr. Enlander uses it for stopping the ‘abnormal impulses’ in ME/CFS patients’ brains. Three studies have found Gabapentin to be beneficial to Fibromyalgia patients in the areas of sleep enhancement and pain reduction.
Gabapentin is considered to be fairly safe with a Cochrane review finding that serious adverse effects were no more common in the Gabapentin group than the placebo group. Dizziness, somnolence, peripheral oedema and gait disturbance are the most common side effects. Dosages should begin at low levels and only be increased if tolerated. ME/CFS specialists tend to start patients at 100mg-800mg and if no side effects occur, the dose is gradually increased up to 2400mg-5000mg. These doses are the total daily dosages and should be split up into three dosages across the day.
Heparin (https://livingwithchronicfatiguesyndrome.wordpress.com/2016/08/23/heparin-for-me/)– Heparin is an anti-coagulant drug that may benefit ME/CFS patients who have hypercoagulation. A Heparin-ME/CFS study found all 9 patients gaining improvement with 5 noting significant improvement. Another paper refers to 60 ME/CFS/Fibromyalgia patients taking Heparin with an average improvement of 85%. Dr. Teitelbaum writes that Heparin helps about 50% of ME/CFS patients who haven’t benefited from any other treatment. It is imperative that ME/CFS patients have coagulation testing performed to determine Heparin suitability before commencing treatment.
Depending on what type of Heparin is used and what delivery method is chosen, the possible side effects of Heparin vary. If unfractionated Heparin is injected subcutaneously, regular blood tests to monitor treatment are a necessity. Heparin-induced thrombocytopenia is a potential side effect with this treatment although with Low Molecular Weight Heparin this is less likely to occur. A DEXA bone density test and liver and kidney function tests may be required before starting Heparin treatment. Sublingual Heparin and Low Molecular Weight Heparin are considered safer than unfractionated Heparin. Dr. Teitelbaum recommends those patients taking unfractionated Heparin start with 5000 unit injections twice a day and if blood tests are normal, the dose be gradually increased to a maximum of 8000 units twice a day.
Isoprinosine (Immunovir)(https://livingwithchronicfatiguesyndrome.wordpress.com/2012/11/19/november-2012-a-treatment-update-clonazepam-and-imunovir/)– Isoprinosine may benefit ME/CFS patients due to its effects as an antiviral as well as its various immunomodulatory properties. A study found that 6 out of 10 ME/CFS patients benefited by taking Isoprinosine. In those patients who improved, their CD4+, T-cells and natural killer cells dramatically increased. Dr. Sharp believes Isoprinosine is one of the most helpful, safest and cost effective drugs for ME/CFS patients.
Isoprinosone may increase uric acid levels and therefore shouldn’t be used by those with gout. ME/CFS specialists generally pulse the dosage of Isoprinosine so patients don’t develop a tolerance to the drug.
Low Dose Naltrexone (LDN)(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/02/26/low-dose-naltrexone-for-cfs/)– When used at low doses, Naltrexone causes the body to create more opioids which in turn may; relax the microglial cells, block pain, create endorphins and modulate the immune system. A small, pilot study on Fibromyalgia patients found that subjects experienced on average a 30% decrease in pain and fatigue while taking LDN. A second placebo controlled study on Fibromyalgia patients resulted in 32% of those taking LDN experiencing a significant reduction in pain as well as either a significant reduction in sleep problems or significant reduction in fatigue. Dr. Bihari reports that approximately 50% of ME/CFS patients are helped by LDN. Stories litter the internet of ME/CFS patients benefiting from this treatment.
LDN is considered one of the safest treatments for ME/CFS with few patients experiencing side effects. The most common side effect is sleep disturbance. The dosage used is normally in the 1.5mg-4.5mg range. LDN is generally taken at night before falling asleep.
Magnesium Injections(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/03/09/my-2011-treatments-a-progress-report/)– A study found low red blood cell magnesium levels in ME/CFS patients. After intramuscular magnesium sulphate injections, 12 out of the 15 ME/CFS patients improved compared to 3 out 17 patients receiving the placebo improving. A study determined that despite normal magnesium blood levels, Fibromyalgia patients had low intracellular levels of magnesium. Dr. Myhill has found approximately 70% of her ME/CFS patients improving after receiving magnesium injections.
Magnesium injections can cause temporary pain at the injection sight. High doses may cause diarrhea. Intramuscular injections are generally given once or twice a week.
Melatonin https://livingwithchronicfatiguesyndrome.wordpress.com/2011/03/09/my-2011-treatments-a-progress-report/)– Melatonin is a hormone whose primary role as an ME/CFS treatment is to aid sleep. One study found that it improved ME/CFS patients’ ability to function and that it enhanced patients’ quality of life. Another study concluded that it reduced patients’ fatigue levels. Dr. Wright states that over 60% of his ME/CFS patients produce undetectable levels of Melatonin. As well as improving quality of sleep, this treatment may be beneficial due to its anti-inflammatory and antioxidant effects.
The most common side effects of Melatonin are morning drowsiness and headaches. These side effects may dissipate if the dose is decreased. Melatonin is listed in this section under the ‘prescription treatments’ umbrella due to a prescription being required to gain it in Australia despite formulations with negligible amounts of Melatonin being available over the counter. Other countries may have differing laws regarding prescription requirements to gain Melatonin. Some doctors use doses as low as 0.5mg while most doctors recommend doses in the 3-9mg range. It is normally taken at night, before sleep.
Myers’ Cocktail (https://livingwithchronicfatiguesyndrome.wordpress.com/2011/03/09/my-2011-treatments-a-progress-report/)– The Myers’ Cocktail is an intravenously administered mixture of supplements including; magnesium, calcium, vitamin C, B vitamins and sometimes further ingredients. A study on Fibromyalgia patients receiving this treatment found that most of the subjects noted improvements however the placebo group that received a saline solution also improved. Intravenous saline solution is considered by some to be an effective treatment for ME/CFS/Fibromyalgia hence it is conceivable that both groups did improve. The authors noted that both groups experienced “strong symptomatic relief.” Dr. Teitelbaum is an advocate of Myers’ Cocktails and believes they can provide ME/CFS patients with more energy. Dr. Majid Ali had found that 15 grams of intravenous vitamin C (an ingredient in Myers’ cocktails) can fix the abnormal shapes of ME/CFS patients’ blood cells and hence improve blood flow.
Some patients feel sleepy immediately after a Myers’ cocktail for a short period of time. If the patient feels excessive warmth, dizziness, nausea or a headache during the Myers’ cocktail IV, they should notify the physician. The dosages of the individual ingredients within a Myers’ cocktail vary and are at the physician’s discretion.
Nexavir (Kutapressin)(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/10/25/nexavir-kutapressin-for-cfs/)– Nexavir is a porcine liver extract that is administered via subcutaneous or intramuscular injection. Studies have found that Nexavir can inhibit EBV in vitro and HHV-6 replication in vitro by greater than 90%. A study of 270 ME/CFS subjects found that a staggering 96% of patients receiving more than 40 Kutapressin injections reached remission or near remission status. 71% of patients receiving 11-40 injections obtained remission or near remission levels. If an ME/CFS patient had high EBV-EA-IgG titres, they were more likely to improve in this study. A final Kutapressin study contained 130 ME/CFS patients with 85% noting significant improvements. 43% of patients reached remission while a further 42% of patients gained near remission status (they had a few residual symptoms). Dr. De Meirleir had found 67% of his ME/CFS patients responding to Nexavir in comparison to 17% receiving the placebo improving. Dr. Cheney, Dr. Enlander, Dr. Teitelbaum and Dr. Lapp have all been advocates of Nexavir or an analogous version of Nexavir.
Out of the 400 patients across both Kutapressin\- ME/CFS studies, only 1 person experienced new symptoms and a deterioration of function following Kutapressin injections. Some physicians are reluctant to prescribe antivirals including Valtrex or Famvir due to side effects and therefore prescribe Nexavir as a safer alternative. Nexavir is contraindicated in those allergic to pork or liver products. It shouldn’t be used by those taking MAO inhibitors. The most common dosage is 2mls administered daily although some patients start with a lower dose.
Nimodipine (https://livingwithchronicfatiguesyndrome.wordpress.com/2012/11/26/nimodipine-for-me/)– Nimodipine is a calcium channel blocker that is used to improve cognitive function or reduce pain in other illnesses. Dr. Goldstein found that Nimodipine improved ME/CFS patients’ cerebral blood flow (monitored through SPECT scans) and indeed this is the treatment’s primary usage in ME/CFS patients. Dr. Goldstein has labelled Nimodipine as one of the most useful treatments for both ME/CFS and Fibromyalgia. Dr. Mason Brown has found that Nimodipine helps 20% of ME/CFS patient quickly, another 20% over 6 months and the remaining patients to varying degrees. A report on Nimodipine usage in ME/CFS patients found that 9 out of 13 experienced enhanced mental clarity or improved general functioning.
Possible side effects of Nimodipine include; hypotension, nausea, headache, bradycardia, skin rash and peripheral edema. Specialists generally recommend starting at a low dose (some patients begin with as little as 1/16^th of a tablet). The maximum dose normally recommended for ME/CFS patients is 30-60mg taken 2-3 times a day.
Oxytocin (https://livingwithchronicfatiguesyndrome.wordpress.com/2010/07/05/oxytocin-for-cfs/)– This treatment is a neurotransmitter hormone whose most effective delivery method is widely considered to be injection, followed by nasal spray and finally tablets. The ME/CFS patients most likely to respond to Oxytocin are those with cold extremities. Dr. Flechas states that many ME/CFS symptoms are similar to those that an Oxytocin deficiency would cause. Dr. Goldstein found approximately 20% of his patients benefiting from Oxytocin injections and in those patients who do benefit, the improvement is dramatic. As well as Dr. Goldstein, the ME/CFS specialists; Dr. Lapp, Dr. Flechas and Dr. Teitelbaum all use Oxytocin injections on their ME/CFS patients.
Possible side effects of Oxytocin include; headache, weight gain, irregular heartbeat, nausea and dizziness. Intramuscular injections are sometimes given at 10 units and sublingual Oxytocin has been used by Dr. Cheney at 10 units up to a maximum of three times a day. Oxytocin should not be used by those who are pregnant.
Pentoxifylline(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/09/05/pentoxifylline-for-me/)– Pentoxifylline belongs to a class of drugs called xanthine derivatives and its most common usage is to improve cerebral and peripheral blood circulation. It may also benefit ME/CFS patients by reducing; the cytokine IL-2, lowering NF-Kappa B and downregulating the cytokine TNF-alpha. All three facets of the immune system are thought to be high in ME/CFS patients and potentially contributing to symptoms. Pentoxifylline also has antiviral and further immunomodulatory properties. Dr. Leslie Simpson has noted that Pentoxifylline is useful at reducing cognitive problems and dizziness in ME/CFS patients.
Pentoxifylline should not be taken by those who cannot tolerate stimulants. It should also be avoided by those with a peptic ulcer or at risk of haemorrhaging. The drug hasn’t been well studied in ME/CFS patients but in other illnesses is considered safe and well tolerated at 1200mg per day. The standard dose of Pentoxifylline for various non ME/CFS illnesses is 400mg three times per day.
Rifaximin (Xifaxan)(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/11/11/rifaximin-for-m-e/)– Rifaximin is an antibiotic that may benefit ME/CFS patients due to eradicating small intestinal bacterial overgrowth (SIBO). SIBO involves healthy bacteria in the large intestine being transferred to the small intestine thus causing gastrointestinal symptoms. Dr. Pimentel found 100% (42/42) of Fibromyalgia patients testing positive to SIBO compared to 20% of controls. The degree of pain experienced by Fibromyalgia patients in this study correlated strongly with the amount of hydrogen seen on the lactulose breath test. Rifaximin may also help ME/CFS patients as it balances gut flora. In vitro, 90% of the 536 strains of anaerobic bacteria tested were inhibited in vitro. Anecdotally, a reasonable number of ME/CFS patients have improved whilst on Rifaximin although many patients have had their symptoms return upon stopping the drug. Interestingly, some ME/CFS patients with no gastrointestinal symptoms improve. Dr. De Meirleir, Dr. Teitelbaum, Dr. Peterson and Dr. Myhill all use Rifaximin on their ME/CFS patients with some only using it after positive test results.
Rifaximin is generally well tolerated and only 0.4% of subjects in a traveller’s diarrhea study had to discontinue treatment due to side effects. The most common side effects are gastrointestinal. Long term usage of Rifaximin increases the chances of building resistance to the drug. Some specialists recommend a slightly lower dose of 550mg taken 2 times per day for 8 days. Other specialists recommend doses up to 550mg be taken 3 times per day for 14 days. It is recommended that probiotics are taken after Rifaximin usage.
Sleep Aids(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/09/20/the-best-sleep-aids-for-m-e/)– In the attached link I examine the various prescription sleep drugs that the ME/CFS specialists recommend. Dr. Cheney, Dr. Teitelbaum, Dr. Klimas, Dr. Lapp, Dr. Myhill and Dr. Enlander all have certain sleep inducing and sleep enhancing drugs that they try on their patients in a specific order.
Vitamin B12 Injections(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/01/08/10-of-the-most-effective-treatments-for-cfs/)– Despite often having normal B12 as determined by a blood test, ME/CFS patients commonly have low B12 levels in their brain. High levels of B12 being injected can ensure that sufficient B12 crosses the blood-brain barrier. B12 may also benefit ME patients by acting as a scavenger of nitric oxide, a compound that may contribute to ME/CFS symptoms. A poll found that 50%\-80% of Dr. Lapp and Dr. Cheney’s ME/CFS patients improved to some degree after taking B12 injections. A study found that ME/CFS patients were much more likely to respond to B12 injections if they had more frequent injections, a higher dose of B12, tried the treatment for longer and were taking oral folic acid. The study also found that the concentrated (5mg/ml) methylcobalamin form of B12 tended to be more effective than the hydroxocobalamin form (1mg/ml). Some specialists prefer the cyanocobalamin form of B12 as it is more stable. If an ME/CFS patient doesn’t respond to B12 injections, they may respond to oral folic or folinic acid. B12 is also available over-the-counter in a sublingual form however this isn’t necessarily as effective as the injectable versions. ME/CFS specialists inevitably opt for injectable B12 over other forms. Dr. De Meirleir, Dr. Lapp, Dr. Teitelbaum and Dr. Cheney are amongst a number of ME/CFS specialists to use this treatment.
When taking high doses of B12, a vitamin B complex is recommended to be taken concurrently. Although considered to be a fairly safe treatment, B12 may cause a temporary weakness in some patients. Dosage, type of B12, frequency of injection and method of injection vary depending on the physician’s preference.
# Over-the-Counter Treatments for ME/CFS (Non Prescription)
Artesunate(https://livingwithchronicfatiguesyndrome.wordpress.com/2009/08/25/antiviral-and-immunomodulator-cfs-treatment-i-am-trying/)– Artesunate is a derivation of the herb artemisia and commonly used in the non-ME/CFS realm for its anti-malarial properties. It may benefit ME/CFS patients due to its potential anti-herpesvirus and anti-CMV effects. Using Artesunate, Dr. Cheney has doubled his number of ME/CFS cures and 75% of patients have shown some level of improvement using this treatment. Part of Dr. Cheney’s protocol involves the Artesunate being used concurrently with the herb wormwood.
Some ME/CFS patients taking Artesunate have reported dizziness or tiredness. Dr. Cheney recommends the brand Hepasunate be taken on three days of the week. As opposed to swallowing the capsule, he encourages patients to place half the contents of the capsule under their tongue for a period of a minute followed by swishing it around their mouth and spitting the remnants out.
Benfotiamine and Allithiamine(https://livingwithchronicfatiguesyndrome.wordpress.com/2016/01/11/astaxanthin-b1-variants-elimination-diet-ip-6-naphazoline-and-ranitidine/)– These are alternate versions of high dose thiamine that may be better absorbed. Anecdotally, many patients have improved as a result of these treatments. Studies have shown that a thiamine deficiency can causes similar symptoms to ME/CFS and these symptoms can be resolved (especially fatigue) after treatment with high doses of thiamine. See ‘Thiamine\- High Dose’ for more information about thiamine and ME/CFS.
Theoretically, these treatments should be avoided by those who have cancer. Few side effects have been reported by those taking Benfotiamine and Allithiamine. It is difficult to determine a standard quantity for these ‘high dose’ treatments as patients have tried a wide range of doses. Anecdotally, ME/CFS patients online have commonly taken either 50-200mg of Allithiamine or 300-600mg of Benfotiamine.
Biotin(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/01/29/my-me-treatments-a-january-2014-update/)– Biotin deficiency has many shared features with ME/CFS. Several anecdotal accounts are online that mention Biotin greatly benefiting ME/CFS patients. High dose Biotin is currently being studied, with some promising results, as a treatment in progressive multiple sclerosis.
Biotin is normally a fairly safe treatment with few side effects noted. The dosages used by ME/CFS patients have often been in the 300mcg-1000mcg range. A neurologist from Massachusetts recommended that an ME/CFS patient take; 100mg of B1 (twice a day), 100mg of B2 and the high dosage of 5000mcg of Biotin for treating post-exertional malaise. This treatment benefited the patient.
Butyrate(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/08/05/my-me-treatments-an-august-2014-update/)– Butyrate may improve ME/CFS patients’ gut symptoms by creating T-cells in the digestive system. It may reduce cognitive symptoms, lower inflammation and enhance the immune system. Studies have shown that butyrate may be beneficial in treating ulcerative colitis and Crohn’s disease symptoms.
Butyrate is low in side effects and 1-2 capsules are usually taken with each meal.
Coenzyme Q10– Coenzyme Q10 is a treatment that when taken with L-Carnitine, has superior effects. These treatments both enhance mitochondrial function and hence may benefit ME/CFS patients. The active version of Coenzyme Q10, Ubiquinol is often preferred. A study found a close association between levels of Coenzyme Q10 and severity of ME/CFS. Dr. Lapp has found that about half of his patients benefit from Coenzyme Q10 generally by around 10%\-15%. A University of Iowa study rated Coenzyme Q10 as the leading treatment for ME/CFS with 69% of patients reporting it as beneficial. A study with 20 ME/CFS patients (80% of those deficient in Coenzyme Q10) found 90% had a reduction or complete disappearance of symptoms after 3 months of taking Coenzyme Q10.
There is a theory that taking Coenzyme Q10 as two doses throughout the day can increase its efficacy. There also exists a sublingual version of Coenzyme Q10. Alongside the energy boost that Coenzyme Q10 may provide, it occasionally causes insomnia. Those with diabetes or other types of hypoglycemia should be wary of Coenzyme Q10 as it can reduce blood sugar levels. The daily dose that is used generally varies from 50mg to 300mg.
Cordyceps Sinensis and Shiitake Mushroom(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/03/09/my-2011-treatments-a-progress-report/)– Cordyceps Sinensis may enhance the immune system. A study on healthy subjects found ‘CordyMax’ increased aerobic capacity, reduced fatigue and lowered diastolic blood pressure. Another treatment that is similar to Cordyseps Sinensis is Shiitake mushroom which may increase interferon levels and have antiviral and immunomodulatory benefits. Anecdotally, numerous ME/CFS patients have reported more energy after taking versions of Shiitake mushroom supplements. A Japanese study that used injected ‘Lentinan’ taken from Shiitake mushroom on ME/CFS subjects found patients’ natural killer cell function increased. Recovery of the majority of patients studied took several months. Another study injected Lentinan into ME/CFS patients and found that 6 months of injections was required to normalise natural killer cell activity. Lentinan doesn’t get absorbed orally hence has to be given as an injection. Maitake and Reishi are another two of the many types of mushroom supplements used by ME/CFS patients. A study found that oral Maitake and oral Shiitake mushroom in combination significantly increased natural killer cell function in mice.
Most people that take Cordyceps Sinensis experience no side effects however rarely diarrhea and nausea can occur transiently. In the aforementioned study, subjects took 333mg of Cordymax three times per day with meals. Shiitake mushroom supplements may cause gastrointestinal symptoms or a rash. Shiitake mushroom supplements are sometimes used at daily doses between 400mg-1500mg, with this total daily dose broken up into smaller doses taken several times a day.
Curcumin(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/02/01/sulforaphane-nicotine-gum-curcumin-and-vns/)– Curcumin is a derivation of turmeric. A study found that curcumin benefited mice with ‘CFS.’ Dr De Meirleir has recommended this treatment to some patients. It may reduce cognitive impairment, improve HPA axis dysfunction and have anti-inflammatory and antioxidant properties. A study found that when Curcumin is supplemented with either; olive oil, stearic acid or choline, the brain and blood absorption levels of Curcumin dramatically increase.
Side effects from Curcumin usage are rare however if they do occur are generally of a gastrointestinal nature. Dosages used generally fall within the 500mg-1000mg range. Those with illnesses other than ME/CFS have ventured up to 8 grams of Curcumin a day. The absorption levels of the specific type of Curcumin used are relevant when determining a dosage.
D-Ribose(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/01/08/10-of-the-most-effective-treatments-for-cfs/)– This treatment may improve mitochondrial function and supply the body with energy. A pilot study found that 66% of ME/CFS patients significantly improved while taking D-Ribose. A follow up study involved 203 ME/CFS and Fibromyalgia patients that completed three weeks of treatment. The patients’ experienced: an average energy increase of 61%, a 37% improvement in well-being, a 30% increase in mental clarity, a 29% enhancement in sleep and a 16% reduction in pain.
D-Ribose shouldn’t be used by those with gout as it may raise uric acid levels. Side effects can include nausea, headache and sleepiness. In the above D-Ribose studies, patients took 5 grams of D-Ribose, three times per day. It may be wise to start at a lower dose, to gauge any potential side effects.
Energy Revitalization System(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/01/08/10-of-the-most-effective-treatments-for-cfs/)– This formulation contains a broad range of nutrients including a B vitamin complex. It also contains various amino acids, choline, malic acid and biotin. It was developed by Dr. Teitelbaum and it is claimed that it can replace taking 30 tablets in the one formulation. A number of the ingredients probably aren’t of a high enough dosage to have a therapeutic effect on some patients although other parts of this formulation contain reasonable dosages. Many ME/CFS specialists recommend that patients take a multi-vitamin tablet including Dr. Cheney who labels a quality multi-vitamin as “essential.” Energy Revitalization System isn’t a multi-vitamin tablet but rather a powder containing eclectic ingredients targeted at improving patients’ energy.
A small number of patients taking this treatment experience gastrointestinal symptoms. The typical dosage is one scoop (20.3 grams) per day.
Epicor(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/02/03/beta-glucan-and-coconut-oil/)– Studies have shown that Epicor may improve natural killer cell function (which is almost inevitably low in ME/CFS patients) up to 4-fold. A similar substance, beta-glucan, may regulate other parts of the immune system too. A study that induced mice with ‘CFS’ found that beta-glucan significantly improved the symptoms of the mice.
Epicor and beta-glucan are considered to be fairly safe supplements. The standard dosing of Epicor and beta-glucan ranges from 200mg to 3000mg.
Essential fatty acids (EFA)– Essential fatty acids include such substances as; flaxseed oil, evening primrose oil and fish oil. The first study to examine EFA usage in ME/CFS patients provided patients with both omega-3 and omega-6, resulting in 85% of the patients showing at least moderate improvement. A second study on ME/CFS patients taking EFA found 90% of patients experiencing a reduction in symptoms. Another study that provided patients with eicosapentaenoic acid (EPA) found that all four patients improved while the same patients didn’t respond to a placebo.
Heartburn and gastrointestinal symptoms are some of the most common side effects of fish oil. The recommended dosing of EFA varies depending on what type of EFA product is being used. Fish oil is often used at 3000-4000 mg per day.
Far Infrared Sauna(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/08/05/my-me-treatments-an-august-2014-update/)– A study on 13 ME/CFS patients using a Far Infrared Sauna found two patients dramatically improve. The other 11 ME/CFS patients had a reduction in physical symptoms, lower levels of pain and reduced fatigue. Another study monitored the effects of Far Infrared Saunas on 10 ME/CFS patients. Average fatigue levels reduced on a 10 point scale from 6.7 to 4.8.
It is recommended to hydrate after a Far Infrared Sauna session with electrolytes. Also, many people shower when a session is completed to remove the excess sweat from their body. The Far Infrared Sauna user should also be cognisant of the signs of heat stroke. ME/CFS patients that do trial this therapy should start off for only a short period of time in the Far Infrared Sauna before gradually increasing the time period if they don’t experience side effects. Some patients slowly build up to having a maximum 15-30 minute session per day.
Fucoidan(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/09/14/fucoidan-for-cfs/)– There is limited information online pertaining to ME/CFS patients taking Fucoidan. Despite this, over 850 studies on Pubmed detail many effects that may potentially benefit ME/CFS patients. These include; immune modulation, antiviral, anticoagulant and anti-inflammatory effects. A study found that Fucoidan reduced the amount of fatigue experienced by cancer patients.
Fucoidan is widely considered to be a safe treatment. Some people have experienced transient diarrhea while taking this treatment. Anticoagulants shouldn’t be used while a patient in on Fucoidan. Studies have found that the efficacy of Fucoidan is largely dose dependant. An osteoarthritis study determined that 1000mg per day had a much better effect on subjects that 100mg per day. Fucoidan has been largely untried by the ME/CFS patient community hence appropriate doses are hard to establish.
Germanium(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/10/10/my-2011-me-treatments-a-progress-report/)– A 1988 paper reported that Dr. Greenberg found 25% of his ME/CFS patients showing “substantial clinical improvement” as a result of taking 300mg of Germanium a day. Dr. Maslin in the same paper found 150mg-300mg daily was sufficient to provide significant relief from ME/CFS symptoms in the majority of his patients and found 20% of patients to be non-responders. Dr. Anderson found half of his patients responding favourably to Germanium with doses for some patients needing to be as high as 1 gram.
If patients are keen to take high doses of Germanium, they should have regular tests to monitor kidney function. It may be wise for ME/CFS patients to start Germanium at a low dosage and gradually build up to 300mg per day. As the above specialists’ reports indicate, some patients may need high doses, up to 1 gram a day to experience the effects of this treatment. The safer, medicinal form of Germanium is known as organic Germanium-132, the inorganic form is not recommended for supplemental use.
Hawthorn(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/03/09/my-2011-treatments-a-progress-report/)– Dr. Cheney has been an advocate of Hawthorn and did recommend its use in tandem with the prescription injectable, Nexavir. Hawthorn may improve the heart’s ability to pump blood around the body. Dr. Cheney trialled it on some of his patient and noted that it improved their cardiac output.
In low doses, Hawthorn is non-toxic. Side effects are fairly uncommon but may include; nausea, headaches and palpitations. Doses used generally fall between 200mg-1000mg.
Inosine(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/01/08/10-of-the-most-effective-treatments-for-cfs/)– The supplement, Inosine, is the active ingredient in prescription medication ‘Isoprinosine.’ A study on the prescription version of this treatment found benefits in 6 out of 10 ME/CFS patients. Dr. De Meirleir believes the supplement Inosine is as effective as the prescription formulation. Inosine is antiviral and an immunomodulator. Dr. Sharp has labelled its prescription cousin as “One of the safest, most cost effective and helpful drugs at our (ME/CFS doctors’) disposal.”
Inosine is fairly low in side effects although some patients have experienced insomnia and headaches. Inosine can raise uric acid levels so shouldn’t be taken by those with gout. ME/CFS patients commonly take inosine at a dosage of 500mg three times a day but only on five days of the week. The treatment isn’t taken on 2 consecutive days each week such as the weekend. A pulsing dosing structure of this treatment is recommended so the patient doesn’t build up a tolerance to the Inosine.
IP-6 (Inositol Hexaphosphate)(https://livingwithchronicfatiguesyndrome.wordpress.com/2016/01/11/astaxanthin-b1-variants-elimination-diet-ip-6-naphazoline-and-ranitidine/)– The main mechanism of this supplement is to increase natural killer cell activity which is inevitably low in ME/CFS patients. Dr. Conley reports that he has used IP-6 to increase natural killer cell function in dozens of cases of ME/CFS. He notes one patient who went from being unable to work to working a 32-40 hour a week job as a result of taking IP-6. A related treatment that some patients use is Inositol. Inositol may be useful against insomnia and depression.
IP-6 is generally low in side effects with the most common being gastrointestinal. It is recommended that this supplement be taken on an empty stomach and twice a day. Some ME/CFS patients start with a lower dose of IP-6 such as 500mg and gradually increase this dosage to a total daily dose between 2-8 grams. The dose is taken at two separate occasions each day.
L-Carnitine– This amino acid could potentially benefit ME/CFS patients due to improving mitochondrial function. Acetyl-L-Carnitine may be better absorbed by the body than standard L-Carnitine. When taken in tandem with Coenzyme Q10, the positive effects may be magnified. A research centre found that out of 150 ME/CFS patients taking L-Carnitine, 69% noted an improvement in symptoms. A study found 12 out of 18 ME/CFS patients noting a statistically significant reduction in fatigue as a result of taking L-Carnitine. Another study found that 59% of ME/CFS patients taking Acetyl-L-Carnitine improved, 63% taking Propionyl-L-Carnitine improved but only 37% taking both treatments improved. The study noted that Acetyl-L-Carnitine mainly reduced mental fatigue while Propionyl-L-Carnitine was more likely to lower general fatigue. Studies have found ME/CFS patients low in cellular acylcarnitine levels. Deficiency of acylcarnitine can produce symptoms similar to ME/CFS. A study also found that as acylcarnitine levels improved in ME/CFS patients, symptoms improved.
L-Carnitine should be avoided by those ME/CFS patients with low thyroid. If side effects do occur, they may be of a gastrointestinal nature. L-Carnitine should be taken with food and recommended dosages range from 1000mg to 2000mg per day. Patients often start off with a lower dose before increasing the dosage if no side effects occur.
L-Serine(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/05/31/mecfs-treatments-a-progress-report/)– L-Serine is an amino acid that former ME/CFS specialist Dr. Buttfield believes should help 60% of CFS patients significantly. Dr. Vallings found that 5/6 ME/CFS patients benefited from L-Serine supplementation. A study found that ME/CFS patients had “significantly reduced” levels of L-Serine in their urine when compared to healthy controls. The study continued on to note that those ME/CFS patients with low urinary L-Serine levels had mainly neurological symptoms and high levels of pain.
L-Serine side effects are fairly rare but may consist of sleep disturbance or gastrointestinal symptoms. Dr. Buttfield’s protocol consisted of beginning patients on 500mg of L-Serine in the morning and increasing this dosage to 2 grams per day.
Magnesium– The majority of ME/CFS specialists incorporate either oral magnesium or magnesium injections into their treatment protocol. Dr. Cheney believes magnesium can benefit ME/CFS patients due to; enhancing energy, improving sleep and lowering muscle pain. He advocates oral magnesium glycinate due to its ability to cross the blood-brain barrier and also be absorbed into cells. Other ME/CFS specialists prefer magnesium citrate due to its possible higher levels of bodily absorption.
Another facet of Dr. Cheney’s advocacy of magnesium glycinate is that this treatment is less likely to cause gastrointestinal symptoms. Other forms of magnesium are more likely to cause diarrhea. Magnesium should be taken with food and dosages should begin at low levels before increasing to the 200mg-400mg range.
NADH– This treatment is a form of coenzyme 1. A study found that 31% of ME/CFS patients improved while taking NADH in comparison to 8% of the control group improving. 18 out of 25 (72%) of ME/CFS patients enrolled in the longer follow up version of this study noted improvements. There is some evidence that it may take up to 6 months before certain ME/CFS patients respond to this treatment.
Side effects tend to be rare but mild overstimulation is possible. NADH should be taken on an empty stomach, before breakfast. Recommended dosages range from 5mg up to 20mg per day.
Naphazoline HCL(https://livingwithchronicfatiguesyndrome.wordpress.com/2016/01/11/astaxanthin-b1-variants-elimination-diet-ip-6-naphazoline-and-ranitidine/)– Dr. Goldstein, who was an ME/CFS specialist, always tried Naphazoline HCL 0.1% eye drops as an initial treatment when a patient stepped into his office. He claimed that 20% of patients benefited from this treatment and in those patient who benefited, the benefits were remarkable and immediate. He theorised that those patients in the cohort of having severe anxiety were the most likely to respond. In some countries such as Australia, Naphazoline HCL is available over-the-counter.
The delivery process of this treatment involves placing a drop in each eye. Due to the nature of Naphazoline HCL, any benefits will be felt almost instantaneously. One of the most common side effects is local irritation. The occurrence of more serious side effects from this treatment is unlikely but may include; dizziness, headache or nausea. The dosage of the Naphazoline HCL eye drops used should be 0.1% and not 0.01%.
NeuroProtek(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/10/10/my-2011-me-treatments-a-progress-report/)– NeuroProtek contains a number of eclectic supplements; luteolin, quercetin and rutin in tandem with the antioxidant, olive kernel oil. Anecdotally, many ME/CFS patients have reported a reduction in cognitive impairment as a result of taking NeuroProtek. A drawback is that often the cognitive impairment returns when the patient ceases taking the treatment. Neuroprotek may be able to normalise mast cell function.
Side effects of NeuroProtek are rare however caution is advised if the patient is concurrently taking drugs that are metabolised by the liver as NeuroProtek may alter the blood levels of these substances. The dosage of NeuroProtek is dependent on the patient’s weight, with a daily dose being 2 capsules taken per 20kg (44lbs) of body weight. The maximum dose, regardless of body weight is 8 capsules per day. Capsules should be taken with food and the dosage spread out across the day.
Nicotine Gum(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/02/01/sulforaphane-nicotine-gum-curcumin-and-vns/)– Former ME/CFS specialist, Dr. Goldstein wrote fondly of Nicotine Gum as a treatment for ME/CFS. He noted that patients experienced an improvement in energy, cognition and mood as a result of this treatment although did caution that some patients may get worse. It potentially benefits ME/CFS patients due to inhibiting brain inflammation. Several patients have noted an improvement in cognition and increase in energy as a result of this treatment.
Nicotine Gum can be detrimental to those with Crohn’s disease. Dr. Goldstein stipulates that occasional patients will have a worsening of ME/CFS symptoms as a result of taking this treatment. If a patient does improve on this treatment, benefit will be noted soon after taking the gum. One ME/CFS patient took a week before experience more energy. Nicotine may increase blood pressure which may be detrimental if an ME/CFS patient has high blood pressure. Longer term use of nicotine is also conducive to health problems such as addiction, periodontal problems and hair loss. If this treatment is trialled, a low starting dose is imperative.
Oxymatrine(https://livingwithchronicfatiguesyndrome.wordpress.com/2009/11/03/oxymatrine/) (Equilibrant(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/01/29/my-me-treatments-a-january-2014-update/))– Equilibrant is Dr Chia’s own formulation of Oxymatrine that also contains; Astragalus, Olive Leaf, Liquorice and Shiitake Mushroom. Oxymatrine, derived from the Sophora plant, is thought to be effective against enteroviruses. Dr. Chia has trialled Oxymatrine on 500 ME/CFS patients and has found approximately 52% of his patients improve as a result of taking this treatment.
Common side effects of Oxymatrine can include headache, fatigue or an increase in ME/CFS symptoms. Oxymatrine should be avoided by those with autoimmune tendencies or seizure disorders. A low starting dose of Oxymatrine is essential for ME/CFS patients and the dosage should only be titrated upwards after a week. The maximum dosage of this treatment is in the realm of 200mg taken in the morning and 200mg taken in the afternoon. Dr. Chia’s Equilibrant doesn’t list the amount of Oxymatrine in the product however the recommended initial dosages of this product is 1 tablet per day for 1-2 weeks. This is followed by a gradual increase of dose, with patients taking up to a maximum of 6 tablets per day.
Piracetam(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/04/04/piracetam-for-mecfs/)– Piracetam is a supplement that specifically targets enhancing cognition. It may also benefit ME/CFS patients due to increasing blood circulation. A study that gave fatigued patients (not necessarily those with ME/CFS) Piracetam and Cinnarizine (an antihistamine) found that patients’ physical fatigue significantly reduced. There exist several similar products to Piracetam that may also benefit ME/CFS patients and these are classed as nootropics.
In non-ME/CFS studies, Piracetam has rarely caused side effects. One study ascertained that 12% of subjects experienced sleep disturbances while taking this treatment. If a headache does occur while a patient is taking Piracetam, Choline may be a beneficial tandem treatment. Anecdotally some ME/CFS patients have stated that they can only tolerate a small dose of Piracetam\- in the 100mg range. Other patients even find this dose too stimulating. Starting at the normally recommended dosage is not recommended for those with ME/CFS. The dosage of Piracetam used for other indications can be up to 20 grams per day. ME/CFS patients generally require much smaller dosages in the 0.8-4.8 gram range. This dosage is spread out across the day and taken at three different occasions at 8 hour intervals. Different countries have various classifications on Piracetam pertaining to its over-the-counter or prescription status.
Post-Exertional Malaise Treatments(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/07/18/how-to-gain-relief-from-post-exertional-malaise/)– This debilitating and central symptom of ME/CFS is often overlooked by doctors. There exists a range of treatment worth trying that I’ve written about in the attached link that benefit patients to varying degrees once in a ‘crashed’ state. These include; Hydralyte iceblocks, liquorice, D-Ribose, electrolyte solutions, leg elevation, massage, meditation, warm baths or cold baths.
ProBoost(https://livingwithchronicfatiguesyndrome.wordpress.com/2009/08/25/antiviral-and-immunomodulator-cfs-treatment-i-am-trying/)– Also known as thymic protein A, a study found 16 out of 23 ME/CFS patients experienced a normalisation of immune function as a result of taking this treatment. There was a corresponding improvement in the clinical ME/CFS symptoms of patients in this study. Another study examined the use of thymic protein A in 6 ME/CFS patients with high EBV titre levels. Patients experienced an increase in energy and required less sleep to function. There exist several reports online of patients greatly benefiting from ProBoost. Many ME/CFS patients who feel run down or on the precipice of a virus take ProBoost.
Side effects as a result of taking ProBoost are rare with occasional patients reporting mild, flu like symptoms when they start this treatment. The dosage used varies depending on whether the patient is taking it as a maintenance dosage\- 1 packet a day or are fighting off an acute infection\- 3 packets per day. Dr. Teitelbaum recommends that ME/CFS patients take one packet of ProBoost, 3 times a day.
Propax with NT Factor(https://livingwithchronicfatiguesyndrome.wordpress.com/2011/10/10/my-2011-me-treatments-a-progress-report/)– This product contains a number of treatments all in the one formulation. Many of these lone treatments are individually used by ME/CFS patients including; quercetin, L-Glutathione, NAC, grape seed extract, various B supplement and NT factor. A study that was ominously run by the company that produces this product found that those with the symptom of severe fatigue (not necessarily ME/CFS) experienced a reduction in fatigue by on average 40%. Another study found Propax with NT Factor reduced the fatigue experienced by cancer patients. Propax with NT Factor is potentially a form of ‘lipid replacement therapy’. This entails repairing damage to a patient’s mitochondrial membranes. A study examined lipid replacement therapy’s efficacy on ‘moderately fatigued patients.’ As subjects mitochondrial function improved while taking lipid replacement therapy, their fatigue proportionally reduced.
Propax with NT Factor is considered to be a safe product with gastrointestinal symptoms rare but possible. It is recommended that the packet be consumed 2-3 times a day. The tablets in the formulation can be taken with or without food and the soft gel capsule that contains omega-3, EPA and DHA should be taken with food.
Ranitidine(https://livingwithchronicfatiguesyndrome.wordpress.com/2016/01/11/astaxanthin-b1-variants-elimination-diet-ip-6-naphazoline-and-ranitidine/)– Ranitidine is a treatment that former ME/CFS specialist Dr. Goldstein found benefited those with infectious mononucleosis. He then began using this treatment on ME/CFS patients with some success. If Ranitidine is not available over the counter in a country, often the alternative Cimetidine is. Dr. Goldstein has found that about 90% of mononucleosis cases respond to Cimetidine. When an ME/CFS patient does respond to one of these drugs, Dr. Goldstein notes that the recovery is remarkable. Approximately 20% of Dr. Goldstein’s ME/CFS patients respond to this type of drug.
Stimulation and headaches are two of the most common side effects of Ranitidine treatment. Dr. Goldstein recommends that 150mg of Ranitidine be taken twice a day. The alternative, Cimetidine, should be taken at 300-400mg. Dr. Goldstein has written that it may take from one hour to one week before a patient notices whether this treatment is working for them.
Selenium (high dose)(https://livingwithchronicfatiguesyndrome.wordpress.com/2014/08/05/my-me-treatments-an-august-2014-update/)– Numerous patients online have noted great benefit from this treatment. The symptoms that have generally improved in these patients are cognitive ability and energy. High dose Selenium may benefit ME/CFS patients due to its antiviral and strong antioxidant properties.
Taking high dose Selenium for more than several months is not recommended as it may increase the chance of toxicity, although Selenium toxicity generally occurs at higher doses (the 2400-3000mcg range). Overdosing on Selenium can cause numerous symptoms. The recommended dosage of the high dose Selenium protocol is between 400-800mcg a day. Some ME/CFS patients have noted side effects if they increase the dosage past 400mcg. The Selenium should be taken on an empty stomach to increase absorption. Yeast-free selenomethionine is thought to be the best form of Selenium to take although other forms may benefit certain patients more effectively.
Sleep Aids(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/09/20/the-best-sleep-aids-for-m-e/)– In this link I present various ME/CFS experts’ opinions on sleep aids including many over-the-counter formulations.
Sulforaphane(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/02/01/sulforaphane-nicotine-gum-curcumin-and-vns/)– This compound may benefit ME/CFS patients due to shifting the immune system from Th2 dominant to Th1 dominant. Sulforaphane is also an antioxidant, neuroprotective, defensive against oxidative stress and may improve mitochondrial function. It has been studied in autism and benefited those who took it through a mechanism the authors suspected may be due to inducing a “fever effect.”
In the aforementioned autism study, those taking Sulforaphane experienced a tiny increase in their liver enzymes. There is quite some conjecture about the amount of Sulforaphane the body absorbs. This is partly due to the possible discrepancy between the specific forms of Sulforaphane ingested. It is therefore difficult to pinpoint a commonly used dosage.
Thiamine (high dose)(https://livingwithchronicfatiguesyndrome.wordpress.com/2013/08/05/an-me-update-august-2013/)– Anecdotally, some ME/CFS patients have reported benefits from taking high doses of thiamine (vitamin B1). A small study of Fibromyalgia patients found all 3 patients benefiting from high dose thiamine treatment. Thiamine deficiency (which can be caused by a defective enzyme system) can produce similar symptoms to ME/CFS. A study found that fatigue associated with ulcerative colitis and Crohn’s disease can be caused by a thiamine deficiency and that high doses of thiamine resolved this fatigue. Despite this, across multiple studies examining various disease state, patients have normal blood thiamine levels yet improve significantly when taking high dose thiamine. A study has speculated that this may be due to low cellular thiamine transportation or enzymatic problems.
The three Fibromyalgia patients studied experienced no side effects as a result of high dose thiamine. Patients with other disease states taking high dose thiamine have reported insomnia and tachycardia. In the Fibromyalgia\- high dose thiamine study, patients started at 600mg of thiamine a day and gradually increased this dose. Abrupt improvement was seen when patients reached 1800mg a day. Anecdotally, ME/CFS patients that have responded to high dose thiamine seem to have an optimal dose that varies from patient to patient. The challenge is to find this optimal dose without exceeding it and experiencing any side effects. If a patient doesn’t respond to thiamine, they may benefit from Benfotiamine or Allithiamine, which may be better absorbed.
Vagus Nerve Stimulation(https://livingwithchronicfatiguesyndrome.wordpress.com/2015/02/01/sulforaphane-nicotine-gum-curcumin-and-vns/)– Dr. VanElzakker has theorised that the vagus nerve being infected could explain many of the features of ME/CFS. The vagus nerve has been implicated in several other illnesses such as epilepsy, with stimulation of the nerve proving beneficial. A study implanted Fibromyalgia patients with a vagus nerve stimulation device with the authors concluding that it was a “useful adjunct treatment.” A less invasive measure to stimulate the vagus nerve involves attaching a TENS machine’s electrode pads to the tragus part of the ear.
Vitamin D– Vitamin D deficiency can often be a secondary problem that arises when ME/CFS patients are unable to get proper supplementation from sunlight. A retroactive study of 221 ME/CFS patients found that Vitamin D levels were “moderately to severely suboptimal in CFS patients.” Numerous patients online have benefited to some degree from Vitamin D supplementation. Dr. Lapp recommends Vitamin D3 to almost all of his ME/CFS patients.
Vitamin D side effects are rare at normal doses yet high Vitamin D may cause weakness, headaches or gastrointestinal symptoms. Some patients gain Vitamin D from sunlight or through daily lower level supplementation in the 1000-2000IU range that is available over-the-counter. To definitively raise Vitamin D levels, a single or once a month for several months prescription dose may be required. This may on occasions be as high as 100,000IU. Blood tests can monitor Vitamin D levels yet there is some conjecture about what levels are considered suboptimal. Studies have suggested that those with any form of chronic illness should try and maintain higher vitamin D levels than the healthy population.
## About These Lists
The key purpose behind creating the above lists was to show patients who have lost hope that there are treatment ideas for this illness. Another purpose of these lists was to compile much of the information that was spread haphazardly across this blog in a centralised and easy to access location.
As I continue to write about other ME/CFS treatments on my blog, I will add them to this treatment page. There are many more treatments that I didn’t include in the above lists but ME/CFS patients may benefit from. The following are just some treatments that may help ME/CFS patients based on either study results or their use by some ME/CFS specialists; various probiotics, Glutathione, N-Acetyl Cysteine, methylation cycle treatments, MAF 314, IV saline solution, Gamma Globulin injections/IV, Lidocaine IV, Valtrex, Valcyte, Ergoloid, Levofolinic Acid, Nifedipine, Galantamine, Ampligen and Rituximab.
There seems to be a degree of disease heterogeneity(https://livingwithchronicfatiguesyndrome.wordpress.com/2010/10/09/a-meta-analysis-of-the-efficacy-of-graded-exercise-therapy-in-treating-cfs-part-3/) across the entire collection of ME/CFS studies and indeed often within single ME/CFS studies. Some studies require that just the overly broad Oxford Criteria be met for patient inclusion. In contrast, other studies are narrower and demand more severely affected patients sharing more common symptomology. Many ME/CFS studies aren’t adequately funded and hence; don’t have a high number of participants, lack a placebo group and aren’t considered high quality. If these idealistic studies existed, I would have written more about these and the corresponding treatments but unfortunately they don’t.
It is for the above reasons that I often place a greater emphasis on what an ME/CFS specialist (who has stringently diagnosed ME/CFS) has found the clinical response rate of a treatment to be e.g. 30% of responders. This is why I have attempted to include as many clinical observations and comments from ME/CFS specialists as possible in the above lists.
Finally, I should emphasise that patients should always consult with their physicians prior to taking any treatment. I am not a doctor and nothing on this blog should be construed as medical advice. It is imperative that patients and their physicians are aware of possible side effects, including those not listed before starting any treatment. Patients should also be aware of possible interactions between any treatment they commence and their current medications. Some treatments listed are recommended for short term use only while other treatments may require up to 6 months of usage before effects may be noticed. ME/CFS patients are renowned for having a higher sensitivity to treatments than patients with other diseases. In many cases it is wise to begin treatments at a lower dose to mitigate the chance of more severe side effects.
\*
From: 'DR. JAY GOLDSTEIN: A-Z TREATMENTS' http://www.cfstreatmentguide.com/dr-jay-goldstein-a-z-treatments.html
A Typical Neurosomatic New Patient Treatment Protocol
*Agents tried sequentially Onset of Action Duration of action*
1. Naphazoline HCL 0.1% gtt ┬OU 2 - 3 seconds 3 - 6 hours
2. Nitroglycerin 0.04 mg sublingual 2 - 3 minutes 3 - 6 hours
3. Nimodipine 30 mg po 20 - 40 minutes 4 - 8 hours
4. Gabapentin 100-800 mg po 30 minutes 8 hours
5. Baclofen 10 mg 30 minutes 8 hours
6. Oxytocin 5-10 U IM or BID
or
Syntocinon 1-2 puffs TID 15 minutes - 72 hrs 12 - 24 hours
7. Pyridostigmine 30 - 60 mg po 30 minutes 4 - 6 hours
8. Hydralazine 10 - 25 mg po 30 - 45 minutes 6 - 12 hours
9. Mexiletine 150 mg po 30 - 45 minutes 6 - 8 hours
10. Tacrine 10 mg 30 minutes 4 - 6 hours
11. Risperidone 0.25 - 0.5 mg 45 - 60 minutes 8 - 12 hours
12. Pindolol 5 mg BID 15 minutes - 7 days 12 hours
13. Lamotrigine 25 - 50 mg QD 30 - 45 minutes 24 hours
14. Sumatriptan 3 - 6 mg SQ 15 - 30 minutes 16 hours
15. Ranitidine 150 mg BID 1 hour - 1 week 12 - 24 hours
16. Doxepin HCL elixir 2 - 20 mg HS 1 hour variable
17. Sertraline 25 - 50 mg QAM
or
Paroxetine 10 - 20 mg QAM 1 hour - 8 weeks 1 - 2 days
18. Bupropion 100 mg TID 30 minutes - 8 weeks 8 - 24 hours
19. Nefazodone 100 - 300 mg BID 2 - 8 weeks 24 hours
20. Venlafaxine 37.5 - 75 mg BID 1 - 4 weeks 24 hours
21. Glycine powder 0.4 Gm/Kg/day in juice
or
Cycloserine 15 - 20 mg QD 1 hour 24 hours
22. Felbamate 400 mg 30 minutes 6 - 8 hours
23. Lidocaine 200-300 mg
A-Z Treatments (Comments are by Dr. Goldstein)
*Acetazolamide* (*Diamox*): This drug is a carbonic anhydrase (CA) inhibitor which is routinely used as a cerebral vasodilator in nuclear medicine. Patients will occasionally have a reduction in symptomatology with acetazolamide. Acetazolamide 250 mg eliminated the pain of a 41-year-old female patient with post-traumatic fibromyalgia, helped her feel very relaxed, and markedly reduced her other symptoms.
*Acetyl-L-Carnitine*: In theory, a good drug. It should work as an acetyl group donor to increase acetylcholine, and the carnitine has already been shown to be effective in a double-blind experiment by the Drs. Plioplys. Acetyl-L-carnitine also increases the levels of nerve growth factor (which are four times normal in the spinal fluid of FMS patients) and increases other transmitters like adenosine and ATP. In practice, a semi-dud.
*Adderall*: An amphetamine combination that a few patients find more energizing than plain dexedrine. Only about a third of CFS patients have a good response to stimulants, which act by squeezing dopamine (DA) and norepiniphrine (NE) out of neurons and glia. If these transmitters are much too low already, giving stimulants will further lower the signal-to-noise ratio and increase symptoms.
*Amantadine*: A weak NMDA antagonist. Helpful for a few patients. Doses higher than the PDR recommends may be more effective, but there is an increased risk of adverse drug reactions when exceeding this dose. Israelis have given 100 mg IV with good results in neurogenic pain. IV amantadine is not available in the USA. Amantadine, ketamine, dextromethorphan, and a new MNDA antagonist, memantine, can be used in trigger point injections as well as gel applications for local pain.
*Ambien*: The best sleeping pill. Does not cause dependence except in unusual circumstances.
*Aricept*: A cholinesterase inhibitor marketed for Alzheimer's disease. Has the advantage of once-a-day dosing and no requirement for liver function test. Does not work as well as Cognex, perhaps because it is not a potassium channel blocker. Cognex has several effects on neurotransmitters relevant to CFS/FMS.
*Ascorbic Acid* (*Vitamin C*): Recent research into the role of ascorbic acid in the brain (which has the highest concentrations of this substance in the entire body) has shown that this agent may be beneficial in certain patients with CFS. Ascorbate has been found to be neuroprotective, particularly by inhibiting the redox site of the NMDA receptor and diminishing calcium influx. Trials of high-dose oral ascorbic acid have been generally disappointing. Administration of ascorbic acid is done via IV doses of 25 to 50 grams diluted in half-normal saline of Ringer's lactate over a period of about 90 minutes. Adding magnesium sulfate is recommended because ascorbic acid can cause magnesium shifts from extracellular to intracellular compartments. It is beneficial to add 500 mg of calcium gluconate since ascorbic acid is a calcium chelator and could possibly lower serum calcium. Responders to IV ascorbic acid generally feel considerably better in most respects the day after treatment.
*Baclofen*: A greatly under used medication. A GABA-B agonist with few ADRs, it has an immediate onset of action and is still in my top 10.
*Vitamin B12*: Besides being vital to transmethylation (which helps to synthesize NE), B12 2g. orally in AM decreases inappropriate daytime melatonin secretion, thereby aiding in the treatment of the delayed sleep-wake cycle many CFS patients experience. Very large doses (10 g) may aid transmethylation.
*BuSpar*: The ideal anxiolytic in all respects except efficacy. Best used as an SSRI augmentation agent, especially combined with Visen (not generic Pindolol). Augmentation strategies, of which there are many, do not work nearly as well in CFS as they do in major depression disorder.
*Clonidine*: Another greatly underused drug. Can be good for central pain, ADD, anxiety. Helps all symptoms in some patients. Eliminates nightmares. Safe and cheap. Comes in a patch that lasts all day. Better than Zanaflex, another alpha-2 agonist. Tolerance and depression have not been much of a problem. Adverse drug reactions to clonidine can be reversed by yohimbine, an alpha-2 antagonist. Guanfacine (Tenex) is a less sedating alpha-2 antagonist with a 24-hour duration of action.
*Dexedrine*: An effective stimulant. Makes some patients calm also. May synergize with Ultram. Desoxyn may be better but has neurotoxicity. Many patients like Adderall more.
*Depakote*: In the CFS population its only value is in migraine prophylaxis, for which it is excellent.
*Dilantin*: Useless in every CFS patient I have treated with it.
*DHEA*: Theoretically excellent, it is a neurosteroid which is a GABA antagonist, not necessarily a good thing for some patients. Pregnenolone should be the best neurosteroid (low in PMS).
*Felbamate*(*Felbatol)*: Not used much because of requirement for hematologic and liver function test monitoring. Should be tried in every treatment-resistant patient. May work when nothing else does, especially for intractable headaches. It may cause headaches, however. There's no free lunch.
*Gabapentin* (*Neurontin*): Gabapentin, an antiepileptic drug with a novel mechanism of action, has become one of my five favorite medications (the others are oxytocin, nimopidine, baclofen, and intravenous lidocaine) to treat neurosomatic disorders.
*Gabitril*: The only GABA reuptake inhibitor (like Prozac is a serotonin reuptake inhibitor). Very effective and very safe if you follow PDR dosing suggestions. Increase the dose too rapidly and the patient may get delirious or manic. Effects are reversible with flumazenil if necessary.
*Gingko Biloba*: Useful only for sexual dysfunction induced by serotonin reuptake inhibitors (SRIs). Inhibits platelet aggregation. Rare reports of brain hemorrhage. This adverse reaction raises the risk/benefit ratio.
*Ginseng Saponins*: Works a little like nitroglycerin, which converts to nitric oxide. Increases energy slightly.
*Gotu Kola*: A mild stimulant with no apparent adverse reactions.
*Honey Bee Venom*: As with any "natural product," bee venom has a multitude of ingredients. Patients should be skin tested for bee venom allergy first. Major constituents from my point of view are phospholipase A2 (PLA2), which makes arachidonic acid, the precursor to eicosanoids (prostaglandins, leukotrienes, etc.), dopamine and NE. When it works, the patient often feels like he has been injected with rocket fuel. Effects last about one to two weeks. Has made three patients worse, two of whom were father and daughter. Patients should have an Epi-Pen (if available) and an antihistamine with them at all times. Plaquenil antagonizes PLA2. Arachidonic acid combines with effianolamine in the brain to make anandamide, an endogenous cannabinoid (like marijuana).
*H2 Receptor Antagonists*: The first treatments I developed for CFS were cimetidine and ranitidine. I based this therapy on my successful experience treating acute infectious mononucleosis with cimetidine. When a CFS patient responds to an H2 antagonist (I use ranitidine), the onset of action is similar to that seen in acute infectious mononucleosis, i.e. one or two days at a dose of 150 mg b.i.d. Usually all symptoms are ameliorated. Some patients are unable to take any does of ranitidine because it makes them “hyper.”
*Hydergine*: The most underused effective medication in the PDR. Extremely safe. A dopamine and acetylcholine agonist. There is nothing else like it. Other dopamine agonists seem to be restricted in action to the nigrostriatal dopaminergic tract, which is not important in CFS symptoms. Not the case with Hydergine, which is quite helpful for alertness, especially in those sedated by Baclofen. As with most medications listed, it can sometimes help all symptoms.
*Oxytocin*: Oxytocin has a wide range of behavioral effects. Oxytocin neurons project to many areas of the limbic system, as well as to the frontal cortex. Oxytocin is involved in maternal behavior, female and male sexual behavior, feeding, social behavior, and memory. It also has effects on cardiovascular, autonomic, and thermoregulatory processes. Approximately one-fifth of my patients have a good response to IM oxytocin after failing to respond to numerous oral agents. Cognitive clarity is the most responsive symptom, with fibromyalgia and pain being second.
*Kava-Kava*: One of the two best "natural products" for CFS. May take up to eight weeks to have an effect. No adverse drug reactions.
*Ketamine*: The best single agent for CFS/FMS and all other neurosomatic disorders. Known best as an NMDA receptor antagonist (the NMDA receptor is one of the several receptors for the excitatory amino acid glutamate), it increases dopamine in the limbic system, a very important objective in CFS. I administer it by slow intravenous infusion or in PLO gel for transdermal (through the skin) absorption. The intravenous route is more effective, but transdermal application can be done daily, and if effective, can obviate peaks and valleys and need for IVs. I have seen no cases of Ketamine abuse among my patients. Ketamine is one component of my "resurrection cocktail," for patients who have been bedridden for more than a year and whom I may only see once. The others are IV ascorbate, IV lidocaine, IV thyrotropin\- releasing hormone (which raises all biogenic amines plus acetylcholine), Nimotop, and Neurontin (still the most effective oral agent but is being pushed by Tasmar). I am doing trials with Ketamine eyedrops.
*Klonopin*: The benzodiazepine to use if you are going to use one. Affects neurosteroid biosynthesis.
*Kutapressin*: I don't know how this drug works, but some patients have immediate symptomatic improvement after 2 ml IM. I don't usually prescribe it otherwise since there are so many immediate-acting options. It does increase bradykinin, and adverse drug reactions may be treated with drugs like Vasotec (ACE inhibitors).
*Lamictal*: One of the new anti-epileptic drugs. All of them increase GABA, and most of them are N-methyl-d-aspartate (NMDA) antagonists. Works immediately. The main adverse drug reaction is a rash, which can be minimized by gradual dosage escalations. Affects all symptoms. 50-100 mg of Larnictal and 800-1200 mg of Neurontin have rendered euthymic in 30 minutes every patient with acute manic excitement I have treated. Zyprexa and Rilutek could be added to this cocktail if necessary. Lamictal is also an antidepressant and may also work over four weeks or so.
*IV lidocaine*: In addition to its actions mentioned in *Betrayal by the Brain*, it also acts as an NMDA antagonist. It is the second best treatment. I have given it about a thousand times without a serious adverse drug reaction. Patients have come with great difficulty from other states or countries with the common lament of "If you can't help me I'm going to kill myself' (I hear this about twice a week). At least two patients, achieving complete symptomatic relief with IV lidocaine, returned home and could not find a physician or nursing service to administer it. Since they could not move to southern California, they were again bedridden and had to crawl to the bathroom. Not able to live this way any longer, they committed suicide, a worse outcome than the lidocaine toxicity, which never happens. Many physicians will not prescribe any of the medications I use, even if they help their patients a lot. Some medium-sized cities have not one physician who will care for CFS patients. I must treat them from afar, a hazardous practice medicolegally.
*Marinol*: Marinol-deta-9-tetrahydrocannobinol is a medication I use rarely, because of the medicolegal implications. Among other things, it is a dopamine agonist in the limbic system (at the nucleus accumbens, a key structure in CFS), but an indirect one. It is also a calcium channel blocker. A few patients get total symptomatic relief with Marinol when one hundred other medications have failed. One such patient is applying for disability only because she cannot afford it. It is one of the last and best options for treating the diffuse pain of FMS, and is good for atypical facial pain. In five years it should be used routinely in many situations.
*Methadone*: Another drug I don't use very often, and for the same reason, although California has passed a law that physicians cannot be prosecuted for using opioids responsibly to treat chronic pain. Thus, it is less risky for me. Physicians in some states are afraid to prescribe it. It is the opioid of choice. Besides being an agonist at the mu opioid receptor, it is an NMDA receptor antagonist (like Ketamine), and blocks the serotonin transporter (like SRIs). I described its use as an antidepressant about 15 years ago in the medical literature. It is very cheap, does not produce much opioid euphoria, and often ameliorates all neurosomatic symptoms.
*Nicotine Patch or Gum*: I have been prescribing nicotine in these forms for a long time. Nicotine is analgesic, probably by virtue of its stimulating secretion of dopamine and norepinephrine. It binds to the nicotinic cholinergic receptor and can also have profound effects on mood, energy, and cognition. An occasional patient will have worsening of symptoms with nicotine.
*Papaverine SA*: Marketed many years ago as a vasodilator, this medication will probably be discontinued shortly. It is the only drug available that inhibits adenylate cyclase, thereby increasing cyclic AMP, which you may recall from biology class as being pretty important. There is an experimental antidepressant, rolipram, which has a similar mode of action. It preferentially affects energy, alertness, and cognition, and has very few adverse drug reactions. It is a top-10 drug (cheap, too).
*Pentazocine* (*Talwin*):Occasionally, an extremely treatment-resistant individual has felt much better after taking pentazocine plus naloxone (Talwin-Nx).
*Spironolactone (Aldactone)*: Spironolactone (a mineralocorticoid receptor antagonist) has been used for several years to treat premenstrual syndrome. My experience with spironolactone is that it helps only occasionally, but the effect is rapid (30 minutes or so), and thus can be assessed while the patient is in the office.
*St. John's Wort*(*Hypericum*): The other good "natural" remedy for CFS.
*Tasmar* (*Tolcapone*): Neither an exotic location on the Silk Road nor a Mafia-run turnpike in Chicago, Tasmar is a unique agent. It inhibits the enzyme catechol-ortho-methyltransferase (COMT), one of the two enzymes (monomine oxidase is the other) that metabolizes dopamine and norepinephrine. Tasmar degrades them in the synaptic cleft. I have been waiting for this drug for years. It is marketed for Parkinson's disease, and most physicians have not heard of it yet. It can work as monotherapy, either acutely or after four weeks or so. It may be more effective (immediately) when combined with a dopamine agonist such as Requip (quinpirole) or a reversible inhibitor of monoamine oxidase (RIMA) such as meclobemide, which due to the wisdom of the FDA is available in every other industrialized country in the world but the USA. The package insert advises against combining it with irreversible MAOIs such as Nardil and Pamate, so I have not done so. This combination would leave reuptake as the only mechanism to terminate the post-synaptic effect of catecholamines, although rats do quite well on the two drugs. An accountant, unable to work for three years, is back to work now on meclobemide and Tasmar. Adding Sinemet may enhance the action of Tasmar, since it is metabolized to dopamine. Sinemet may be given instead of Requip or Mirapex, or concomitantly. Requip and Mirapex are useful in that they are D3 agonists also. The D3 receptor is located primarily in the limbic system. Since COMT is a methyl group acceptor, it may work better by combining it with S-adenosylmethionine (SAMe), a methyl group donor with no adverse drug reactions, effective in FMS and depression. SAMe is available in many other countries, and certain buyer's clubs will supply you with it. Tasmar inactivates COMT, allowing SAMe to transfer methyl groups to precursors so that more norepinephrine can he formed. This process is termed "transmethylation" and is too complicated to discuss further in this column. Interested readers may consult the work of John R. Sinythies and R.J. Baldessarini and go from there.
*Topamax*: Another new AED, Topamax has a little more affinity for the ANWA glutamate receptor, as well as the NMDA receptor. It has very few adverse drug reactions, and when it works, is quite energizing. Agonists at the third major class of glutamate receptor, the "metabotropic," of which there are of course various subtypes, are being developed as anxiolytics.
*Viagra*: I don't have enough money to buy stock in anything, but buying Pfizer a few months ago would have been almost as good as buying Microsoft in 1985. This drug works by inhibiting type 5 phosphodiesterase, one of the six known enzymes to degrade cyclic GMP (as important as cyclic AMP, but maybe not covered in biology class). Type 5 is supposed to be specific for the corpus cavemosurn of the penis and probably the clitoris as well. It is not all that specific, though, at least in my patients, who frequently experience flushing and headache. When Viagra works in CFS/FMS, patients experience a reduction in all symptoms. One patient whom I have been treating for 10 years had not responded to one medication until she took Viagra, whereupon she felt almost normal. Nitroglycerin and hydralazine, which stimulate cyclic GMP by different mechanisms, had not helped her.
*Zyprexa*: One of the new "atypical neuroleptics," with Risperdal and Seroquel, Zyprexa can he used as a sleeping aid, antidepressant, anxiolytic, and of special relevance to my practice, is probably the most effective treatment for borderline personality disorder. You can look up the symptoms in the DSM-IV, personality disorder.
SOURCES:
“Treatment Protocol for Physicians.” *The National Forum:* http://www.ncf-net.org/forum/jay.htm
*Dr. Goldstein's summary of his protocol for physicians.*
Goldstein, Jay A.*Betrayal by the Brain: The Neurologic Basis of Chronic Fatigue Syndrome, Fibromyalgia Syndrome, and Related Neural Network Disorders.*Binghamton, New York: Haworth Medical Press, 1996.
*This book is filled with valuable information about how the CFS/ME brain works, and how medications affect it, but you will need a background in biochemistry to make full use of it.*
“The Neuropharmacology of Chronic Fatigue Syndrome.” Jay Goldstein: *http://www.cfids-cab.org/cfs-inform/Optimists/goldstein98.html*(http://www.cfids-cab.org/cfs-inform/Optimists/goldstein98.html)
*In this article, Dr. Goldstein provides an in-depth discussion of diagnosis, tests, associated* *disorders, and neurological findings in CFS/ME patients. From these, Dr. Goldstein draws the conclusion that other than limbic encephalopathy there is no other no other mechanism that could create the constellation symptoms found in CFS/ME.*
---
## AMPLIGEN
\*
From: 'CHRONIC FATIGUE SYNDROME: A TREATMENT GUIDE, 2ND EDITION' http://www.cfstreatmentguide.com/chronic-fatigue-syndrome-a-treatment-guide-2nd-edition.html
PHARMACEUTICALS AND PRESCRIPTION DRUGS
Ampligen
Antibiotics
Anticonvulsants: Neurontin (g
abapentin), Gabitril (tiagabine) Lyrica (pregabalin)
Antidepressant Drugs: doxepin, amitriptyline, nortriptyline, desipramine, imipramine, trimipramine, clomipramine,
fluoxetine, sertraline, paroxetine, citalopram, excitalopram, bupropion, phenalzine, tranylcypromine,
trazadone, venlafaxine, duloxetine, mirtazapine
Antifungal Agents: Nystatin, Diflucan, Nizoral, Sporanox
Antihistamines: Benadryl (diphenhydramine), Claritin (loratadine), Allegra (fexofenadine), Zyrtec (cetirizine), Chlor\-
Trimeton (chlorpheniramine maleate), Atarax and Vistaril (hydroxyzine), Dramamine (meclizine), DiVertigo
Antiviral Agents: acyclovir, famcyclovir, amantadine, valacyclovir, valganciclovir
Artesunate
Benzodiazepines: clonazepam, diazepam, alprazolam
Beta Blockers: propanolol (Inderol), atenolol (Tenormin), labetalol (Normodyne), nebivolol (Bystolic)
Calcium Channel Blockers: Nicardipine, Nimodipine, Nifedipine, Verapamil
Central Nervous System Stimulants: Ritalin, Dexedrine, Lonamin, Provigil, Strattera
Cytotec (misoprostol)
Diamox (acetazolamide)
Epogen (Procrit)
Flexeril (cyclobenzaprine)
Florinef (fludrocortisone)
Gamma Globulin
GcMAF
Guaifenesin
H2 Blockers: Tagamet (cimetidine) and Zantac (ranitidine)
Hormones: Growth Hormone, Testosterone, Thyroid Hormones, Hydrocortisone
Hypnotics: Ambien, Lunesta, Rozerem, Xyrem
Kutapressin (see: Nexavir)
Midodrine
Naltrexone (LDN)
Nexavir (formerly Kutapressin)
Nitroglycerin
Oxytocin
Pain Relievers: Aspirin, NSAIDs, Tylenol, Aleve, Ultram, Narcotics
Pentoxifylline
Plaquenil
Pyridostigmine (Mestinon)
Questran (cholestyramine)
Rituximab
Transfer Factor
CHAPTER 5: NUTRITIONAL SUPPLEMENTS AND BOTANICALS
Introduction: Useful Resources
5-HTP
Alpha Ketoglutarate (AKG)
Alpha Lipoic Acid
Amino Acids: Carnitine, Glutamine, Lysine, Taurine
Antioxidants
Betaine HCl
Bioflavonoids: Grape seed extract, Pycnogenol, Quercetin
Butyric Acid (Butyrate)
Choline
CoQ10 (ubiquinone, ubiquinol)
D-Ribose
Digestive Enzymes
DHEA (dehydroepiandrosterone)
Essential Fatty Acids: Fish Oil, Flaxseed Oil, Evening Primrose Oil, Borage Seed Oil
FOS (fructooligosaccharides)
GABA (gamma aminobutyric acid)
Galantamine
Glucosamine Sulfate
Glutathione
Herbs: Aloe vera, Astragalus, Chamomile, Echinacea, Garlic, Ginger, Gingko, Ginseng, Goldenseal, Gotu kola, Kava,
Licorice, Lomatium, Milk Thistle, St. John's Wort, Uva ursi, Valerian
Histame
Inosine
Inositol
Malic Acid
Melatonin
Minerals: Calcium, Magnesium, Selenium, Colloidal Silver, Zinc
Monolaurin
Mushroom extracts: LEM (shiitake), Maitake, Cordyceps
NAC (N-acetylcysteine )
NADH (ENADA)
Piracetam
Probiotics
Royal Jelly
Sambucol
SAMe (S-Adenosyl methionine)
Vitamins:
Vitamin A, Beta-Carotene, Vitamin B12, Vitamin B6, Vitamin B Complex, Vitamin C, Vitamin D, Vitamin E and
Tocotrienols
Whey Products: Colostrom, Undenatured Whey, Probioplex
CHAPTER 6: ALTERNATIVE AND COMPLEMENTARY MEDICAL AND SUPPORTIVE THERAPIES
Acupressure
Acupuncture
Aroma Therapy
Bach Remedies
Bed Rest
Biofeedback
Chelation Therapy
Chiropractic
CBT (Cognitive Behavioral Therapy)
Exercise; GET (Graded Exercise Therapy)
Homeopathy
Hydrotherapy
Hypnosis
Massage:Craniosacral Massage, Lymphatic Drainage, Myofascial Release, Perrin Technique, Reflexology, Shiatsu
Meditation; Amygdala Retraining Program
Pacing
TENS (transcutaneous electrical nerve stimulation)
Visualization and Imagery
Yoga
COPING AND MANAGEMENT STRATEGIES
Introduction– Pacing Yourself
CHAPTER 7: STRESS REDUCTION AND ELIMINATION
CHAPTER 8: CLEANING UP: ELIMINATING TOXINS IN THE HOME
CHAPTER 9: FOOD AND DIET
\*
From: 'DRUG DATABASE' http://fmcfsme.com/drug_database.php
(for CFS/ME but includes FM)
A
Acai
acetaminophen
Acetyl-L-Carnitine
Actiq®
alprazolam
Ambien®
amitriptyline
amoxapine
Anafranil®
Anexsia®
Anolor®
Asian Ginseng
aspirin
Ativan®
atomoxetine
B
baclofen
Balacet®
Bancap®
bupropion
Buspar®
buspirone
Butrans Patch®
C
Capsaicin®
carbamazepine
carisoprodol
Carnitine
Celebrex®
celecoxib
Celexa®
chlordiazepoxide
citalopram
clonazepam
codeine
CoQ10
cyclobenzaprine
Cymbalta®
D
Darvocet®
Darvon®
Daypro®
Demerol®
desloratadine
desvenlafaxine
Desyrel®
DHEA®
diazepam
diclofenac
Dicloflex®
Dilaudid®
Dolophine®
doxepin
D-Ribose
duloxetine
E
Effexor®
Elavil®
Eldepryl®
Endep®
Endocet®
Eskalith®
estazolam
eszopiclone
etodolac
F
fentanyl
Fentora®
Feverfew®
fexofenadine
Fioricet®
Fiorinal®
Flebogamma®
Flexeril®
fluoxetine
flurazepam
fluvoxamine
G
gabapentin
Gammar-P I.V.®
ganciclovir
Garlic
Ginko
guaifenesin
H
halazepam
5-HTP
hydrocodone
hydromorphone
I
ibuprofen
imipramine
Imitrex®
Imovane®
isocarboxazid
J
K
Kadian®
Kava
ketamine
ketoprofen
Klonopin®
L
Lexapro®
Licorice Root
Lidocaine®
Lidoderm®
Lioresal®
Lodine®
lorazepam
Lorcet®
Lortab®
L-Theanine
Lunesta®
Lyrica®
M
Magnesium Malate
melatonin
mephobarbital
metaxalone
methadone
Methadose®
Methocarbamol
milnacipran
Mirapex®
mirtazapine
Mobic®
moclobemide
morphine
N
nabilone
NADH
Nalfon®
naltrexone
naproxen
Nardil®
nefazodone
Nembutal®
Neurontin®
nialamide
Niravam®
Norco®
Norflex®
Norpramin®
nortriptyline
Nucynta®
O
omeprazole
Orudis®
oxazepam
oxycodone
OxyContin®
P
paracetamol
paroxetine
Paxil®
Percocet®
Percodan®
Pexeva®
phenelzine
piroxicam
Plaquenil®
pregabalin
Propacet®
propoxyphene
Provigil®
Prozac®
R
reboxetine
Reglan®
Remeron®
Requip®
Restoril®
Rhodiola Rosea
risperidone
Robaxin®
rofecoxib
Rozerem®
S
SAM-e
Sarafem®
Savella®
Serax®
sertraline
Serzone®
Sinemet®
Skelaxin®
sodium oxybate
Soma®
Sonata®
St. John's Wort
sumatriptan
T
tiapreferic acid
tizanidine
Toradol®
tramadol
Trancot®
Tranxene SD®
tranylcypromine
trazodone
triazolam
Tylox®
U
Ultracet®
Ultram®
V
valganciclovir
Valium®
Valtrex®
Vanadom®
Vanatrip®
Vicodin®
Vitamin B-12
Vivactil®
Voltaren®
W
Wellbutrin®
Wygesic®
X
Xanax®
Xyrem®
Z
zaleplon
Zanaflex®
Zoloft®
zolpidem
zopiclone
Zostrix®
Zyban®
Zyrtec®
oman P, Carrillo-Trabalón F, Sánchez-Labraca N, Cañadas F, Estévez AF, Cardona D. Are probiotic treatments useful on fibromyalgia syndrome or chronic fatigue syndrome patients? A systematic review. Benef Microbes. 2018 Jun 15;9(4):603-611. PMID: 29695180
This study systematically reviewed the reported effect of probiotic treatments in patients diagnosed with FMS or CFS. The administration of Lactobacillus casei strain Shirota in CFS patients, over the course of 8 weeks, reduced anxiety scores. Additionally, the treatment with Bifidobacterium infantis 35624 in CFS patients, during the same period, reduced inflammatory biomarkers. The evidence about the usefulness of probiotics in CFS and FMS patients remains limited.
\*
Scheibenbogen C, Loebel M, Freitag H, Krueger A, Bauer S, Antelmann M, Doehner W, Scherbakov N, Heidecke H, Reinke P, Volk HD, Grabowski P. Immunoadsorption to remove ß2 adrenergic receptor antibodies in Chronic Fatigue Syndrome CFS/ME. PLoS One. 2018 Mar 15;13(3):e0193672. PMID: 29543914
Ten patients with post-infectious CFS/ME and elevated ß2 autoantibodies were treated with immunoadsorption with an IgG-binding column for 5 days. The researchers concluded that immunoadsorption can remove autoantibodies against ß2 adrenergic receptor and lead to clinical improvement. B cell phenotyping provides evidence for an effect of IA on memory B cell development.
\*
Corbitt M, Campagnolo N, Staines D, Marshall-Gradisnik S. A Systematic Review of Probiotic Interventions for Gastrointestinal Symptoms and Irritable Bowel Syndrome in Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (CFS/ME). Probiotics Antimicrob Proteins. 2018 Sep;10(3):466-477. PMID: 29464501
The aim of this study was to conduct a systematic literature review of gastrointestinal and irritable bowel symptoms in CFS/ME, along with any evidence for probiotics as treatment. The authors concluded that there is currently insufficient evidence for the use of probiotics in CFS/ME patients, despite probiotic interventions being useful in IBS.
\*
Wallis A, Ball M, Butt H, Lewis DP, McKechnie S, Paull P, Jaa-Kwee A, Bruck D. Open-label pilot for treatment targeting gut dysbiosis in myalgic encephalomyelitis/chronic fatigue syndrome: neuropsychological symptoms and sex comparisons. J Transl Med. 2018 Feb 6;16(1):24. PMID: 29409505
Participants in this study included 44 adult ME/CFS patients (27 females) from one specialist medical clinic with Streptococcus viable counts above 3.00 × 10^5 cfu/g (wet weight of faeces). The 4-week treatment protocol included alternate weeks of Erythromycin twice daily and probiotic (D-lactate free multistrain probiotic, 5 × 1010cfu twice daily). Large treatment effects were observed for the intention-to-treat sample with a reduction in Streptococcus viable count and improvement on several clinical outcomes including total symptoms, some sleep (less awakenings, greater efficiency and quality) and cognitive symptoms (attention, processing speed, cognitive flexibility, story memory and verbal fluency). This study’s results support the notion that specific microorganisms interact with some ME/CFS symptoms and offer promise for the therapeutic potential of targeting gut dysbiosis in this population.
\*
Rowe PC, Marden CL, Heinlein S, Edwards CC 2nd. Improvement of severe myalgic encephalomyelitis/chronic fatigue syndrome symptoms following surgical treatment of cervical spinal stenosis. J Transl Med. 2018 Feb 2;16(1):21. PMID: 29391028
The authors describe three consecutive patients with severe ME/CFS whose symptoms improved after recognition and surgical management of their cervical spinal stenosis. The prompt post-surgical restoration of more normal function suggests that cervical spine stenosis contributed to the pathogenesis of refractory ME/CFS and orthostatic symptoms.
\*
Gunn SR, Gunn GG, Mueller FW. Reversal of Refractory Ulcerative Colitis and Severe Chronic Fatigue SyndromeSymptoms Arising from Immune Disturbance in an HLA-DR/DQ Genetically Susceptible Individual with Multiple Biotoxin Exposures. Am J Case Rep. 2016 May 11;17:320-5. PMID: 27165859
A 25-year-old previously healthy male with new-onset refractory ulcerative colitis (RUC) and chronic fatigue syndrome (CFS) tested negative for autoimmune disease biomarkers. However, urine mycotoxin panel testing was positive for trichothecene group and air filter testing from the patient’s water-damaged rental house identified the toxic mold Stachybotrys chartarum. HLA-DR/DQ testing revealed a multisusceptible haplotype for development of chronic inflammation, and serum chronic inflammatory response syndrome (CIRS) biomarker testing was positive for highly elevated TGF-beta and a clinically undetectable level of vasoactive intestinal peptide (VIP). Following elimination of biotoxin exposures, VIP replacement therapy, dental extractions, and implementation of a mind body intervention-relaxation response (MBI-RR) program, the patient’s symptoms resolved. He is off medications, back to work, and resuming normal exercise.
\*
Alegre J, Rosés JM, Javierre C, Ruiz-Baqués A, Segundo MJ, de Sevilla TF. Nicotinamide adenine dinucleotide (NADH) in patients with chronic fatigue syndrome. Rev Clin Esp. 2010 Jun;210(6):284-8. PMID: 20447621
Administration of oral NADH was associated to a decrease in anxiety and maximum heart rate, after a stress test in patients with CFS.
\*
Rao AV, Bested AC, Beaulne TM, Katzman MA, Iorio C, Berardi JM, Logan AC. A randomized, double-blind, placebo-controlled pilot study of a probiotic in emotional symptoms of chronic fatigue syndrome. Gut Pathog. 2009 Mar 19;1(1):6. PMID: 19338686
CFS patients who received 24 billion colony forming units of Lactobacillus casei strain Shirota (LcS) daily for two months had a decrease in anxiety symptoms.
\*
Sullivan A, Nord CE, Evengård B. Effect of supplement with lactic-acid producing bacteria on fatigue and physical activity in patients with chronic fatigue syndrome. Nutr J. 2009 Jan 26;8:4. PMID: 19171024
Severely ill CFS patients were given the probiotics Lactobacillus paracasei ssp. paracasei F19, Lactobacillus acidophilus NCFB 1748 and Bifidobacterium lactis Bb12. The study reported neurocognitive functioning improvements, but no changes in fatigue or physical activity.
\*
Teitelbaum JE, Johnson C, St Cyr J. The use of D-ribose in chronic fatigue syndrome and fibromyalgia: a pilot study. J Altern Complement Med. 2006 Nov;12(9):857-62. PMID: 17109576
D-ribose was effective at improving CFS patients’ energy, sleep, mental clarity, pain intensity and overall feelings of well-being.
\*
Kodama M, Kodama T. The clinical course of interstitial pneumonia alias chronic fatigue syndrome under the control of megadose vitamin C infusion system with dehydroepiandrosterone-cortisol annex. Int J Mol Med. 2005 Jan;15(1):109-16. PMID: 15583836
A combination of high-dose intravenous Vitamin C and DHEA was effective at treating both CFS and interstitial pneumonia.
\*
Vermeulen RC, Scholte HR. Exploratory open label, randomized study of acetyl\- and propionylcarnitine in chronic fatigue syndrome. Psychosom Med. 2004 MarApr;66(2):276-82. PMID: 15039515
The authors compared 2 g/d acetyl-L-carnitine, 2 g/d propionyl-L-carnitine, and its combination in 3 groups of 30 CFS patients during 24 weeks. Acetylcarnitine and propionylcarnitine showed beneficial effect on fatigue and attention concentration. Less improvement was found by the combined treatment. Acetylcarnitine had main effect on mental fatigue and propionylcarnitine on general fatigue.
\*
Santaella ML, Font I, Disdier OM. Comparison of oral nicotinamide adenine dinucleotide (NADH) versus conventional therapy for chronic fatigue syndrome. P R Health Sci J. 2004 Jun;23(2):89-93. PMID: 15377055
NADH was effective in CFS for three months, but the positive results faded after that.
\*
Puri BK, Holmes J, Hamilton G. Eicosapentaenoic acid-rich essential fatty acid supplementation in chronic fatigue syndrome associated with symptom remission and structural brain changes. Int J Clin Pract. 2004 Mar;58(3):297-9. PMID: 15117099
Supplementation of an essential fatty acid rid in eicosapentaenoic acid (EPA) was followed by marked improvement in clinical condition after six weeks. Accurate quantification of the lateral ventricular volumes in the baseline and 16-week follow-up registered images of high-resolution magnetic resonance imaging structural scans showed that the treatment was accompanied by a marked reduction in the lateral ventricular volume during this period.
\*
Puri BK. The use of eicosapentaenoic acid in the treatment of chronic fatigue syndrome. Prostaglandins Leukot Essent Fatty Acids. 2004 Apr;70(4):399-401. PMID: 15041033
A series of patients with chronic fatigue syndrome were treated solely with a higheicosapentaenoic acid-containing essential fatty acid supplement. All showed improvement in their symptomatology within eight to 12 weeks.
\*
Cleare AJ, O’Keane V, Miell JP. Levels of DHEA and DHEAS and responses to CRH stimulation and hydrocortisone treatment in chronic fatigue syndrome. Psychoneuroendocrinology. 2004 Jul;29(6):724-32. PMID: 15110921
DHEA levels are raised in CFS and correlate with the degree of self-reported disability. Hydrocortisone therapy leads to a reduction in these levels towards normal, and an increased DHEA response to CRH, most marked in those who show a clinical response to this therapy.
\*
Cleare AJ, Miell J, Heap E, Sookdeo S, Young L, Malhi GS, O’Keane V. Hypothalamopituitary-adrenal axis dysfunction in chronic fatigue syndrome, and the effects of low-dose hydrocortisone therapy. J Clin Endocrinol Metab. 2001 Aug;86(8):3545-54. PMID: 11502777
The authors treat 32 patients with low-dose hydrocortisone and conclude that the improvement in fatigue seen in some patients with CFS during treatment is accompanied by a reversal of the blunted cortisol responses to human CRH.
\*
Forsyth LM, Preuss HG, MacDowell AL, Chiazze L Jr, Birkmayer GD, Bellanti JA. Therapeutic effects of oral NADH on the symptoms of patients with chronic fatigue syndrome. Ann Allergy Asthma Immunol. 1999 Feb;82(2):185-91. PMID: 10071523
31% of a group of CFS patients responded favorably to NADH, compared to 8% to a placebo.
\*
Warren G, McKendrick M, Peet M. The role of essential fatty acids in chronic fatigue syndrome. A case-controlled study of red-cell membrane essential fatty acids (EFA) and a placebo-controlled treatment study with high dose of EFA. Acta Neurol Scand. 1999 Feb;99(2):112-6. PMID: 10071170
Treatment with an essential fatty acid product (Efamol Marine) did not result in benefits compared to a placebo for CFS patients.
\*
Dykman KD, Tone C, Ford C, Dykman RA. The effects of nutritional supplements on the symptoms of fibromyalgia and chronic fatigue syndrome. Integr Physiol Behav Sci. 1998 Jan-Mar;33(1):61-71. PMID: 9594356
Nutritional supplements resulted in a reduction in initial symptom severity, with continued improvement in the period between initial assessment and the follow-up, in a group of CFS sufferers.
\*
See DM, Cimoch P, Chou S, Chang J, Tilles J. The in vitro immunomodulatory effects of glyconutrients on peripheral blood mononuclear cells of patients with chronic fatigue syndrome. Integr Physiol Behav Sci. 1998 Jul-Sep;33(3):280-7. PMID: 9829439
Addition of glyconutrient homogenate to PBMC from patients with CFS stimulated with phytohemagglutinin significantly increased the expression of each glycoprotein. The glyconutrient preparation significantly enhanced NK cell activity versus human herpes virus 6 (HHV-6)\-infected H9 cells in an 8 h 51Cr release assay compared to placebo for PBMC from patients with CFS (p< .01). Finally, apoptosis was significantly higher in patients with CFS. The percentage of apoptotic cells was significantly decreased in PBMC from patients with CFS that had been incubated for 48 h with glyconutrients.
\*
Plioplys AV, Plioplys S. Amantadine and L-carnitine treatment of Chronic Fatigue Syndrome. Neuropsychobiology. 1997;35(1):16-23. PMID: 9018019
In a group of 30 CFS patients, l-carnitine demonstrated significant improvements within 4-8 weeks. Amantadine, used to treat fatigue in MS, was poorly tolerated by CFS patients.
\*
De Vinci C, Levine PH, Pizza G, Fudenberg HH, Orens P, Pearson G, Viza D. Lessons from a pilot study of transfer factor in chronic fatigue syndrome. Biotherapy. 1996;9(1\- 3):87-90. PMID: 8993764
Of the 20 patients in the placebo-controlled trial of transfer factor, improvement was observed in 12 patients, generally within 3-6 weeks of beginning treatment.
\*
Ablashi DV, Levine PH, De Vinci C, Whitman JE Jr, Pizza G, Viza D. Use of anti HHV-6 transfer factor for the treatment of two patients with chronic fatigue syndrome (CFS). Two case reports. Biotherapy. 1996;9(1-3):81-6. PMID: 8993763
Specific Human Herpes virus-6 (HHV-6) transfer factor (TF) preparation, administered to two chronic fatigue syndrome patients, inhibited the HHV-6 infection. Prior to treatment, both patients exhibited an activated HHV-6 infection. TF treatment significantly improved the clinical manifestations of CFS in one patient who resumed normal duties within weeks, whereas no clinical improvement was observed in the second patient.
\*
Cox IM, Campbell MJ, Dowson D. Red blood cell magnesium and chronic fatigue syndrome. Lancet. 1991 Mar 30;337(8744):757-60. PMID: 1672392
A clinical trial showed that magnesium supplementation may be helpful in CFS.
\*
Behan PO, Behan WM, Horrobin D. Effect of high doses of essential fatty acids on the postviral fatigue syndrome. Acta Neurol Scand. 1990 Sep;82(3):209-16. PMID: 2270749
High doses of essential fatty acids containing linolenic, gamma-linolenic, eicosapentaenoic and docosahexaenoic acidswere helpful in CFS.
Increased levels of serum MAP-2 at 6-months correlate with improved outcome in survivors of severe traumatic brain injury
\*
Mailbag! My top 3 treatments for chronic fatigue syndrome | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2021/09/20/mailbag-my-top-3-treatments-for-chronic-fatigue-syndrome/)
Health Notes - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2002/01/01/health-notes-jan02/)
“Lazarus plant” ashwagandha brings energy levels back from the dead | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2014/12/26/ashwagandha/)
The Douglass Report February 2012 - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2012/02/01/the-douglass-report-february-2012/)
Study proves fibromyalgia is the real deal - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2009/01/16/study-proves-fibromyalgia-is-the-real-deal/)
Licorice whips your health problems - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2005/04/01/licorice-whips-health-problems/)
The sweet poison even the FDA didn’t want to approve - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2004/09/01/the-sweet-poison/)
Not soy fast - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2004/08/01/not-soy-fast/)
So you’re getting older who ever said you had to look or feel your age? DHEA may help you defy it - Daily Dose with Dr. Kevin Dobrzynski, DN | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2002/07/01/dhea-may-help-defy-age/)
Vitamin B12 cures DOZENS of health problems | Daily Dose with Dr. Kevin Dobrzynski, DN(https://drkevinsdailydose.com/2019/02/18/how-to-cure-any-disease/)
dmso cfs - Google Search(https://www.google.com/search?q=dmso+cfs&rlz=1C1CHBF_enUS864US864&oq=dmso+cfs&aqs=chrome..69i57j0i512j0i395i512l5j69i65.4021j1j7&sourceid=chrome&ie=UTF-8)
dmso arnica - Google Search(https://www.google.com/search?q=dmso+arnica&rlz=1C1CHBF_enUS864US864&oq=dmso+arnica&aqs=chrome..69i57j0i22i30l2.5284j1j7&sourceid=chrome&ie=UTF-8)
New folder
dmso cfs - Google Search(https://www.google.com/search?q=dmso+cfs&rlz=1C1CHBF_enUS975US975&oq=dmso&aqs=chrome.1.69i59l2j69i57j0i67j0i395i512l3j69i65.4102j1j7&sourceid=chrome&ie=UTF-8)
DMSO - Mycotoxins entering tissues? | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/dmso-mycotoxins-entering-tissues.52965/)
dmso arnica - Google Search(https://www.google.com/search?q=dmso+arnica&rlz=1C1CHBF_enUS975US975&oq=dmso&aqs=chrome.1.69i59l2j69i57j0i67j0i395i512l2j69i60l2.5296j1j7&sourceid=chrome&ie=UTF-8)
can exposure to black mold lead to cfs years later - Google Search(https://www.google.com/search?q=can+exposure+to+black+mold+lead+to+cfs+years+later&rlz=1C1CHBF_enUS975US975&oq=can+exposure+to+black+mold+lead+to+cfs+years+later&aqs=chrome..69i57j33i299.10753j1j7&sourceid=chrome&ie=UTF-8)
M.E., My Mold, & I… A Story of ME/CFS & Toxic Mold - Health Rising(https://www.healthrising.org/blog/2017/09/26/me-cfs-chronic-fatigue-toxic-mold-story-lissa/)
What Is Chronic Fatigue Syndrome? | RealTime Labs(https://realtimelab.com/blog/what-is-chronic-fatigue-syndrome/)
Toxic Mold Syndrome and How it Affects The Brain | Amen Clinics | Amen Clinics(https://www.amenclinics.com/blog/toxic-mold-syndrome-it-was-like-i-lost-my-personality/)
Can Mould & Mycotoxins Cause Chronic Fatigue Syndrome (CFS)?(https://www.alexmanos.co.uk/mould-mycotoxins-chronic-fatigue/)
Can Mold Cause Chronic Fatigue? - Fatigue To Flourish(https://fatiguetoflourish.com/chronic-fatigue-symptom-of-toxic-mold/)
Detection of Mycotoxins in Patients with Chronic Fatigue Syndrome(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3705282/)
Nootropics for chronic fatigue Syndrome - Google Search(https://www.google.com/search?q=Nootropics+for+chronic+fatigue+Syndrome&sxsrf=AOaemvIsp3UIiooMXWAwHqZVMWyWS583Vw:1637065920593&ei=wKSTYbLPI8Tc-gTkkrLQDg&start=10&sa=N&ved=2ahUKEwiyr67l8Zz0AhVErp4KHWSJDOoQ8NMDegUIARCvAw&biw=1072&bih=539&dpr=1.1)
LDN, Nootropics, Rituximab and Fads: Maija Haavisto on Treating Chronic Fatigue Syndrome and Fibromyalgia - Health Rising(https://www.healthrising.org/blog/2014/05/28/ldn-nootropics-rituximab-fads-maija-haavisto-treating-chronic-fatigue-syndrome/)
Chronic Fatigue Causes and How Nootropics Can Help | Thrivous®(https://thrivous.com/blogs/views/chronic-fatigue-causes-and-how-nootropics-can-help)
Nootropics for Chronic Fatigue? Well - Yes, but tread lightly(https://www.livecortex.com/nootropics-for-chronic-fatigue-well-yes-but-tread-lightly/)
Bacopa monnieri Supplement — Health Benefits, Dosage, Side Effects | Examine.com(https://examine.com/supplements/bacopa-monnieri/)
Supplements for Chronic Fatigue Syndrome?(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010273/)
cell membrane glycerolphospholipids cfs - Google Search(https://www.google.com/search?q=cell+membrane+glycerolphospholipids+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJTa_VAWQIMk_GUsAGG8rzt34ysjA%3A1637067268924&ei=BKqTYcT0N47c-gTPlYvgAg&oq=cell+membrane+glycerolphospholipids+cfs&gs_lcp=Cgdnd3Mtd2l6EAMyBwghEAoQoAEyBwghEAoQoAE6BwgAEEcQsAM6BggAEBYQHjoICAAQCBANEB46BQgAEIYDOgUIIRCrAkoECEEYAFCpCljHFGCpF2gBcAF4AIABqAGIAcIEkgEDMC40mAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjEhqbo9pz0AhUOrp4KHc_KAiwQ4dUDCA4&uact=5)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6941554/)
Nootropics for Fatigue: How to Use Supplements to Boost Your Energy - AZOTH | Peak-Productivity Nootropic Supplements(https://azothwise.com/resources/nootropics-for-fatigue/)
L-Alpha glyceryl phosphorylcholine "cfs" - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJOJ6QwsCEjaTTurem6TiUplPf8DQ:1637066500964&q=L-Alpha+glyceryl+phosphorylcholine+%22cfs%22&sa=X&ved=2ahUKEwiepI3685z0AhVDs54KHRrzDMgQ5t4CegQICBAB&biw=1072&bih=539&dpr=1.1)
14 Nootropics, aka Brain Enhancers, for Your Memory and More(https://www.healthline.com/health/nootropics-what-is-it-and-list-of-supplements)
The Best Nootropics for Energy and Motivation | FOCL(https://focl.com/blogs/learn/your-guide-to-nootropics-for-energy-and-motivation)
NADH – Nootropics Expert(https://nootropicsexpert.com/nadh/)
(1) Biomarker for chronic fatigue syndrome identified : Nootropics(https://www.reddit.com/r/Nootropics/comments/bl05dl/biomarker_for_chronic_fatigue_syndrome_identified/)
purinergic antagonists - Google Search(https://www.google.com/search?q=purinergic+antagonists&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
Sulbutiamine as a Treatment for Chronic Fatigue Syndrome » Corpina(https://corpina.com/sulbutiamine-treatment-chronic-fatigue-syndrome/)
Phenylpiracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Phenylpiracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBcQAQ&biw=1072&bih=539&dpr=1.1)
Piracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Piracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBkQAQ&biw=1072&bih=539&dpr=1.1)
Nimodipine CFS - Google Search(https://www.google.com/search?sxsrf=AOaemvKQL56w5GblA4d7JHMHUTCBU41BYg:1637065876173&q=Nimodipine+CFS&sa=X&ved=2ahUKEwilkZfQ8Zz0AhXNv54KHQ03AhUQ1QJ6BAghEAE&biw=1072&bih=539&dpr=1.1)
nimodipine use in me, jan 2014.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.actionforme.org.uk/assets/components/discuss/attachments/2/6193/nimodipine%20use%20in%20me,%20jan%202014.pdf)
When antibiotics turn toxic(https://www.nature.com/articles/d41586-018-03267-5)
purinergic antagonists chronic fatigue syndrome - Google Search(https://www.google.com/search?q=purinergic+antagonists+chronic+fatigue+syndrome&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJGlXWykhodQ42YFbXm8Ki_Q--V9A%3A1637066666812&ei=qqeTYfz6MI7W-wSelaqoDQ&oq=purinergic+antagonists+chronic+fat&gs_lcp=Cgdnd3Mtd2l6EAMYATIFCCEQoAEyBQghEKABOgcIIxCwAxAnOgQIIxAnOgUIIRCrAjoGCAAQFhAeSgQIQRgBUNIJWIFVYJpmaAlwAHgAgAFqiAGnCZIBBDEwLjOYAQCgAQHIAQHAAQE&sclient=gws-wiz)
New Tab(chrome://newtab/)
Sci-Hub(https://sci-hubtw.hkvisa.net/)
neurotrophic cfs - Google Search(https://www.google.com/search?q=neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotrophic+cfs&aqs=chrome..69i57j69i65.12939j1j7&sourceid=chrome&ie=UTF-8)
neurotropic cfs - Google Search(https://www.google.com/search?q=neurotropic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotropic+cfs&aqs=chrome..69i57.13372j1j7&sourceid=chrome&ie=UTF-8)
post stroke neurotrophic neurorehabilitation medicine textbook - Google Search(https://www.google.com/search?rlz=1C1TSNO_enUS609US609&biw=1290&bih=858&ei=uKNsXKD1K8Lk9APZ5b-gDg&q=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&oq=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&gs_l=psy-ab.3...143106.154126..158615...1.0..0.134.1464.6j8......0....1..gws-wiz.......0i71j35i304i39j33i10.oOyfywRfLLs)
peptide modulation. Some neurons, given neurotrophic factors show regrowth/repair cfs - Google Search(https://www.google.com/search?q=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg%3A1637068069900&ei=Ja2TYciqNsf9-gT67I0I&oq=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAgjECdKBAhBGABQoyJYzTFguzVoAXACeACAAXeIAeMCkgEDMC4zmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ4dUDCA4&uact=5)
Frontiers | The Influence of Neuron-Extrinsic Factors and Aging on Injury Progression and Axonal Repair in the Central Nervous System | Cell and Developmental Biology(https://www.frontiersin.org/articles/10.3389/fcell.2020.00190/full)
Neurotrophin medication - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg:1637068069900&q=Neurotrophin+medication&sa=X&ved=2ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ1QJ6BAgoEAE&biw=1072&bih=539&dpr=1.1)
Neurotrophic drugs cfs - Google Search(https://www.google.com/search?q=Neurotrophic+drugs+cfs&rlz=1C1CHBF_enUS864US864&biw=1072&bih=539&sxsrf=AOaemvKdXB8DB9QDY7MneMEdqqGiXpNzAw%3A1637068176384&ei=kK2TYb7zFsHm-gSUsabwDQ&oq=Neurotrophic+drugs+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6BQgAEIAEOggIABAWEAoQHjoFCCEQoAE6BQghEKsCSgQIQRgAUOoJWJMXYLQbaAFwAngAgAGHAYgB0gOSAQMwLjSYAQCgAQHIAQnAAQE&sclient=gws-wiz&ved=0ahUKEwi--4CZ-pz0AhVBs54KHZSYCd4Q4dUDCA4&uact=5)
"Neurotrophic" drugs cfs treatment - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJ416h00H5WUgPDewpXrt47-wOeTw:1637068281438&q=%22Neurotrophic%22+drugs+cfs+treatment&sa=X&ved=2ahUKEwjQ2ozL-pz0AhWP6p4KHfmsA08Q5t4CegQIChAB&biw=1072&bih=539&dpr=1.1)
Postulated vasoactive neuropeptide immunopathology affecting the blood-brain/blood-spinal barrier in certain neuropsychiatric fatigue-related conditions: A role for phosphodiesterase inhibitors in treatment? - PubMed(https://pubmed.ncbi.nlm.nih.gov/19557103/)
Frontiers | Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome | Frontiers in Systems Neuroscience(https://www.frontiersin.org/articles/10.3389/fnsys.2021.698240/full)
A Novel Nutriceutical Treatment of Myalgic Encephalitis/Chronic Fatigue Syndrome (ME/CFS): “What it is and what it is not” - a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.longdom.org/open-access/a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf)
nutraceutical cfs - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvI5tGny2KtFiuTU-yYbuCUN-JdfWQ:1637068508214&q=nutraceutical+cfs&spell=1&sa=X&ved=2ahUKEwiPkJ63-5z0AhWJrp4KHV8OB60QBSgAegQIARA0&biw=1072&bih=539&dpr=1.1)
nutraceutical neurotrophin - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophin&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro&aqs=chrome.1.69i57j33i160l4.20328j1j7&sourceid=chrome&ie=UTF-8)
nutraceutical neurotrophic cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotrophic+cfs&aqs=chrome..69i57.49667j1j7&sourceid=chrome&ie=UTF-8)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvIckRIy2NrjMpHNTWDR5zbOk_IICA:1637068696696&ei=mK-TYfj3KcPY-wSZh7b4CQ&start=10&sa=N&ved=2ahUKEwj4o46R_Jz0AhVD7J4KHZmDDZ8Q8NMDegQIARBN&biw=1072&bih=539&dpr=1.1)
New folder
"Neurotrophic" drugs cfs treatment - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJ416h00H5WUgPDewpXrt47-wOeTw:1637068281438&q=%22Neurotrophic%22+drugs+cfs+treatment&sa=X&ved=2ahUKEwjQ2ozL-pz0AhWP6p4KHfmsA08Q5t4CegQIChAB&biw=1072&bih=539&dpr=1.1)
(PDF) A Randomized Controlled Trial of Intranasal Neuropeptide Y in Patients With Major Depressive Disorder(https://www.researchgate.net/publication/345721621_A_Randomized_Controlled_Trial_of_Intranasal_Neuropeptide_Y_in_Patients_With_Major_Depressive_Disorder)
A Combination of Three Repurposed Drugs Administered at Reperfusion as a Promising Therapy for Postischemic Brain Injury | Request PDF(https://www.researchgate.net/publication/317671530_A_Combination_of_Three_Repurposed_Drugs_Administered_at_Reperfusion_as_a_Promising_Therapy_for_Postischemic_Brain_Injury)
A Novel Neuroinflammatory Paradigm for Chronic Fatigue Syndrome (ME/CFS) - Health Rising(https://www.healthrising.org/blog/2020/05/27/neuroinflammatory-paradigm-chronic-fatigue-me-cfs/)
Better Thinking for Chronic Fatigue Syndrome and Fibromyalgia: the Nootropics - the "Smart Drugs" - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/nootropics/)
A Novel Nutriceutical Treatment of Myalgic Encephalitis/Chronic Fatigue Syndrome (ME/CFS): “What it is and what it is not” - a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.longdom.org/open-access/a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf)
Aneurysmal Subarachnoid Hemorrhage Trial in Xi'an (Magnesium-Rich Artificial Cerebrospinal Fluid) | Clincosm(https://www.clincosm.com/trial/aneurysmal-subarachnoid-hemorrhage-xian-magnesium-rich-artificial)
Chronic Fatigue Causes and How Nootropics Can Help | Thrivous®(https://thrivous.com/blogs/views/chronic-fatigue-causes-and-how-nootropics-can-help)
Bookmarks(chrome://bookmarks/?q=Drugs)
Bacopa monnieri Supplement — Health Benefits, Dosage, Side Effects | Examine.com(https://examine.com/supplements/bacopa-monnieri/)
Can the Drugs Namenda and Aricept Help After Brain Injury? | BrainLine(https://www.brainline.org/qa/can-drugs-namenda-and-aricept-help-after-brain-injury)
cell membrane glycerolphospholipids cfs - Google Search(https://www.google.com/search?q=cell+membrane+glycerolphospholipids+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJTa_VAWQIMk_GUsAGG8rzt34ysjA%3A1637067268924&ei=BKqTYcT0N47c-gTPlYvgAg&oq=cell+membrane+glycerolphospholipids+cfs&gs_lcp=Cgdnd3Mtd2l6EAMyBwghEAoQoAEyBwghEAoQoAE6BwgAEEcQsAM6BggAEBYQHjoICAAQCBANEB46BQgAEIYDOgUIIRCrAkoECEEYAFCpCljHFGCpF2gBcAF4AIABqAGIAcIEkgEDMC40mAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjEhqbo9pz0AhUOrp4KHc_KAiwQ4dUDCA4&uact=5)
cfs treatment neuropeptide - Google Search(https://www.google.com/search?q=cfs+treatment+neuropeptide&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJbvoEdcWpODz94rwSdORVrod567Q:1637068421629&ei=ha6TYbbZJcf2-gT5oaSQCA&start=10&sa=N&ved=2ahUKEwj2r_mN-5z0AhVHu54KHfkQCYIQ8NMDegQIARBM&biw=1072&bih=539&dpr=1.1)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer - PubMed(https://pubmed.ncbi.nlm.nih.gov/32309576/)
Piracetam + Choline - Google Search(https://www.google.com/search?q=Piracetam+%2B+Choline&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
complete list drugs cfs forum "hip" - Google Search(https://www.google.com/search?q=complete+list+drugs+cfs+forum+%22hip%22&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvK40MmRvXyotJtfv_YzA2nGTYyotA%3A1637080344723&ei=GN2TYea3K8rm-gTEtpnQBA&oq=complete+list+drugs+cfs+forum+%22hip%22&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAghEApKBAhBGABQlAxYuBJgyhhoAXACeACAAaUCiAGeBpIBBTMuMi4xmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjmo6nDp530AhVKs54KHURbBkoQ4dUDCA4&uact=5)
Supplements for Chronic Fatigue Syndrome?(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010273/)
Drugs - Health Rising(https://www.healthrising.org/blog/category/treatment/drugs/)
Drugs and Supplements For Chronic Fatigue Syndrome (ME/CFS) and/or Fibromyalgia - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/)
Health Rising - Finding Answers for Fibromyalgia and Chronic Fatigue Syndrome (ME/CFS)(https://www.healthrising.org/)
intranasal neuropeptide cfs - Google Search(https://www.google.com/search?q=intranasal+neuropeptide+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvLlnIUIPjwVjbho8NH20SKVnt5oWA:1637079556777&ei=BNqTYczwLoz4-gTM8Y2ABg&start=10&sa=N&ved=2ahUKEwjMgs3LpJ30AhUMvJ4KHcx4A2AQ8NMDegQIARBM&biw=1072&bih=539&dpr=1.1)
Intranasal Neuropeptide Y Blunts Lipopolysaccharide-Evoked Sickness Behavior but Not the Immune Response in Mice(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6985076/)
LDN, Nootropics, Rituximab and Fads: Maija Haavisto on Treating Chronic Fatigue Syndrome and Fibromyalgia - Health Rising(https://www.healthrising.org/blog/2014/05/28/ldn-nootropics-rituximab-fads-maija-haavisto-treating-chronic-fatigue-syndrome/)
14 Nootropics, aka Brain Enhancers, for Your Memory and More(https://www.healthline.com/health/nootropics-what-is-it-and-list-of-supplements)
Mitochondrial Modifying Nutrients in Treating Chronic Fatigue Syndrome: A 16-week Open-Label Pilot Study | Request PDF(https://www.researchgate.net/publication/321122761_Mitochondrial_Modifying_Nutrients_in_Treating_Chronic_Fatigue_Syndrome_A_16-week_Open-Label_Pilot_Study)
The Best Nootropics for Energy and Motivation | FOCL(https://focl.com/blogs/learn/your-guide-to-nootropics-for-energy-and-motivation)
neurotrophic cfs - Google Search(https://www.google.com/search?q=neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotrophic+cfs&aqs=chrome..69i57j69i65.12939j1j7&sourceid=chrome&ie=UTF-8)
NADH – Nootropics Expert(https://nootropicsexpert.com/nadh/)
Neurotrophic Factors - an overview | ScienceDirect Topics(https://www.sciencedirect.com/topics/neuroscience/neurotrophic-factors)
(1) Biomarker for chronic fatigue syndrome identified : Nootropics(https://www.reddit.com/r/Nootropics/comments/bl05dl/biomarker_for_chronic_fatigue_syndrome_identified/)
Neurotrophin medication - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg:1637068069900&q=Neurotrophin+medication&sa=X&ved=2ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ1QJ6BAgoEAE&biw=1072&bih=539&dpr=1.1)
purinergic antagonists - Google Search(https://www.google.com/search?q=purinergic+antagonists&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
New Tab(chrome://newtab/)
Treatment of chronic fatigue syndrome with 5-HT3 receptor antagonists - preliminary results: Scandinavian Journal of Rheumatology: Vol 29, No 113(https://www.tandfonline.com/doi/abs/10.1080/030097400750001851-1)
Nimodipine CFS - Google Search(https://www.google.com/search?sxsrf=AOaemvKQL56w5GblA4d7JHMHUTCBU41BYg:1637065876173&q=Nimodipine+CFS&sa=X&ved=2ahUKEwilkZfQ8Zz0AhXNv54KHQ03AhUQ1QJ6BAghEAE&biw=1072&bih=539&dpr=1.1)
(1) Anyone had any success dealing with chronic fatigue syndrome? : Nootropics(https://www.reddit.com/r/Nootropics/comments/6mjzp7/anyone_had_any_success_dealing_with_chronic/)
Nootropics for chronic fatigue Syndrome - Google Search(https://www.google.com/search?q=Nootropics+for+chronic+fatigue+Syndrome&sxsrf=AOaemvIsp3UIiooMXWAwHqZVMWyWS583Vw:1637065920593&ei=wKSTYbLPI8Tc-gTkkrLQDg&start=10&sa=N&ved=2ahUKEwiyr67l8Zz0AhVErp4KHWSJDOoQ8NMDegUIARCvAw&biw=1072&bih=539&dpr=1.1)
Sulbutiamine as a Treatment for Chronic Fatigue Syndrome » Corpina(https://corpina.com/sulbutiamine-treatment-chronic-fatigue-syndrome/)
Nootropics for Chronic Fatigue? Well - Yes, but tread lightly(https://www.livecortex.com/nootropics-for-chronic-fatigue-well-yes-but-tread-lightly/)
Nootropics for Fatigue: How to Use Supplements to Boost Your Energy - AZOTH | Peak-Productivity Nootropic Supplements(https://azothwise.com/resources/nootropics-for-fatigue/)
nutraceutical cfs - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvI5tGny2KtFiuTU-yYbuCUN-JdfWQ:1637068508214&q=nutraceutical+cfs&spell=1&sa=X&ved=2ahUKEwiPkJ63-5z0AhWJrp4KHV8OB60QBSgAegQIARA0&biw=1072&bih=539&dpr=1.1)
nutraceutical neurotrophic cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotrophic+cfs&aqs=chrome..69i57.49667j1j7&sourceid=chrome&ie=UTF-8)
nimodipine use in me, jan 2014.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.actionforme.org.uk/assets/components/discuss/attachments/2/6193/nimodipine%20use%20in%20me,%20jan%202014.pdf)
peptide modulation. Some neurons, given neurotrophic factors show regrowth/repair cfs - Google Search(https://www.google.com/search?q=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg%3A1637068069900&ei=Ja2TYciqNsf9-gT67I0I&oq=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAgjECdKBAhBGABQoyJYzTFguzVoAXACeACAAXeIAeMCkgEDMC4zmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ4dUDCA4&uact=5)
Phenylpiracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Phenylpiracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBcQAQ&biw=1072&bih=539&dpr=1.1)
When antibiotics turn toxic(https://www.nature.com/articles/d41586-018-03267-5)
Piracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Piracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBkQAQ&biw=1072&bih=539&dpr=1.1)
purinergic antagonists chronic fatigue syndrome - Google Search(https://www.google.com/search?q=purinergic+antagonists+chronic+fatigue+syndrome&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJGlXWykhodQ42YFbXm8Ki_Q--V9A%3A1637066666812&ei=qqeTYfz6MI7W-wSelaqoDQ&oq=purinergic+antagonists+chronic+fat&gs_lcp=Cgdnd3Mtd2l6EAMYATIFCCEQoAEyBQghEKABOgcIIxCwAxAnOgQIIxAnOgUIIRCrAjoGCAAQFhAeSgQIQRgBUNIJWIFVYJpmaAlwAHgAgAFqiAGnCZIBBDEwLjOYAQCgAQHIAQHAAQE&sclient=gws-wiz)
post stroke neurotrophic neurorehabilitation medicine textbook - Google Search(https://www.google.com/search?rlz=1C1TSNO_enUS609US609&biw=1290&bih=858&ei=uKNsXKD1K8Lk9APZ5b-gDg&q=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&oq=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&gs_l=psy-ab.3...143106.154126..158615...1.0..0.134.1464.6j8......0....1..gws-wiz.......0i71j35i304i39j33i10.oOyfywRfLLs)
New Tab(chrome://newtab/)
Tetramethoxyluteolin for the Treatment of Neurodegenerative Diseases - PubMed(https://pubmed.ncbi.nlm.nih.gov/30451113/)
Thesis - Personalized nootropic formulas to activate every kind of brain.(https://i.takethesis.com/google/?utm_campaign=14954151256&utm_source=google&utm_medium=cpc&utm_content=558937427235&utm_term=nootropic%20supplements&adgroupid=127211547054&gclid=Cj0KCQiAys2MBhDOARIsAFf1D1e4ewslWTbNnwb7spk_E_oAzFC8HDBoPuIIkzNBW3TQgkepj3trJtsaAlgxEALw_wcB)
Sci-Hub(https://sci-hubtw.hkvisa.net/)
Treatment | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums(https://www.healthrising.org/forums/forums/treatment.11/)
neurotropic cfs - Google Search(https://www.google.com/search?q=neurotropic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotropic+cfs&aqs=chrome..69i57.13372j1j7&sourceid=chrome&ie=UTF-8)
neurorehabilitation drug cfs - Google Search(https://www.google.com/search?q=neurorehabilitation+drug+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJG8sJskCkLEf1K4T9tnp6mlZTGZg%3A1637067605716&ei=VauTYaGOK-LE0PEP_MytsAg&oq=neurorehabilitation+drug+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6DQgAEIAEEIcCEMkDEBQ6BQgAEIAEOgQIABBDOgsILhCABBDHARCvAToFCC4QgAQ6BggAEBYQHjoICAAQFhAKEB46BQghEKABOgUIIRCrAkoECEEYAFDWCFiGKGDQK2gBcAJ4AIABigKIAfYJkgEFMC44LjGYAQCgAQHIAQrAAQE&sclient=gws-wiz&ved=0ahUKEwjhjPKI-Jz0AhViIjQIHXxmC4YQ4dUDCA4&uact=5)
Neurotrophic Peptide - an overview | ScienceDirect Topics(https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/neurotrophic-peptide)
Frontiers | The Influence of Neuron-Extrinsic Factors and Aging on Injury Progression and Axonal Repair in the Central Nervous System | Cell and Developmental Biology(https://www.frontiersin.org/articles/10.3389/fcell.2020.00190/full)
Neurotrophic drugs cfs - Google Search(https://www.google.com/search?q=Neurotrophic+drugs+cfs&rlz=1C1CHBF_enUS864US864&biw=1072&bih=539&sxsrf=AOaemvKdXB8DB9QDY7MneMEdqqGiXpNzAw%3A1637068176384&ei=kK2TYb7zFsHm-gSUsabwDQ&oq=Neurotrophic+drugs+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6BQgAEIAEOggIABAWEAoQHjoFCCEQoAE6BQghEKsCSgQIQRgAUOoJWJMXYLQbaAFwAngAgAGHAYgB0gOSAQMwLjSYAQCgAQHIAQnAAQE&sclient=gws-wiz&ved=0ahUKEwi--4CZ-pz0AhVBs54KHZSYCd4Q4dUDCA4&uact=5)
Postulated vasoactive neuropeptide immunopathology affecting the blood-brain/blood-spinal barrier in certain neuropsychiatric fatigue-related conditions: A role for phosphodiesterase inhibitors in treatment? - PubMed(https://pubmed.ncbi.nlm.nih.gov/19557103/)
Frontiers | Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome | Frontiers in Systems Neuroscience(https://www.frontiersin.org/articles/10.3389/fnsys.2021.698240/full)
nutraceutical neurotrophin - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophin&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro&aqs=chrome.1.69i57j33i160l4.20328j1j7&sourceid=chrome&ie=UTF-8)
Fibromyalgia Causes And Treatment With Guaifenesin, Amitriptyline, Kratom, Flexeril, And Others. -(https://www.sunshinentc.com/fibromyalgia-causes-and-treatment-with-guaifenesin-amitriptyline-kratom-flexeril-and-others/)
A systematic review of nutraceutical interventions for mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome | Journal of Translational Medicine | Full Text(https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-021-02742-4)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvIckRIy2NrjMpHNTWDR5zbOk_IICA:1637068696696&ei=mK-TYfj3KcPY-wSZh7b4CQ&start=10&sa=N&ved=2ahUKEwj4o46R_Jz0AhVD7J4KHZmDDZ8Q8NMDegQIARBN&biw=1072&bih=539&dpr=1.1)
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Metabolic Disease or Disturbed Homeostasis due to Focal Inflammation in the Hypothalamus? - ME-CFS-JPET-9-2018.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/mastcellmaster.com/documents/2018-09/ME-CFS-JPET-9-2018.pdf)
neuropeptide Y - Clincosm(https://www.clincosm.com/search?q=neuropeptide%20Y)
Peptidergic Drugs for Treatment of Traumatic Brain Injury(https://www.medscape.com/viewarticle/780437_5)
Supplements and Drugs That Reduce or Prevent PEM (Post-Exertional Malaise) | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/supplements-and-drugs-that-reduce-or-prevent-pem-post-exertional-malaise.48438/)
ocd
4 Common OCD Alternative Treatments and Therapies(https://www.verywellmind.com/new-treatments-for-ocd-2510610)
Treatments for Obsessive-Compulsive Disorder(https://www.verywellmind.com/ocd-treatments-2510626)
Herbal Remedies for OCD and Anxiety Disorders(https://www.verywellmind.com/herbal-remedies-for-ocd-2510631)
New Multisensory Therapy as an Alternative for Treatment of OCD - Psious(https://psious.com/multisensory-therapy-alternative-treatment-of-ocd/)
OCD Alternative Treatments - Promises P.A.T.H. Programs(https://www.promises.com/addiction-blog/ocd-alternative-treatments/)
Alternative Therapies for OCD | Psychology Today(https://www.psychologytoday.com/us/blog/natural-standard/201205/alternative-therapies-ocd)
Can OCD Be Treated Without Medication? OCD Medication and Treatment(https://www.treatmyocd.com/blog/can-ocd-be-treated-without-medication)
muschealth.org(https://muschealth.org/patients-visitors/about-us/2020-year-in-review/new-ocd-treatment-option)
Promising new nutrient treatment gives hope to OCD sufferers - Scimex(https://www.scimex.org/newsfeed/promising-new-nutrient-treatment-gives-hope-to-ocd-sufferers)
root canal chronic fatigue syndrome - Google Search(https://www.google.com/search?q=root+canal+chronic+fatigue+syndrome&oq=root+canal+chronic+fatigue&aqs=chrome.1.69i57j0i22i30l4.16182j0j8&client=tablet-android-verizon&sourceid=chrome-mobile&ie=UTF-8)
You searched for CHRONIc fatigue - ICNR(https://icnr.com/?s=CHRONIc+fatigue)
Is a Hidden Infection Causing Your Chronic Fatigue?(https://www.jillcarnahan.com/2016/05/07/hidden-infection-causing-fatigue/)
Chronic Fatigue - Kelatox(https://www.kelatox.com/chronic-fatigue/)
Drug can reverse hyperactivity induced by parasitic infection -- ScienceDaily(https://www.sciencedaily.com/releases/2019/04/190430141627.htm)
Systems analysis points to links between Toxoplasma infection and common brain diseases -- ScienceDaily(https://www.sciencedaily.com/releases/2017/09/170913084443.htm)
Parasite makes quick exit when researchers remove the handbrake -- ScienceDaily(https://www.sciencedaily.com/releases/2018/09/180924144049.htm)
pyrimethamine combined with sulfadiazine - Google Search(https://www.google.com/search?q=pyrimethamine+combined+with+sulfadiazine&client=tablet-android-verizon&sourceid=chrome-mobile&ie=UTF-8)
International OCD Foundation | Medications for OCD(https://iocdf.org/about-ocd/ocd-treatment/meds/)
Medication for OCD | OCD-UK(https://www.ocduk.org/overcoming-ocd/medication/)
Obsessive-compulsive disorder (OCD) - Diagnosis and treatment - Mayo Clinic(https://www.mayoclinic.org/diseases-conditions/obsessive-compulsive-disorder/diagnosis-treatment/drc-20354438)
New folder
Erythroprotein cfs - Google Search(https://www.google.com/search?q=Erythroprotein+cfs&rlz=1C1CHBF_enUS975US975&oq=Erythroprotein+cfs&aqs=chrome..69i57j33i10i160.1741j1j7&sourceid=chrome&ie=UTF-8)
Autonomic function and serum erythropoietin levels in chronic fatigue syndrome - ScienceDirect(https://www.sciencedirect.com/science/article/abs/pii/S0022399903005439)
Autonomic function and serum erythropoietin levels in chronic fatigue syndrome - PubMed(https://pubmed.ncbi.nlm.nih.gov/15016575/)
Erythropoietin (Procrit) | Myalgic Encephalomyelitis / Chronic Fatigue Syndrome (ME/CFS)(https://phoenixrising.me/myalgic-encephalomyelitis-chronic-fatigue-syndrome-mecfs-treatments/orthostatic-intolerance/treating-orthostatic-intolerance/treating-chronic-fatigue-syndrome-mecfs-erythropoietin-and-low-blood-volume/)
Scientists Find Hormonal Deficit in Chronic Fatigue Sufferers - The New York Times(https://www.nytimes.com/1991/12/02/us/scientists-find-hormonal-deficit-in-chronic-fatigue-sufferers.html)
Erythropoietin | You and Your Hormones from the Society for Endocrinology(https://www.yourhormones.info/hormones/erythropoietin/)
Chronic Fatigue Diet: 12 Hacks(https://www.healthline.com/health/diet-hacks-to-reduce-chronic-fatigue#6.-Limit-your-caffeine-intake)
What Supplements Should I Take for Chronic Fatigue?(https://wthn.com/blogs/wthnside-out/what-supplements-should-i-take-for-chronic-fatigue)
Nutrivy® | #1 UK Health Supplements(https://www.nutrivy.co.uk/)
Chronic Fatigue Syndrome Patients Benefit from CoQ10(https://www.pharmanord.com/news/chronic-fatigue-syndrome-patients-benefit-from-coq10)
Magnesium Malate: Benefits, Side Effects, Dosage, and Interactions(https://www.verywellhealth.com/magnesium-malate-fibromyalgia-chronic-fatigue-715798)
NAD vs NAD+ vs NADH - What’s the difference? | Tru Niagen®(https://www.truniagen.com/blog/nad-vs-nad-vs-nadh-whats-the-difference/)
Treatment of CFS Patients with low MSH and Elevated C4a using Low Dose Erythropoietin(https://www.survivingmold.com/store1/presentations/treatment-of-cfs-patients-with-low-msh-and-elevated-c4a-using-low-dose-erythropoietin)
Testing - SelfHacked(https://selfhacked.com/testing/)
Organic Acid Test (OAT): Amino Acid Metabolites - SelfHacked(https://selfhacked.com/blog/oat-amino-acid-metabolites/)
What is Sulforaphane? + Foods (Kale, Broccoli Sprouts) - SelfHacked(https://selfhacked.com/blog/sulforaphane-foods/)
ACTH Test: High & Low Levels, Normal Range + Benefits - SelfHacked(https://selfhacked.com/blog/acth/)
Albumin: Function & Associated Diseases - SelfHacked(https://selfhacked.com/blog/albumin/)
High Alkaline Phosphatase Symptoms & How to Reduce It - SelfHacked(https://selfhacked.com/blog/alkaline-phosphatase/)
Iron Lab Tests, Deficiency & Overload - SelfHacked(https://selfhacked.com/blog/iron-balance-blood-test-iron-deficiency-anemia-overload/)
What is Androstenedione? Tests, Supplements, Side Effects - SelfHacked(https://selfhacked.com/blog/androstenedione/)
Posts - SelfHacked(https://selfhacked.com/posts/)
SelfDecode Coupon - SelfHacked(https://selfhacked.com/blog/promo-code/)
SelfDecode Review: Upload Your Raw DNA Data and Get a Health Analysis - SelfHacked(https://selfhacked.com/blog/selfdecode-review-dna-analysis/)
9 Labs to Check Your Immune System Health - SelfHacked(https://selfhacked.com/blog/labs-immune-system-health/)
OCD Treatment: Medication & Complementary Approaches - SelfHacked(https://selfhacked.com/blog/ocd-treatment-medication-complementary-approaches/)
“Acetylcholine Deficiency” & Factors that Increase Levels - SelfHacked(https://selfhacked.com/blog/acetylcholine-deficiency-increase-levels/)
Low & High Sedimentation Rate + How to Lower Inflammation - SelfHacked(https://selfhacked.com/blog/sedimentation-rate-low-high/)
Low Chloride Levels (Hypochloremia) Symptoms & Causes - SelfHacked(https://selfhacked.com/blog/low-chloride-levels-hypochloremia/)
L-DOPA & Sinemet (Carbidopa-Levodopa) Side Effects - SelfHacked(https://selfhacked.com/blog/carbidopa-levodopa-sinemet-side-effects/)
Mitochondrial Diseases & Mitochondrial Dysfunction - SelfHacked(https://selfhacked.com/blog/mitochondrial-dysfunction-disease/)
Racetams & Nootropic Drugs: Does the Limitless Pill Exist? - SelfHacked(https://selfhacked.com/blog/nootropics-limitless-pill/)
About page - SelfDecode(https://selfdecode.com/en/about/?seg_id=01FKPK3W4RRZ0TSNV2X405FC1M.2704.1636806621217)
Home Page - SelfDecode(https://selfdecode.com/?seg_id=01FKPK3W4RRZ0TSNV2X405FC1M.2704.1636806621217)
Lab Test Analyzer(https://www.labtestanalyzer.com/)
Fatigue: 45+ Tips To Help You Fight It - SelfHacked(https://selfhacked.com/blog/fatigue-45-tips-to-help-you-fight-it/)
self hacked tests - Google Search(https://www.google.com/search?q=self+hacked+tests&rlz=1C1CHBF_enUS975US975&oq=self&aqs=chrome.1.69i60j69i59j46i199i395i424i465i466i512j35i39i395j69i60j69i65l3.2039j1j7&sourceid=chrome&ie=UTF-8)
Selfhacked nootropics - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS975US975&sxsrf=AOaemvJviUf-9nxVoUWhKCO24RWCRZaPVw:1636806613722&q=Selfhacked+nootropics&sa=X&ved=2ahUKEwiwhpvmq5X0AhVUqZ4KHYxPDzcQ1QJ6BAg1EAE&cshid=1636806776498974&biw=1678&bih=911&dpr=0.9)
10 Natural Nootropic Supplements that May Improve Memory - SelfHacked(https://selfhacked.com/blog/nootropics-top-ways-improve-protect-memory/)
Sulforaphane cfs - Google Search(https://www.google.com/search?q=Sulforaphane+cfs&rlz=1C1CHBF_enUS975US975&oq=Sulforaphane+cfs&aqs=chrome..69i57.1991j1j7&sourceid=chrome&ie=UTF-8)
The Integrative Role of Sulforaphane in Preventing Inflammation, Oxidative Stress and Fatigue: A Review of a Potential Protective Phytochemical(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7346151/)
Dr COURTNEY CRAIG — Diet & Nutrition for Chronic Fatigue & Fibromyalgia(https://www.drcourtneycraig.com/blog/2019/4/11/sulforaphane-broccolis-secret-weapon)
Demystifying Chronic Fatigue Syndrome/Myalgic Encephalomyelitis - A Systematic Review(https://clinmedjournals.org/articles/jmdt/journal-of-musculoskeletal-disorders-and-treatment-jmdt-7-090.php?jid=jmdt)
New folder
dmso cfs - Google Search(https://www.google.com/search?q=dmso+cfs&rlz=1C1CHBF_enUS975US975&oq=dmso&aqs=chrome.1.69i59l2j69i57j0i67j0i395i512l3j69i65.4102j1j7&sourceid=chrome&ie=UTF-8)
DMSO - Mycotoxins entering tissues? | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/dmso-mycotoxins-entering-tissues.52965/)
dmso arnica - Google Search(https://www.google.com/search?q=dmso+arnica&rlz=1C1CHBF_enUS975US975&oq=dmso&aqs=chrome.1.69i59l2j69i57j0i67j0i395i512l2j69i60l2.5296j1j7&sourceid=chrome&ie=UTF-8)
can exposure to black mold lead to cfs years later - Google Search(https://www.google.com/search?q=can+exposure+to+black+mold+lead+to+cfs+years+later&rlz=1C1CHBF_enUS975US975&oq=can+exposure+to+black+mold+lead+to+cfs+years+later&aqs=chrome..69i57j33i299.10753j1j7&sourceid=chrome&ie=UTF-8)
M.E., My Mold, & I… A Story of ME/CFS & Toxic Mold - Health Rising(https://www.healthrising.org/blog/2017/09/26/me-cfs-chronic-fatigue-toxic-mold-story-lissa/)
What Is Chronic Fatigue Syndrome? | RealTime Labs(https://realtimelab.com/blog/what-is-chronic-fatigue-syndrome/)
Toxic Mold Syndrome and How it Affects The Brain | Amen Clinics | Amen Clinics(https://www.amenclinics.com/blog/toxic-mold-syndrome-it-was-like-i-lost-my-personality/)
Can Mould & Mycotoxins Cause Chronic Fatigue Syndrome (CFS)?(https://www.alexmanos.co.uk/mould-mycotoxins-chronic-fatigue/)
Can Mold Cause Chronic Fatigue? - Fatigue To Flourish(https://fatiguetoflourish.com/chronic-fatigue-symptom-of-toxic-mold/)
Detection of Mycotoxins in Patients with Chronic Fatigue Syndrome(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3705282/)
New folder
"Neurotrophic" drugs cfs treatment - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJ416h00H5WUgPDewpXrt47-wOeTw:1637068281438&q=%22Neurotrophic%22+drugs+cfs+treatment&sa=X&ved=2ahUKEwjQ2ozL-pz0AhWP6p4KHfmsA08Q5t4CegQIChAB&biw=1072&bih=539&dpr=1.1)
(PDF) A Randomized Controlled Trial of Intranasal Neuropeptide Y in Patients With Major Depressive Disorder(https://www.researchgate.net/publication/345721621_A_Randomized_Controlled_Trial_of_Intranasal_Neuropeptide_Y_in_Patients_With_Major_Depressive_Disorder)
Drugs and Supplements For Chronic Fatigue Syndrome (ME/CFS) and/or Fibromyalgia - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/)
Artesunate - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/artesunate/)
Ampligen Chronic Fatigue Syndrome (ME/CFS) Resource Center - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/ampligen-chronic-fatigue-syndrome-mecfs-resource-center/)
CMX001 (Brincidofovir) - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/cmx001/)
Equilibriant / Oxymatrine in Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/oxymatrine-equilibriant/)
ivig-intravenous-gamma-globulin-therapy-for-chronic-fatigue-syndrome - Google Search(https://www.google.com/search?q=ivig-intravenous-gamma-globulin-therapy-for-chronic-fatigue-syndrome&rlz=1C1CHBF_enUS975US975&oq=ivig-intravenous-gamma-globulin-therapy-for-chronic-fatigue-syndrome&aqs=chrome..69i57j69i65.2007j0j4&sourceid=chrome&ie=UTF-8)
IVIG - Intravenous Gamma Globulin Therapy for Chronic Fatigue Syndrome (ME/CFS), Fibromyalgia and POTS - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/ivig-intravenous-gamma-globulin-therapy/)
The Case for IVIG Treatment in Chronic Fatigue Syndrome (ME/CFS), Fibromyalgia, Small Fiber Neuropathy, and POTS : IVIG#3 - Health Rising(https://www.healthrising.org/blog/2018/09/13/ivig-chronic-fatigue-syndrome-pots-fibromyalgia/)
A controlled trial of intravenous immunoglobulin G in chronic fatigue syndrome - PubMed(https://pubmed.ncbi.nlm.nih.gov/2239975/)
The 2021 Ramsay Awards: Leaky Brains, Healing the Gut-Brain Axis / Pathological Antibodies / Breathing Better? And More - Health Rising(https://www.healthrising.org/blog/2021/11/16/ramsay_awards_solve_mecfs_initiative_2021/)
Vistide (Cidofovir) - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/vistide-cidofovir/)
A Novel Neuroinflammatory Paradigm for Chronic Fatigue Syndrome (ME/CFS) - Health Rising(https://www.healthrising.org/blog/2020/05/27/neuroinflammatory-paradigm-chronic-fatigue-me-cfs/)
A Novel Nutriceutical Treatment of Myalgic Encephalitis/Chronic Fatigue Syndrome (ME/CFS): “What it is and what it is not” - a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.longdom.org/open-access/a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf)
Aneurysmal Subarachnoid Hemorrhage Trial in Xi'an (Magnesium-Rich Artificial Cerebrospinal Fluid) | Clincosm(https://www.clincosm.com/trial/aneurysmal-subarachnoid-hemorrhage-xian-magnesium-rich-artificial)
Chronic Fatigue Causes and How Nootropics Can Help | Thrivous®(https://thrivous.com/blogs/views/chronic-fatigue-causes-and-how-nootropics-can-help)
Bacopa monnieri Supplement — Health Benefits, Dosage, Side Effects | Examine.com(https://examine.com/supplements/bacopa-monnieri/)
Can the Drugs Namenda and Aricept Help After Brain Injury? | BrainLine(https://www.brainline.org/qa/can-drugs-namenda-and-aricept-help-after-brain-injury)
cell membrane glycerolphospholipids cfs - Google Search(https://www.google.com/search?q=cell+membrane+glycerolphospholipids+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJTa_VAWQIMk_GUsAGG8rzt34ysjA%3A1637067268924&ei=BKqTYcT0N47c-gTPlYvgAg&oq=cell+membrane+glycerolphospholipids+cfs&gs_lcp=Cgdnd3Mtd2l6EAMyBwghEAoQoAEyBwghEAoQoAE6BwgAEEcQsAM6BggAEBYQHjoICAAQCBANEB46BQgAEIYDOgUIIRCrAkoECEEYAFCpCljHFGCpF2gBcAF4AIABqAGIAcIEkgEDMC40mAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjEhqbo9pz0AhUOrp4KHc_KAiwQ4dUDCA4&uact=5)
cfs treatment neuropeptide - Google Search(https://www.google.com/search?q=cfs+treatment+neuropeptide&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJbvoEdcWpODz94rwSdORVrod567Q:1637068421629&ei=ha6TYbbZJcf2-gT5oaSQCA&start=10&sa=N&ved=2ahUKEwj2r_mN-5z0AhVHu54KHfkQCYIQ8NMDegQIARBM&biw=1072&bih=539&dpr=1.1)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer - PubMed(https://pubmed.ncbi.nlm.nih.gov/32309576/)
Piracetam + Choline - Google Search(https://www.google.com/search?q=Piracetam+%2B+Choline&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
complete list drugs cfs forum "hip" - Google Search(https://www.google.com/search?q=complete+list+drugs+cfs+forum+%22hip%22&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvK40MmRvXyotJtfv_YzA2nGTYyotA%3A1637080344723&ei=GN2TYea3K8rm-gTEtpnQBA&oq=complete+list+drugs+cfs+forum+%22hip%22&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAghEApKBAhBGABQlAxYuBJgyhhoAXACeACAAaUCiAGeBpIBBTMuMi4xmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjmo6nDp530AhVKs54KHURbBkoQ4dUDCA4&uact=5)
Supplements for Chronic Fatigue Syndrome?(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010273/)
Drugs - Health Rising(https://www.healthrising.org/blog/category/treatment/drugs/)
Drugs and Supplements For Chronic Fatigue Syndrome (ME/CFS) and/or Fibromyalgia - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6941554/)
intranasal neuropeptide cfs - Google Search(https://www.google.com/search?q=intranasal+neuropeptide+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvLlnIUIPjwVjbho8NH20SKVnt5oWA:1637079556777&ei=BNqTYczwLoz4-gTM8Y2ABg&start=10&sa=N&ved=2ahUKEwjMgs3LpJ30AhUMvJ4KHcx4A2AQ8NMDegQIARBM&biw=1072&bih=539&dpr=1.1)
L-Alpha glyceryl phosphorylcholine "cfs" - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJOJ6QwsCEjaTTurem6TiUplPf8DQ:1637066500964&q=L-Alpha+glyceryl+phosphorylcholine+%22cfs%22&sa=X&ved=2ahUKEwiepI3685z0AhVDs54KHRrzDMgQ5t4CegQICBAB&biw=1072&bih=539&dpr=1.1)
LDN, Nootropics, Rituximab and Fads: Maija Haavisto on Treating Chronic Fatigue Syndrome and Fibromyalgia - Health Rising(https://www.healthrising.org/blog/2014/05/28/ldn-nootropics-rituximab-fads-maija-haavisto-treating-chronic-fatigue-syndrome/)
14 Nootropics, aka Brain Enhancers, for Your Memory and More(https://www.healthline.com/health/nootropics-what-is-it-and-list-of-supplements)
Mitochondrial Modifying Nutrients in Treating Chronic Fatigue Syndrome: A 16-week Open-Label Pilot Study | Request PDF(https://www.researchgate.net/publication/321122761_Mitochondrial_Modifying_Nutrients_in_Treating_Chronic_Fatigue_Syndrome_A_16-week_Open-Label_Pilot_Study)
The Best Nootropics for Energy and Motivation | FOCL(https://focl.com/blogs/learn/your-guide-to-nootropics-for-energy-and-motivation)
neurotrophic cfs - Google Search(https://www.google.com/search?q=neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotrophic+cfs&aqs=chrome..69i57j69i65.12939j1j7&sourceid=chrome&ie=UTF-8)
NADH – Nootropics Expert(https://nootropicsexpert.com/nadh/)
Neurotrophic Factors - an overview | ScienceDirect Topics(https://www.sciencedirect.com/topics/neuroscience/neurotrophic-factors)
Biomarker for chronic fatigue syndrome identified : Nootropics(https://www.reddit.com/r/Nootropics/comments/bl05dl/biomarker_for_chronic_fatigue_syndrome_identified/)
Neurotrophin medication - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg:1637068069900&q=Neurotrophin+medication&sa=X&ved=2ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ1QJ6BAgoEAE&biw=1072&bih=539&dpr=1.1)
purinergic antagonists - Google Search(https://www.google.com/search?q=purinergic+antagonists&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
Treatment of chronic fatigue syndrome with 5-HT3 receptor antagonists - preliminary results: Scandinavian Journal of Rheumatology: Vol 29, No 113(https://www.tandfonline.com/doi/abs/10.1080/030097400750001851-1)
Nimodipine CFS - Google Search(https://www.google.com/search?sxsrf=AOaemvKQL56w5GblA4d7JHMHUTCBU41BYg:1637065876173&q=Nimodipine+CFS&sa=X&ved=2ahUKEwilkZfQ8Zz0AhXNv54KHQ03AhUQ1QJ6BAghEAE&biw=1072&bih=539&dpr=1.1)
Anyone had any success dealing with chronic fatigue syndrome? : Nootropics(https://www.reddit.com/r/Nootropics/comments/6mjzp7/anyone_had_any_success_dealing_with_chronic/)
Nootropics for chronic fatigue Syndrome - Google Search(https://www.google.com/search?q=Nootropics+for+chronic+fatigue+Syndrome&sxsrf=AOaemvIsp3UIiooMXWAwHqZVMWyWS583Vw:1637065920593&ei=wKSTYbLPI8Tc-gTkkrLQDg&start=10&sa=N&ved=2ahUKEwiyr67l8Zz0AhVErp4KHWSJDOoQ8NMDegUIARCvAw&biw=1072&bih=539&dpr=1.1)
Sulbutiamine as a Treatment for Chronic Fatigue Syndrome » Corpina(https://corpina.com/sulbutiamine-treatment-chronic-fatigue-syndrome/)
Nootropics for Chronic Fatigue? Well - Yes, but tread lightly(https://www.livecortex.com/nootropics-for-chronic-fatigue-well-yes-but-tread-lightly/)
Nootropics for Fatigue: How to Use Supplements to Boost Your Energy - AZOTH | Peak-Productivity Nootropic Supplements(https://azothwise.com/resources/nootropics-for-fatigue/)
nutraceutical neurotrophic cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotrophic+cfs&aqs=chrome..69i57.49667j1j7&sourceid=chrome&ie=UTF-8)
nimodipine use in me, jan 2014.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.actionforme.org.uk/assets/components/discuss/attachments/2/6193/nimodipine%20use%20in%20me,%20jan%202014.pdf)
peptide modulation. Some neurons, given neurotrophic factors show regrowth/repair cfs - Google Search(https://www.google.com/search?q=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg%3A1637068069900&ei=Ja2TYciqNsf9-gT67I0I&oq=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAgjECdKBAhBGABQoyJYzTFguzVoAXACeACAAXeIAeMCkgEDMC4zmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ4dUDCA4&uact=5)
List of ME/CFS Recovery and Improvement Stories | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/list-of-me-cfs-recovery-and-improvement-stories.80502/)
Phenylpiracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Phenylpiracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBcQAQ&biw=1072&bih=539&dpr=1.1)
When antibiotics turn toxic(https://www.nature.com/articles/d41586-018-03267-5)
Piracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Piracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBkQAQ&biw=1072&bih=539&dpr=1.1)
purinergic antagonists chronic fatigue syndrome - Google Search(https://www.google.com/search?q=purinergic+antagonists+chronic+fatigue+syndrome&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJGlXWykhodQ42YFbXm8Ki_Q--V9A%3A1637066666812&ei=qqeTYfz6MI7W-wSelaqoDQ&oq=purinergic+antagonists+chronic+fat&gs_lcp=Cgdnd3Mtd2l6EAMYATIFCCEQoAEyBQghEKABOgcIIxCwAxAnOgQIIxAnOgUIIRCrAjoGCAAQFhAeSgQIQRgBUNIJWIFVYJpmaAlwAHgAgAFqiAGnCZIBBDEwLjOYAQCgAQHIAQHAAQE&sclient=gws-wiz)
Tetramethoxyluteolin for the Treatment of Neurodegenerative Diseases - PubMed(https://pubmed.ncbi.nlm.nih.gov/30451113/)
Thesis - Personalized nootropic formulas to activate every kind of brain.(https://i.takethesis.com/google/?utm_campaign=14954151256&utm_source=google&utm_medium=cpc&utm_content=558937427235&utm_term=nootropic%20supplements&adgroupid=127211547054&gclid=Cj0KCQiAys2MBhDOARIsAFf1D1e4ewslWTbNnwb7spk_E_oAzFC8HDBoPuIIkzNBW3TQgkepj3trJtsaAlgxEALw_wcB)
Sci-Hub(https://sci-hubtw.hkvisa.net/)
Treatment | Health Rising's Chronic Fatigue Syndrome (ME/CFS) and Fibromyalgia Forums(https://www.healthrising.org/forums/forums/treatment.11/)
neurotropic cfs - Google Search(https://www.google.com/search?q=neurotropic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotropic+cfs&aqs=chrome..69i57.13372j1j7&sourceid=chrome&ie=UTF-8)
neurorehabilitation drug cfs - Google Search(https://www.google.com/search?q=neurorehabilitation+drug+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJG8sJskCkLEf1K4T9tnp6mlZTGZg%3A1637067605716&ei=VauTYaGOK-LE0PEP_MytsAg&oq=neurorehabilitation+drug+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6DQgAEIAEEIcCEMkDEBQ6BQgAEIAEOgQIABBDOgsILhCABBDHARCvAToFCC4QgAQ6BggAEBYQHjoICAAQFhAKEB46BQghEKABOgUIIRCrAkoECEEYAFDWCFiGKGDQK2gBcAJ4AIABigKIAfYJkgEFMC44LjGYAQCgAQHIAQrAAQE&sclient=gws-wiz&ved=0ahUKEwjhjPKI-Jz0AhViIjQIHXxmC4YQ4dUDCA4&uact=5)
Frontiers | Therapeutic Potential of Neurotrophins for Repair After Brain Injury: A Helping Hand From Biomaterials | Neuroscience(https://www.frontiersin.org/articles/10.3389/fnins.2019.00790/full)
Frontiers | The Influence of Neuron-Extrinsic Factors and Aging on Injury Progression and Axonal Repair in the Central Nervous System | Cell and Developmental Biology(https://www.frontiersin.org/articles/10.3389/fcell.2020.00190/full)
Neurotrophic factors, cellular bridges and gene therapy for spinal cord injury(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2278599/)
Neurotrophic drugs cfs - Google Search(https://www.google.com/search?q=Neurotrophic+drugs+cfs&rlz=1C1CHBF_enUS864US864&biw=1072&bih=539&sxsrf=AOaemvKdXB8DB9QDY7MneMEdqqGiXpNzAw%3A1637068176384&ei=kK2TYb7zFsHm-gSUsabwDQ&oq=Neurotrophic+drugs+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6BQgAEIAEOggIABAWEAoQHjoFCCEQoAE6BQghEKsCSgQIQRgAUOoJWJMXYLQbaAFwAngAgAGHAYgB0gOSAQMwLjSYAQCgAQHIAQnAAQE&sclient=gws-wiz&ved=0ahUKEwi--4CZ-pz0AhVBs54KHZSYCd4Q4dUDCA4&uact=5)
Postulated vasoactive neuropeptide immunopathology affecting the blood-brain/blood-spinal barrier in certain neuropsychiatric fatigue-related conditions: A role for phosphodiesterase inhibitors in treatment? - PubMed(https://pubmed.ncbi.nlm.nih.gov/19557103/)
Postulated Vasoactive Neuropeptide Autoimmunity in Fatigue-Related Conditions: A Brief Review and Hypothesis(https://www.hindawi.com/journals/jir/2006/576425/)
Frontiers | Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome | Frontiers in Systems Neuroscience(https://www.frontiersin.org/articles/10.3389/fnsys.2021.698240/full)
nutraceutical neurotrophin - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophin&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro&aqs=chrome.1.69i57j33i160l4.20328j1j7&sourceid=chrome&ie=UTF-8)
Fibromyalgia Causes And Treatment With Guaifenesin, Amitriptyline, Kratom, Flexeril, And Others. -(https://www.sunshinentc.com/fibromyalgia-causes-and-treatment-with-guaifenesin-amitriptyline-kratom-flexeril-and-others/)
A systematic review of nutraceutical interventions for mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome | Journal of Translational Medicine | Full Text(https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-021-02742-4)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro+cfs&aqs=chrome..69i57.29295j1j7&sourceid=chrome&ie=UTF-8)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvIckRIy2NrjMpHNTWDR5zbOk_IICA:1637068696696&ei=mK-TYfj3KcPY-wSZh7b4CQ&start=10&sa=N&ved=2ahUKEwj4o46R_Jz0AhVD7J4KHZmDDZ8Q8NMDegQIARBN&biw=1072&bih=539&dpr=1.1)
Microglial Inhibiting Drugs, Supplements and Botanicals to Combat Neuroinflammation - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/microglial-inhibiting-drugs-combat-neuroinflammation/)
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome—Metabolic Disease or Disturbed Homeostasis due to Focal Inflammation in the Hypothalamus? - ME-CFS-JPET-9-2018.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/mastcellmaster.com/documents/2018-09/ME-CFS-JPET-9-2018.pdf)
neuropeptide Y - Clincosm(https://www.clincosm.com/search?q=neuropeptide%20Y)
General Treatment | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/forums/general-treatment.5/)
Peptidergic Drugs for Treatment of Traumatic Brain Injury(https://www.medscape.com/viewarticle/780437_5)
Supplements and Drugs That Reduce or Prevent PEM (Post-Exertional Malaise) | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/supplements-and-drugs-that-reduce-or-prevent-pem-post-exertional-malaise.48438/)
MAGNESIUM-RICH ARTIFICIAL CEREBROSPINAL FLUID cfs - Google Search(https://www.google.com/search?q=MAGNESIUM-RICH+ARTIFICIAL+CEREBROSPINAL+FLUID+cfs&rlz=1C1CHBF_enUS975US975&oq=MAGNESIUM-RICH+ARTIFICIAL+CEREBROSPINAL+FLUID+cfs&aqs=chrome..69i57.2289j1j7&sourceid=chrome&ie=UTF-8)
New folder
Resources | ME/CFS Initiative | Stanford Medicine(https://med.stanford.edu/chronicfatiguesyndrome/resources.html)
Nootropics for chronic fatigue Syndrome - Google Search(https://www.google.com/search?q=Nootropics+for+chronic+fatigue+Syndrome&sxsrf=AOaemvIsp3UIiooMXWAwHqZVMWyWS583Vw:1637065920593&ei=wKSTYbLPI8Tc-gTkkrLQDg&start=10&sa=N&ved=2ahUKEwiyr67l8Zz0AhVErp4KHWSJDOoQ8NMDegUIARCvAw&biw=1072&bih=539&dpr=1.1)
Better Thinking for Chronic Fatigue Syndrome and Fibromyalgia: the Nootropics - the "Smart Drugs" - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/nootropics/)
LDN, Nootropics, Rituximab and Fads: Maija Haavisto on Treating Chronic Fatigue Syndrome and Fibromyalgia - Health Rising(https://www.healthrising.org/blog/2014/05/28/ldn-nootropics-rituximab-fads-maija-haavisto-treating-chronic-fatigue-syndrome/)
Chronic Fatigue Causes and How Nootropics Can Help | Thrivous®(https://thrivous.com/blogs/views/chronic-fatigue-causes-and-how-nootropics-can-help)
Nootropics for Chronic Fatigue? Well - Yes, but tread lightly(https://www.livecortex.com/nootropics-for-chronic-fatigue-well-yes-but-tread-lightly/)
Bacopa monnieri Supplement — Health Benefits, Dosage, Side Effects | Examine.com(https://examine.com/supplements/bacopa-monnieri/)
Piracetam + Choline - Google Search(https://www.google.com/search?q=Piracetam+%2B+Choline&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
Supplements for Chronic Fatigue Syndrome?(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5010273/)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer - PubMed(https://pubmed.ncbi.nlm.nih.gov/32309576/)
cell membrane glycerolphospholipids cfs - Google Search(https://www.google.com/search?q=cell+membrane+glycerolphospholipids+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJTa_VAWQIMk_GUsAGG8rzt34ysjA%3A1637067268924&ei=BKqTYcT0N47c-gTPlYvgAg&oq=cell+membrane+glycerolphospholipids+cfs&gs_lcp=Cgdnd3Mtd2l6EAMyBwghEAoQoAEyBwghEAoQoAE6BwgAEEcQsAM6BggAEBYQHjoICAAQCBANEB46BQgAEIYDOgUIIRCrAkoECEEYAFCpCljHFGCpF2gBcAF4AIABqAGIAcIEkgEDMC40mAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwjEhqbo9pz0AhUOrp4KHc_KAiwQ4dUDCA4&uact=5)
Clinical Uses of Membrane Lipid Replacement Supplements in Restoring Membrane Function and Reducing Fatigue in Chronic Diseases and Cancer(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6941554/)
Nootropics for Fatigue: How to Use Supplements to Boost Your Energy - AZOTH | Peak-Productivity Nootropic Supplements(https://azothwise.com/resources/nootropics-for-fatigue/)
L-Alpha glyceryl phosphorylcholine "cfs" - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJOJ6QwsCEjaTTurem6TiUplPf8DQ:1637066500964&q=L-Alpha+glyceryl+phosphorylcholine+%22cfs%22&sa=X&ved=2ahUKEwiepI3685z0AhVDs54KHRrzDMgQ5t4CegQICBAB&biw=1072&bih=539&dpr=1.1)
14 Nootropics, aka Brain Enhancers, for Your Memory and More(https://www.healthline.com/health/nootropics-what-is-it-and-list-of-supplements)
The Best Nootropics for Energy and Motivation | FOCL(https://focl.com/blogs/learn/your-guide-to-nootropics-for-energy-and-motivation)
Thesis - Personalized nootropic formulas to activate every kind of brain.(https://i.takethesis.com/google/?utm_campaign=14954151256&utm_source=google&utm_medium=cpc&utm_content=558937427235&utm_term=nootropic%20supplements&adgroupid=127211547054&gclid=Cj0KCQiAys2MBhDOARIsAFf1D1e4ewslWTbNnwb7spk_E_oAzFC8HDBoPuIIkzNBW3TQgkepj3trJtsaAlgxEALw_wcB)
NADH – Nootropics Expert(https://nootropicsexpert.com/nadh/)
Biomarker for chronic fatigue syndrome identified : Nootropics(https://www.reddit.com/r/Nootropics/comments/bl05dl/biomarker_for_chronic_fatigue_syndrome_identified/)
purinergic antagonists - Google Search(https://www.google.com/search?q=purinergic+antagonists&rlz=1C1CHBF_enUS864US864&sourceid=chrome&ie=UTF-8)
Treatment of chronic fatigue syndrome with 5-HT3 receptor antagonists - preliminary results: Scandinavian Journal of Rheumatology: Vol 29, No 113(https://www.tandfonline.com/doi/abs/10.1080/030097400750001851-1)
Anyone had any success dealing with chronic fatigue syndrome? : Nootropics(https://www.reddit.com/r/Nootropics/comments/6mjzp7/anyone_had_any_success_dealing_with_chronic/)
Sulbutiamine as a Treatment for Chronic Fatigue Syndrome » Corpina(https://corpina.com/sulbutiamine-treatment-chronic-fatigue-syndrome/)
Phenylpiracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Phenylpiracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBcQAQ&biw=1072&bih=539&dpr=1.1)
Piracetam - Google Search(https://www.google.com/search?sxsrf=AOaemvJ_K_wPkDNCB7kjFOAgGx1WCe3QsQ:1637066173425&q=Piracetam&sa=X&ved=2ahUKEwi0g_bd8pz0AhUIpZ4KHcWlDw04ChDVAnoECBkQAQ&biw=1072&bih=539&dpr=1.1)
Nimodipine CFS - Google Search(https://www.google.com/search?sxsrf=AOaemvKQL56w5GblA4d7JHMHUTCBU41BYg:1637065876173&q=Nimodipine+CFS&sa=X&ved=2ahUKEwilkZfQ8Zz0AhXNv54KHQ03AhUQ1QJ6BAghEAE&biw=1072&bih=539&dpr=1.1)
Drugs and Supplements For Chronic Fatigue Syndrome (ME/CFS) and/or Fibromyalgia - Health Rising(https://www.healthrising.org/treating-chronic-fatigue-syndrome/drugs/)
nimodipine use in me, jan 2014.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.actionforme.org.uk/assets/components/discuss/attachments/2/6193/nimodipine%20use%20in%20me,%20jan%202014.pdf)
List of ME/CFS Recovery and Improvement Stories | Phoenix Rising ME/CFS Forums(https://forums.phoenixrising.me/threads/list-of-me-cfs-recovery-and-improvement-stories.80502/)
When antibiotics turn toxic(https://www.nature.com/articles/d41586-018-03267-5)
purinergic antagonists chronic fatigue syndrome - Google Search(https://www.google.com/search?q=purinergic+antagonists+chronic+fatigue+syndrome&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJGlXWykhodQ42YFbXm8Ki_Q--V9A%3A1637066666812&ei=qqeTYfz6MI7W-wSelaqoDQ&oq=purinergic+antagonists+chronic+fat&gs_lcp=Cgdnd3Mtd2l6EAMYATIFCCEQoAEyBQghEKABOgcIIxCwAxAnOgQIIxAnOgUIIRCrAjoGCAAQFhAeSgQIQRgBUNIJWIFVYJpmaAlwAHgAgAFqiAGnCZIBBDEwLjOYAQCgAQHIAQHAAQE&sclient=gws-wiz)
neurotrophic cfs - Google Search(https://www.google.com/search?q=neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotrophic+cfs&aqs=chrome..69i57j69i65.12939j1j7&sourceid=chrome&ie=UTF-8)
neurotropic cfs - Google Search(https://www.google.com/search?q=neurotropic+cfs&rlz=1C1CHBF_enUS864US864&oq=neurotropic+cfs&aqs=chrome..69i57.13372j1j7&sourceid=chrome&ie=UTF-8)
post stroke neurotrophic neurorehabilitation medicine textbook - Google Search(https://www.google.com/search?rlz=1C1TSNO_enUS609US609&biw=1290&bih=858&ei=uKNsXKD1K8Lk9APZ5b-gDg&q=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&oq=post+stroke+neurotrophic+neurorehabilitation+medicine+textbook&gs_l=psy-ab.3...143106.154126..158615...1.0..0.134.1464.6j8......0....1..gws-wiz.......0i71j35i304i39j33i10.oOyfywRfLLs)
neurorehabilitation drug cfs - Google Search(https://www.google.com/search?q=neurorehabilitation+drug+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJG8sJskCkLEf1K4T9tnp6mlZTGZg%3A1637067605716&ei=VauTYaGOK-LE0PEP_MytsAg&oq=neurorehabilitation+drug+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6DQgAEIAEEIcCEMkDEBQ6BQgAEIAEOgQIABBDOgsILhCABBDHARCvAToFCC4QgAQ6BggAEBYQHjoICAAQFhAKEB46BQghEKABOgUIIRCrAkoECEEYAFDWCFiGKGDQK2gBcAJ4AIABigKIAfYJkgEFMC44LjGYAQCgAQHIAQrAAQE&sclient=gws-wiz&ved=0ahUKEwjhjPKI-Jz0AhViIjQIHXxmC4YQ4dUDCA4&uact=5)
peptide modulation. Some neurons, given neurotrophic factors show regrowth/repair cfs - Google Search(https://www.google.com/search?q=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg%3A1637068069900&ei=Ja2TYciqNsf9-gT67I0I&oq=peptide+modulation.+Some+neurons%2C+given+neurotrophic+factors+show+regrowth%2Frepair+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BAgjECdKBAhBGABQoyJYzTFguzVoAXACeACAAXeIAeMCkgEDMC4zmAEAoAEByAEIwAEB&sclient=gws-wiz&ved=0ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ4dUDCA4&uact=5)
Neurotrophic Peptide - an overview | ScienceDirect Topics(https://www.sciencedirect.com/topics/biochemistry-genetics-and-molecular-biology/neurotrophic-peptide)
Neurotrophic Factors - an overview | ScienceDirect Topics(https://www.sciencedirect.com/topics/neuroscience/neurotrophic-factors)
Frontiers | Therapeutic Potential of Neurotrophins for Repair After Brain Injury: A Helping Hand From Biomaterials | Neuroscience(https://www.frontiersin.org/articles/10.3389/fnins.2019.00790/full)
Frontiers | The Influence of Neuron-Extrinsic Factors and Aging on Injury Progression and Axonal Repair in the Central Nervous System | Cell and Developmental Biology(https://www.frontiersin.org/articles/10.3389/fcell.2020.00190/full)
Neurotrophic factors, cellular bridges and gene therapy for spinal cord injury(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2278599/)
Neurotrophin medication - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvKGWCYD03vNkH3e1pbIuNdyGP6Izg:1637068069900&q=Neurotrophin+medication&sa=X&ved=2ahUKEwiI0Z3m-Zz0AhXHvp4KHXp2AwEQ1QJ6BAgoEAE&biw=1072&bih=539&dpr=1.1)
Neurotrophic drugs cfs - Google Search(https://www.google.com/search?q=Neurotrophic+drugs+cfs&rlz=1C1CHBF_enUS864US864&biw=1072&bih=539&sxsrf=AOaemvKdXB8DB9QDY7MneMEdqqGiXpNzAw%3A1637068176384&ei=kK2TYb7zFsHm-gSUsabwDQ&oq=Neurotrophic+drugs+cfs&gs_lcp=Cgdnd3Mtd2l6EAM6BwgAEEcQsAM6BwgAELADEEM6BQgAEIAEOggIABAWEAoQHjoFCCEQoAE6BQghEKsCSgQIQRgAUOoJWJMXYLQbaAFwAngAgAGHAYgB0gOSAQMwLjSYAQCgAQHIAQnAAQE&sclient=gws-wiz&ved=0ahUKEwi--4CZ-pz0AhVBs54KHZSYCd4Q4dUDCA4&uact=5)
"Neurotrophic" drugs cfs treatment - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJ416h00H5WUgPDewpXrt47-wOeTw:1637068281438&q=%22Neurotrophic%22+drugs+cfs+treatment&sa=X&ved=2ahUKEwjQ2ozL-pz0AhWP6p4KHfmsA08Q5t4CegQIChAB&biw=1072&bih=539&dpr=1.1)
cfs treatment neuropeptide - Google Search(https://www.google.com/search?q=cfs+treatment+neuropeptide&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvJbvoEdcWpODz94rwSdORVrod567Q:1637068421629&ei=ha6TYbbZJcf2-gT5oaSQCA&start=10&sa=N&ved=2ahUKEwj2r_mN-5z0AhVHu54KHfkQCYIQ8NMDegQIARBM&biw=1072&bih=539&dpr=1.1)
Postulated vasoactive neuropeptide immunopathology affecting the blood-brain/blood-spinal barrier in certain neuropsychiatric fatigue-related conditions: A role for phosphodiesterase inhibitors in treatment? - PubMed(https://pubmed.ncbi.nlm.nih.gov/19557103/)
Postulated Vasoactive Neuropeptide Autoimmunity in Fatigue-Related Conditions: A Brief Review and Hypothesis(https://www.hindawi.com/journals/jir/2006/576425/)
Frontiers | Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome | Frontiers in Systems Neuroscience(https://www.frontiersin.org/articles/10.3389/fnsys.2021.698240/full)
A Novel Nutriceutical Treatment of Myalgic Encephalitis/Chronic Fatigue Syndrome (ME/CFS): “What it is and what it is not” - a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf(chrome-extension://oemmndcbldboiebfnladdacbdfmadadm/https:/www.longdom.org/open-access/a-novel-nutriceutical-treatment-of-myalgic-encephalitischronic-fatigue-syndrome-mecfs-what-it-is-and-what-it-is-not-2165-8048-10002452.pdf)
nutraceutical cfs - Google Search(https://www.google.com/search?rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvI5tGny2KtFiuTU-yYbuCUN-JdfWQ:1637068508214&q=nutraceutical+cfs&spell=1&sa=X&ved=2ahUKEwiPkJ63-5z0AhWJrp4KHV8OB60QBSgAegQIARA0&biw=1072&bih=539&dpr=1.1)
nutraceutical neurotrophin - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophin&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro&aqs=chrome.1.69i57j33i160l4.20328j1j7&sourceid=chrome&ie=UTF-8)
nutraceutical neurotrophic cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotrophic+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotrophic+cfs&aqs=chrome..69i57.49667j1j7&sourceid=chrome&ie=UTF-8)
Fibromyalgia Causes And Treatment With Guaifenesin, Amitriptyline, Kratom, Flexeril, And Others. -(https://www.sunshinentc.com/fibromyalgia-causes-and-treatment-with-guaifenesin-amitriptyline-kratom-flexeril-and-others/)
A systematic review of nutraceutical interventions for mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome | Journal of Translational Medicine | Full Text(https://translational-medicine.biomedcentral.com/articles/10.1186/s12967-021-02742-4)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&oq=nutraceutical+neurotro+cfs&aqs=chrome..69i57.29295j1j7&sourceid=chrome&ie=UTF-8)
nutraceutical neurotro cfs - Google Search(https://www.google.com/search?q=nutraceutical+neurotro+cfs&rlz=1C1CHBF_enUS864US864&sxsrf=AOaemvIckRIy2NrjMpHNTWDR5zbOk_IICA:1637068696696&ei=mK-TYfj3KcPY-wSZh7b4CQ&start=10&sa=N&ved=2ahUKEwj4o46R_Jz0AhVD7J4KHZmDDZ8Q8NMDegQIARBN&biw=1072&bih=539&dpr=1.1)
Mitochondrial Modifying Nutrients in Treating Chronic Fatigue Syndrome: A 16-week Open-Label Pilot Study | Request PDF(https://www.researchgate.net/publication/321122761_Mitochondrial_Modifying_Nutrients_in_Treating_Chronic_Fatigue_Syndrome_A_16-week_Open-Label_Pilot_Study)
You searched for CHRONIc fatigue - ICNR(https://icnr.com/?s=CHRONIc+fatigue)
Is a Hidden Infection Causing Your Chronic Fatigue?(https://www.jillcarnahan.com/2016/05/07/hidden-infection-causing-fatigue/)
Chronic Fatigue - Kelatox(https://www.kelatox.com/chronic-fatigue/)
Phoenix Rising ME/CFS Forums
This is a thread for ME/CFS recovery or improvement stories, detailing patient accounts of treatments which have led to full recovery or substantial improvements in their overall ME/CFS symptoms, as well as treatments which have substantially improved specific ME/CFS symptoms (like fatigue, PEM, brain fog, sound sensitivity, etc).
The degree of improvement a patient achieved (where known) is given in terms of the number of levels they moved up on the ME/CFS scale of: very severe, severe, moderate, mild, remission. For example, if the patient was initially severe, and then moved up to mild as a result of a treatment, that is a 2-level gain.
If anyone knows of any other recovery or improvement stories that could be included in this thread, please post. That way we can build up a repository of interesting treatments.
ME/CFS Recovery and Improvement Stories
Valcyte (Valganciclovir) — Antiviral Drug for Herpesviruses
Valcyte is a potent antiviral drug effective against a wide spectrum of herpesviruses, including EBV, HHV-6, cytomegalovirus, varicella-zoster and herpes simplex. Typical dose for ME/CFS is 900 mg daily. Studies which have examined the efficacy of Valcyte for ME/CFS are detailed in this post.
• ME/CFS patient (OnlyInDreams) — with active cytomegalovirus infection made a 2-level gain, moving from moderate ME/CFS to remission, as a result of taking Valcyte 900 mg daily; but if he stops the Valcyte, he finds the ME/CFS soon returns.
• ME/CFS patient (Mariesak) — went into a partial remission lasting 8 years, after a 9 month course of Valcyte (her health gains remained even after she stopped the Valcyte).
• ME/CFS patient (Mariesak's daughter) — completed a 12 month course of Valcyte and also went into remission, and has remained in remission for over a decade.
• ME/CFS patient (JenB) — found Valcyte had a "profound effect".
• ME/CFS patient (TracyD) — improved on low-dose Valcyte 450 mg once daily.
• ME/CFS patient (SOC) — made a 1-level gain on Valcyte, moving from severe to moderate.
• ME/CFS patient (SOC's daughter) — made a 1½-level gain, going from nearly housebound (moderate ME/CFS) to full remission after 18 months on Valcyte for active HHV-6.
• ME/CFS patient (Peter42) — with mild ME/CFS made a 1-level gain and became almost free of ME/CFS symptoms after taking Valcyte for a year. Then 2 years after he stopped taking Valcyte, his ME/CFS returned.
• ME/CFS patient (ArgyrosfeniX) — made a 1-level gain moving from moderate to mild ME/CFS after two years of Valcyte at 900 mg once daily.
• ME/CFS patient (Dan_USAAZ) — with severe HHV-6-associated ME/CFS improved on Valcyte 900 mg daily, perhaps achieving a ½-level gain.
• ME/CFS patient (jstefl) — achieved a 1-level gain moving from severe ME/CFS to moderate after 450 mg dose of Valcyte twice a day for 10 months. This improvement occurred in 2008, and has lasted more than a decade.
• ME/CFS patient (RUkiddingME) — with severe ME/CFS and bedbound most of the time was able to resume driving and shopping again after a year on Valcyte (1-level gain).
Valtrex (Valaciclovir) — Antiviral Drug
Valtrex is an antiviral effective against Epstein-Barr virus. Some ME/CFS doctors prescribe this drug to ME/CFS patients who have an active EBV infection. For EBV ME/CFS treatment, Dr Lerner used a dose of 1000 mg four times daily. Studies which have examined the efficacy of Valtrex for EBV-associated ME/CFS are detailed in this post.
• ME/CFS patient (Leah) — with severe ME/CFS achieved near recovery (2½-level gain) from a course of Valtrex prescribed by Dr Martin Lerner. She is now able to work and socialize, but cannot exercise vigorously.
• ME/CFS patient (Heather) — fully recovered after a year or so of taking Valtrex prescribed by Dr Martin Lerner.
• ME/CFS patient (Janet, see comments section) — with severe ME/CFS achieved 2-level gain, moving up to mild ME/CFS after taking Valtrex for many years.
Valtrex (Valaciclovir) Plus Valcyte (Valganciclovir) Together
• ME/CFS patient (Jacyln) — with severe EBV ME/CFS achieved 2-level gain, moving up to mild ME/CFS after taking a course of Valcyte 450 mg twice daily plus Valtrex 1500 mg four times daily prescribed by Dr Martin Lerner.
• ME/CFS patient (Marilynne, see comments section) — with severe ME/CFS achieved 2-level gain, moving up to mild ME/CFS after taking a course of Valcyte 450 mg twice daily plus Valtrex 1500 mg four times daily prescribed by Dr Martin Lerner.
• ME/CFS patient (Renee) — with moderate to mild ME/CFS associated with active EBV and cytomegalovirus recovered to a near-normal life (1-level gain) after a course of Valtrex and Valcyte prescribed by Dr Martin Lerner. Leads near normal life but cannot exercise vigorously.
Tenofovir (Viread) — Antiviral Drug
Tenofovir is an antiviral drug normally used for hepatitis B virus or HIV. When used to treat ME/CFS, Dr John Chia reports it works for almost 1 in 3 ME/CFS patients. Refs: 1 2 Some ME/CFS patients find tenofovir hard to tolerate initially, but this issue can be avoided by starting at low doses of 30 mg daily, and working up to the full dose of 300 mg daily.
• This ME/CFS patient (Keela Too) — experienced a 1-level gain moving from approximately severe ME/CFS to moderate after taking a course of tenofovir for 12 months. The gains in her health have remained permanently so far.
• ME/CFS patient — with active coxsackievirus B4 infection noticed substantial improvements from tenofovir after just 4 months at 150 mg daily (he took combination pill containing tenofovir + lamivudine). He said: "I almost have my life back. My endurance has increased beyond belief, and PEM is a thing of the past". Even after he stopped tenofovir at the 4 month point, his gains remained. He also found that tenofovir resulted in a suspected nail psoriasis (autoimmune condition) he had for 5 years to suddenly heal.
Antiretrovirals (Tenofovir, Raltegravir, AZT)
These HIV antivirals are immunomodulatory, and can inhibit human endogenous retroviruses (HERVs). Ref: 1 HERV-K activity has been linked to moderate (but not severe) ME/CFS. Ref: 1
• ME/CFS patients (Dr Jamie Deckoff-Jones and her daughter Ali) — both had improvements in their ME/CFS after taking tenofovir 300 mg once daily plus raltegravir 400 mg twice daily.
• ME/CFS patient (Dr Michael Snyderman) — had success in treating his ME/CFS with AZT, raltegravir and tenofovir.
Ampligen (Rintatolimod)
Ampligen is an interferon inducer which stimulates the immune system to fight viral infections. Ampligen has been shown efficacious for ME/CFS in a phase III clinical trial. Ampligen is licensed as an ME/CFS treatment in Argentina, but not in the US or Europe, so is difficult to obtain, and not normally covered by insurance. Ampligen is expensive, costing around $15,000 a year (excluding the medical costs of the infusions). Ampligen is administered by intravenous infusion twice a week.
• ME/CFS patient (Kelvin Lord) — after a year on Ampligen infusions went from severe ME/CFS ("I was barely able to get out of bed") to mild (2-level gain) ME/CFS. He said "Ampligen makes you feel like you have the flu twice a week. The reality is when you are on it, it is pretty much hell. Hell with hope". See his Ampligen blogs here.
• ME/CFS patient (niall) — improved "by 30%" after a course of Ampligen.
• ME/CFS patient (LaurelW) — was on Ampligen for 7 years, improved from severe to moderate (1-level gain), and maintained their gains in health even after stopping Ampligen.
Some other Ampligen stories here.
Oxymatrine (Equilibrant) — Immunomodulator
Oxymatrine is an immunomodulatory herbal extract which ramps up the antiviral Th1 immune response. Dr John Chia uses oxymatrine to treat enterovirus ME/CFS.
• ME/CFS patient (Diwi9) — with enterovirus ME/CFS achieved a substantial improvement from oxymatrine (in the form of Dr Chia's Equilibrant).
• ME/CFS patient (tdog333) — did well taking 6 pills of oxymatrine daily.
• ME/CFS patient (.jm.) — with mild enterovirus ME/CFS went into remission (1-level gain) as a result of taking oxymatrine.
GcMAF — Immunomodulator
GcMAF is an immunomodulatory protein which stimulates macrophages to fight pathogens in the body. GcMAF can be taken orally, by transdermal cream, or via injection. Some sources for GcMAF in this post.
• ME/CFS patient (carlystar13) — obtained a 3-level gain, going from severe ME/CFS to full remission, after a year of taking Goleic GcMAF.
• ME/CFS patient (CindyWillis) — almost completely recovered taking from 40 to 80 ng of GcMAF over a month and a half.
Low-Dose Oral Interferon Alpha
Interferon alpha is a potent immunomodulator that activates the intracellular immune response. You can buy interferon alpha suppositories or nasal sprays cheaply from Russian online pharmacies (see this post), and these may be adapted for oral use.
• ME/CFS patient (Linda) — fully recovered using low doses of interferon alpha taken orally (rather than the usual subcutaneous injection route). She took 250 IU of interferon alpha orally four times a day. Brain fog began to improve after a few weeks, and her ME/CFS pain symptom cleared up after two months. Possibly this oral route interferon targets enterovirus infections in the stomach tissues?
High-Dose Selenium
The high-dose selenium protocol used here is detailed in this post.
• ME/CFS patient (Hip) — achieved a ½-level gain moving from the bottom end of moderate to the top within only 10 days as a result of high-dose selenium (taking selenomethionine 400 mcg once daily on an empty stomach).
Inosine + DMAE = Home-Made Imunovir
According to a ME/CFS patient blog article (now deleted), mixing inosine and DMAE together creates what is equivalent to the antiviral drug Imunovir (isoprinosine). To create home-made Imunovir, as this post details, you simply take equal weights of these two supplements (eg, DMAE 500 mg plus inosine 500 mg). The two supplements will combine in the stomach to make the molecular complex that is Imunovir.
Note however that many ME/CFS patients cannot tolerate Imunovir, and some report getting permanently worse from it: see this thread and this thread.
• ME/CFS patient (Doug) — with major mold exposure-induced illness was more-or-less cured by inosine 2000 mg daily plus DMAE 700 mg, as well as other supplements. See also here. Doug tried inosine on its own for some months, but it was not until he added DMAE to the inosine that he obtained a large increase in health.
Low-Dose Abilify (Aripiprazole)
The Open Medicine Foundation are currently running a clinical trial to determine whether low doses of the drug Abilify (aripiprazole) can benefit ME/CFS. Trial results are not yet available, but several ME/CFS patients have found Abilify in doses of around 0.1 to 2.5 mg daily rapidly leads to major improvements in their ME/CFS symptoms.
• ME/CFS patient (Martin aka paused||M.E.) — moved from very severe to moderate (2-level gain) after two months on Abilify 4 mg daily (plus LDN and Celebrex).
• ME/CFS patient (Jaybee00) — moved from moderate to mild (1-level gain) after 6 weeks on Abilify 2 mg daily. He noticed improvements began to manifest after a week or so.
• ME/CFS patient (Butydoc) — moved from severe to moderate (1-level gain) within a matter of weeks on 0.2 mg of Abilify daily.
• ME/CFS patient (Jessie 107) — improved on 2.5 mg Abilify daily. She said she did not notice much improvement until she reached the 2 mg daily dose level.
• ME/CFS patient (erist) — back in 2012 took 0.5 mg to 1 mg Abilify daily, and found more energy, more appetite, much easier time getting up in the morning, but also restless agitation.
Low-Dose Naltrexone (LDN)
The drug naltrexone at a low dose of 3 to 4.5 mg daily before bed, can have positive effects for ME/CFS as well as autoimmune and neurodegenerative diseases. Dr John Chia finds LDN helps only 10% to 20% of ME/CFS patients, but for those it helps, it does so significantly. Refs: 1 2
• ME/CFS patient (Maija Haavisto) — found LDN had immediate benefits, improving fatigue and muscle weakness, making PEM episodes rarer and milder, and almost eliminating her chronic fever and chronic urticaria symptoms (see "My Own Perspective" section in the link).
Nimodipine (Nimotop)
Nimodipine is a calcium channel blocker which increases blood flow to the brain. Dr David Mason Brown says nimodipine helps 20% of ME/CFS patients quickly, and another 20% over six months. The Mason Brown protocol begins with a nimodipine dose of 7.5 mg per day. The dose is slowly increased by 7.5 mg each week, up to a maximum dose of 120 mg daily. Nimodipine has many drug interactions.
• ME/CFS patient — with severe ME/CFS became very mild (2-level gain) on 90 mg of nimodipine daily (30 mg taken three times daily). This patient has maintained his improvement in health for 7 years without relapse. However, every time he reduces his nimodipine dose, his ME/CFS gets worse again. He finds the minimum dose that produces some benefits is 45 mg daily; but it is not until he increases the dose to 90 mg daily does he get the full benefits
Rapamycin (Sirolimus, Rapamune)
Rapamycin is a drug which calms the immune response, and is usually used to prevent organ transplant rejection, and to treat some autoimmune diseases. It is also used by the anti-aging community, as it extends lifespan in animal tests.
• Several ME/CFS patients — observed improvements on rapamycin.
Tagamet (Cimetidine)
Tagamet is an H2 antihistamine that has immunomodulatory properties: it boosts NK cell activity, and reduces T-regs (doing the latter may not be a good idea in autoimmunity or in those with organ transplants).
Tagamet is a known testicular toxicant, but vitamin B12 helps mitigate this damage. Ref: 1. Tagamet has a lot of interactions with other drugs, so you may like to consult a drug interactions checker to check if it interacts with any drugs you are taking.
• ME/CFS patient (faith.hope.love) — took Tagamet 200 mg every other day, and was able to go back to work.
Ketogenic Diet
A ketogenic diet is a very low-carb and high-fat diet. On a ketogenic diet, the brain is fueled by ketones rather than the usual glucose. Ketogenic diets are known to increase the number of mitochondria in brain cells. These diets are traditionally prescribed for patients with seizures.
• ME/CFS patient (leokitten) — with severe bedbound ME/CFS improved substantially with a ketogenic diet, so that he is no longer bedbound or housebound (2-level gain). But later he said he found it hard to sustain the diet long-term, and found the diet did not prevent crashes when he tried to live a regular life, so currently he is back to bedbound.
Helminth Therapy
Helminths are microscopic parasitic worms which live in the intestines. They modulate the immune function in the gut, which can have benefit in some diseases, especially autoimmune illnesses.
• ME/CFS patient (Gyre) — achieved a 2-level gain, moving from severe ME/CFS to mild as a result of helminth therapy, using the worm Necator americanus.
• ME/CFS patient (Henrik) — went from moderate to mild (1-level gain) using helminthic therapy with Necator americanus.
Several more ME/CFS recovery and improvement stories from Necator americanus detailed here.
Kambo (Medicine From an Amazonian Frog)
Kambo is a substance secreted by the Amazonian giant leaf frog, containing a range of bioactive principles, including sauvagine, a hormone related to the experimental ME/CFS drug CT38 (the Cortene Peptide).
• ME/CFS patient (Jox) — went from severe to near remission (2½-level gain) by taking the Amazonian medicine kambo once a week.
Fecal Microbiota Transplantation (FMT)
FMT involves transplanting fecal material from a healthy donor into a patient's intestines.
• Chronic Lyme patient (Kasia Vermaire) — with severe illness experienced a 3-level gain and made a full recovery after FMT treatment at the Taymount Clinic. Blog article here.
Low-Level Laser Therapy / LED Light Therapy
Also known as photobiomodulation, this therapy uses red or infrared light emitted by a laser or LED lamp, applied to the area of interest, such as the head and brain. Light of these wavelengths is known to stimulate mitochondrial complex IV.
• ME/CFS patient (ScottTriGuy) — housebound with moderate ME/CFS quickly recovered enough health to return to work (1-level gain) as a result low-level laser therapy (LLLT) applied to his head.
• ME/CFS patient (Johannes) — move from severe ME/CFS to moderate ME/CFS (1-level gain) using red and infrared light therapy on on his entire head and body daily (10 minutes on the front of the body and 10 minutes on the back). Light power used is 90 mW/cm2. Ref: 1
C60 Supplement
C60 (buckminsterfullerene) is a molecule comprising 60 carbon atoms that are arranged into a spherical shape. C60 targets the mitochondria where it acts as a non-perishable resuable antioxidant. 1
• ME/CFS patient — with moderate ME/CFS makes at least a 1-level gain and goes back to work as a result of taking a C60 supplement.
Bob Beck Microbe Electrifier
• ME/CFS patient (intheknow) — with moderate ME/CFS recovered after 90 hours of treatment with a Bob Beck Microbe Electrifier connected across his wrists (2-level gain).
Nitrate Drugs
Nitrate drugs increase levels of nitric oxide in the body. These drugs are vasodilators typically given to relieve angina pains.
• ME/CFS patient (zzz) — experienced a 3-level gain going from severe ME/CFS to full remission in a matter of weeks after taking a single 10 mg dose of isosorbide dinitrate (a nitrate drug). That remission lasted for 8 years, but then relapse occurred after a minor surgery.
Statin Drug Atorvastatin
• ME/CFS patient (Hopefulone) — with moderate ME/CFS greatly improved after starting atorvastatin 80 mg daily.
Mitochondrial Cocktail
• ME/CFS patient (MrTwoToedSloth) — with moderate-to-severe ME/CFS went up to mild after taking a mitochondrial cocktail comprising Q10 300 mg, acetyl-L-carnitine, Na-D-alpha lipoic acid, nicotinamide riboside and a vitamin B complex for 3 months (1½-level gain).
Dr Kenny De Meirleir Protocol
• ME/CFS patient (sam.d) — with severe ME/CFS and who was not even able to speak, experienced a 1-level gain on a protocol prescribed by KDM. He became moderate, and able to do volunteer work from home. The KDM protocol included: Gammanorm (immunoglobulin IgG), breathing oxygen for 5 hours daily, vitamin B12 injections, and several other treatments.
Peptides LL-37 + BPC-157
LL-37 is a broad-spectrum antimicrobial peptide naturally made in the body. Anecdotally, supplemental LL-37 helps fix gut issues. BPC-157 is a peptide naturally found in the stomach which may promote healing and tissue regeneration.
• ME/CFS patient (beatsmyth) — with severe ME/CFS experienced a 2-level gain, moving up to mild ME/CFS, after taking a combination of two peptides LL-37 and BPC-157 for three months. He took 125 mcg of LL-37 daily for 6 weeks, then took a 2 week break, and then took LL-37 for another 6 weeks. This treatment also fixed his IBS.
ATP Injections
• ME/CFS patient (Keshav) — rapidly improved in a matter of days from ATP injections.
Daosin (Diamine Oxidase) Supplement
Daosin is a supplement providing diamine oxidase, an enzyme produced in the body to break down excess histamine.
• ME/CFS patient (xlynx) — with severe bedbound ME/CFS and a diamine oxidase deficiency greatly improved by taking the supplement Daosin.
High-Dose Sublingual Biotin
High-dose biotin (100 mg three times daily) has been used experimentally to treat multiple sclerosis. Ref: here.
• ME/CFS patient (BiotinJunkie) — found taking 10 mg of biotin sublingually several times daily worked well for his symptoms.
• One individual with autism (LouiseLouise) — found high-dose biotin 100 mg twice daily dramatically improved her autism.
Surgical Treatment of a Jawbone Cavitation Infection
Jawbone infections (osteomyelitis) can develop inside hollow pockets within the jawbone called cavitations. Cavitations may be left in the jawbone after a tooth extraction. Jawbone cavitation infections induce the inflammatory chemokine RANTES, as well as FGF-2, which are both linked to systemic disease.
A simple test for a jawbone infection is applying pressure with a finger on the gums to the jawbone beneath; if any area feels painful, this indicates a possible jawbone infection (though this method will not always detect jawbone infection). More reliable tests are MRI STIR scans and Cavitat scans. More info here.
• ME/CFS patient (Ian) — recovered from ME/CFS after surgically treating an infection within a jawbone cavitation.
• ME/CFS patient (ERROL_FARNHAMSURREY) — with mild ME/CFS made substantial improvements after treating a jawbone cavitation infection.
• ME/CFS patient (Dukey) — with moderate (housebound) ME/CFS got better after surgery to remove a jawbone cavitation infection (cavitational osteonecrosis).
Treating Nasopharynx Inflammation (in Vaccine-Triggered ME/CFS)
This thread details a published study in which patients with vaccine-triggered ME/CFS (or an ME/CFS-like illness) are cured or improved by treating their nasopharynx inflammation at the back of their nasal cavity with the topical anti-inflammatory zinc chloride.
• ME/CFS patient (DrFaust) — cured his ME/CFS using topical zinc chloride to treat his nasopharyngitis (nasopharynx inflammation).
Surgery for Craniocervical Instability
Craniocervical instability (CCI) is a looseness or laxity of the joint connecting the top of the spine with the skull. The Phoenix Rising CCI forum is here.
• ME/CFS patient (jeff_w) — was cured of his severe ME/CFS by surgery to fix his craniocervical instability (3-level gain).
• ME/CFS patient (JenB) — was cured of her ME/CFS by surgery to fix craniocervical instability, atlantoaxial instability and tethered cord.
• ME/CFS patient (Danielle) — with severe ME/CFS went into full remission (3-level gain) after C1-C2 fusion surgery for atlantoaxial instability, and surgery for occult tethered cord syndrome.
• ME/CFS patient (Karen) — had a major improvement after CCI fusion surgery.
Jawbone Realignment
The following two jawbone realignments were performed by Dr Amir, a dentist based in London:
• Patient with ME/CFS-like illness (Uzma Qureshi) — recovered after jaw realignment using dental appliances.
• Patient with ME/CFS-like illness (Hannah) — recovered after jaw realignment using dental appliances.
Tricyclic Antidepressants
Tricyclic antidepressants (TCAs) like amitriptyline increase the amount of serotonin and norepinephrine in the brain, and block the action of acetylcholine.
• Patient with ME/CFS or ME/CFS-like illness (RuralRick) — finds high doses of tricyclic antidepressants (TCAs) put his ME/CFS into remission.
Mild Hyperbaric Oxygen Therapy (mHBOT)
Mild hyperbaric oxygen therapy (mHBOT) is performed in a soft hyperbaric oxygen chamber that patients usually buy and keep in their home. Whereas regular hyperbaric oxygen therapy (HBOT) uses pressures up to 2 or 3 atmospheres, mHBOT pressures only go up to around 1.3 or 1.5 atmospheres.
• ME/CFS patient or possibly a post-viral fatigue patient (Jesse2233) — had a moderate ME/CFS illness that started with a viral infection, and lasted about 18 months before it went into remission. He had high antibody levels of 1:640 to coxsackie virus B4 on the ARUP lab tests.1 He went into remission (2-level gain) while doing mild hyperbaric oxygen therapy sessions daily in a home soft hyperbaric chamber, and credits his remission to mHBOT. (Although if it he had post-viral fatigue rather than ME/CFS, it may have resolved on its own anyway). He estimates he did over 200 hours of mHBOT.
• ME/CFS patient (used_to_race) — with mild-to-moderate ME/CFS associated with active EBV went into remission (1½-level gain) after two years of mild hyperbaric oxygen (mHBOT) sessions daily at 45 to 90 minutes each session. He also took hydroxychloroquine 400 mg daily during this time, so is not sure which led to his remission.
Pridgen Protocol (Famvir + Celecoxib)
The Pridgen protocol was devised by Dr William Pridgen as a means to treat the herpes simplex virus infections he believes may underpin fibromyalgia. This protocol is being experimentally used to treat ME/CFS as well. The protocol is based on the antiviral drug Famvir (famciclovir), to which the COX inhibitor celecoxib is added, as COX inhibitors are shown to have antiviral effects against herpes simplex.
• ME/CFS patient — improved substantially on the Pridgen protocol (normally Famvir 250 mg twice daily and celecoxib 200 mg twice daily) along with an antidepressant.
Consuming IgY Immunoglobulins From Chicken Eggs
• ME/CFS patient (Maj-Britt) — a Swedish women cured her Chlamydia pneumoniae-associated ME/CFS with a simple home treatment consisting of orally consuming IgY antibodies from a chicken egg yolk. She injected the chicken with her blood, so the chicken started making antibodies against the infections in her blood. Those chicken antibodies are naturally produced in large quantities in the eggs the chicken lays.
Yoga
Yoga is thought to up-regulate the parasympathetic nervous system. The newly-discovered link between ME/CFS and spinal/cranial conditions like craniocervical instability perhaps throws a light on why yoga might help some ME/CFS patients, given that many yoga asanas stretch and tone the spine and neck.
• ME/CFS patient (Sally) — with moderate ME/CFS recovered through yoga (2-level gain), according to a newspaper article.
• Patient with ME/CFS-like illness (Dan) — with symptoms like slurred speech and wild myoclonic jerks sending his limbs flying, went into near remission after doing lots of yoga.
Moving to Hot, Humid and Sunny Costa Rica
• ME/CFS patient (Paul) — with moderate-to-severe ME/CFS went into near remission (2-level gain) after 4 days of arriving in Costa Rica. On going back to his home in Canada, his ME/CFS quickly reappeared. But returning Costa Rica for a second time placed him back into remission, again after around 4 days of arriving. And previously, when Paul had a lingering post-viral fatigue after an infection, it was observed this was fully cured during a visit to Thailand (which is on the same latitude as Costa Rica, and with a similar hot and humid climate). Paul moved to Costa Rica permanently, in order to keep his ME/CFS in remission.
Active Prism Lenses To Treat Proprioception Dysfunction
Proprioception is a bodily sense deriving from receptors in our muscles which (without any visual clues) informs the brain of the current position of your limbs. People with poor proprioception find it hard to know where their limbs are, unless they look visually. One study observed a rapid recovery from severe ME/CFS after treating proprioception dysfunction with active prism lenses.
• ME/CFS patient (Donsboig) — moved from severe to moderate (2-level gain) using active prism lenses to treat his proprioception dysfunction.
Improving PEM
Post-exertional malaise (PEM) is the temporary worsening of ME/CFS symptoms which occurs after physical or mental exertion.
A useful thread detailing many treatments for PEM is found here. The PEM busters in that thread include: corticosteroids, Mestinon, cannabis, D-ribose, BCAA, Q10 and sodium bicarbonate.
Prednisolone
• ME/CFS patient (Hamsterman) — normally bedbound with severe ME/CFS found a one-off dose of 20 mg of prednisolone taken 30 minutes before a major exertion completely prevents PEM. He found taking prednisolone just before exercise allowed him to do a full workout at the gym without getting any PEM repercussion whatsoever. But he cautions that these doses of prednisolone should not be used daily, only occasionally, as the immunosuppressive effects of daily prednisolone will likely allow underlying viral infections to proliferate.
Cannabis
• Several ME/CFS patients — report cannabis is a good PEM shielder and PEM reliever: they find if cannabis is taken just when the first signs of PEM appear, at the first PEM "danger signals", then it will prevent the PEM from fully manifesting.
Mestinon (Pyridostigmine)
• ME/CFS patient (Mel9) — found Mestinon greatly reduced her PEM. Taking 30 mg of Mestinon once every four hours allows her to have a relatively active day (4 km walks).
• ME/CFS patient — with this illness for 28 years found Mestinon 180 mg per day eliminated her PEM, allowing her to do 3 mile runs and go to the gym without any PEM repercussion.
Improving Energy
MitoQ Supplement
MitoQ is a mitochondrially-targeted form of Q10. There is a lot of published research on MitoQ.
• ME/CFS patient (cigana) — finds that MitoQ significantly decreases his fatigue levels. He speculates his genetic A16V (rs4880) +/+ mutation, which results in lower levels of the mitochondrial antioxidant Mn-SOD, may explain why he gets substantial benefit from MitoQ. So those with an A16V +/+ mutation might consider trying MitoQ. However, later he concluded that this energy boost only appeared when he took GcMAF at the same time as MitoQ.
Dichloroacetate (DCA)
Dichloroacetate in ME/CFS studies was found to stimulate mitochondrial energy metabolism, and improve fatigue, brain fog and pain in about one-third of patients (but the study found those with comorbid autoimmune conditions are less likely to respond to DCA). Refs: 1 2 See these tips for avoiding the possible neuropathy side effects of DCA.
• ME/CFS patient (XenForo) experienced "a lot more energy" from DCA.
Cellfood (Deuterium Sulfate)
The active ingredient in Cellfood is deuterium sulfate, a form of sulfuric acid based on the hydrogen isotope deuterium (formula D2SO4). Deuterium sulfate is claimed to have an enzymatic action which improves tissue oxygenation and reduces oxidative stress.
• ME/CFS patient (Mary) — found the supplement Cellfood 10 drops three times daily increased her energy.
Improving Brain Fog
Vitamin B12 Injections / Transdermal B12 Oils
• ME/CFS patient (Hip) — found the B12 transdermal oils formulated by Dr Greg Russell-Jones in Australia help improve brain fog.
Piracetam
• ME/CFS patient (Hip) — found piracetam 800 mg daily helps improve brain fog.
Improving Sound or Light Sensitivity
Very Low-Dose Amisulpride
• ME/CFS patient (Hip) — finds the dopamine system stabilizer drug amisulpride in very low-doses reduces sound sensitivity (hyperacusis), and has several other beneficial effects on ME/CFS symptoms.
Improving Emotional/Stress Sensitivity
Hydrogen-Rich Water
Hydrogen-rich water is made by dissolving hydrogen gas into water under pressure. HRW known to stimulate the release of the hormone ghrelin, which in turn stimulates the hypothalamus. The H2 molecule within HRW is also an antioxidant.
• ME/CFS patient (Hip) — found hydrogen-rich water noticeably reduces the emotional sensitivity / stress sensitivity symptom of ME/CFS.
Improving Gut Health, IBS and SIBO
Chloramine Avoidance
Chloramine is a disinfectant added to the drinking water in some regions. Chloramine can be irritant to the mucous membranes. Note that chloramine is not the same as chlorine, and carbon water filters do not remove chloramine.
• ME/CFS patient (Hip)— substantially improved his IBS-D by removing chloramines from his tap drinking water, which is done by adding a pinch of ascorbic acid (vitamin C) powder to the water, as this reacts with and neutralizes the chloramine.
Improving the "Wired but Tired" Hyperarousal
Useful thread: Five ways to reduce your ME/CFS "wired but tired" hyperaroused brain state
Treating Anxiety
N-Acetyl-Glucosamine
• ME/CFS patient (Hip) — was able to eliminate his moderate-to-severe generalized anxiety disorder with a set of supplements including N-acetyl-glucosamine (NAG). Many other ME/CFS patients with anxiety who tried these supplements also observed a major reduction in anxiety levels, so this is a tried and tested treatment.
Prebiotics
Prebiotics are food which feed friendly bacteria in the gut, but which bad bacteria cannot eat.
• ME/CFS patient (Hip) — found prebiotics such as inulin and FOS greatly reduced anxiety levels and improved mood.
Treating Depression
Saffron
• ME/CFS patient (Hip) — finds Spanish saffron 100 mg quite helpful for depression. Antidepressant effects kick in within an hour or so of taking it. One systematic review found saffron to be as effective as standard pharmaceutical drugs. But watch out for fake saffron.
Treating Headaches or Migraines
Trimetazidine
Trimetazidine is a drug which improves myocardial glucose utilization.
• ME/CFS patient (Hip) — finds a single dose of trimetazidine 40 mg eliminates his normally 3-day long headaches within 12 hours, and if taken at the initial signs of headache, prevent the headache from manifesting in the first place.
Improving Sleep
CBD Oil
• ME/CFS patient (Iquitos) — finds taking 15 drops of cannabidiol (CBD) oil allow him to sleep much better.
Melatonin
• ME/CFS patient (Hip) — finds taking melatonin 2 hours before planning to go to bed helps get him to sleep, and helps prevent the sleep cycle inversion of ME/CFS (where you are awake very late at night, and sleeping during day), and stops his non-24 (where you keep going to bed later and later as the days progress).
• ME/CFS patient (Hip) — finds when you are go to bed but find you are still awake an hour or so later, and cannot get to sleep, getting out of bed and performing 80 squats in rapid succession (which takes about 80 seconds) in order to exhaust the leg muscles and generate some lactate, is a remarkably effective way (almost infallible) of getting to sleep. After performing the squats and going back to be, he finds he then goes to sleep within 5 minutes.
• ME/CFS patient (SpiralOut) — finds when using Luminette glasses for several hours daily, which provide the equivalent of 10,000 lux of light to the eyes, it completely fixes his non-24 sleep issues (non-24 is where each day you go to bed later than the day before, because your circadian rhythm does not match the normal daily 24 hour cycle).
Relieving Pain
Low-Dose Naltrexone (LDN)
• ME/CFS patient (Wishful) — finds LDN works very well to relieve his ME/CFS body aches, which he thinks may be neuropathic pain.
Improving the "Molasses" Heavy Limbs Feeling
Far Infrared Heat
• ME/CFS patient (Hip) — finds far infrared heat on his back for several hours a day reduces the heavy limb feeling of ME/CFS, perhaps by its anti-inflammatory effects on the spine (as he speculates spinal ganglion inflammation might cause the heavy limb feeling).
![]()
Phenytoin
From: Reviving the Broken Marionette: Treatments for CFS/ME and Fibromyalgia
Phenytoin is believed to act by modulating glutamatergic transmission. It has been in clinical use as an anticonvulsant for over 50 years, but it is also an antiarrhythmic similar to lidocaine and mexiletine. It has analgesic, anxiolytic and mood stabilizing properties. Jay Goldstein has used it to treat CFS/ME and fibromyalgia in a low dose of 100 mg a day.62 He reports synergistic effects from combining it with gabapentin.
Phenytoin may also help tinnitus.63
Phenytoin is generally thought to have adverse effects on cognition, but this may only apply to the large doses used to treat epilepsy. Smaller doses have even been shown to positively influence cognition.64 In one study phenytoin was found to cause a significant increase in right brain volume in patients with PTSD.65
The most common side effects include tiredness, nausea, ataxia (impaired coordination), nystagmus, dizziness and tremor. Phenytoin may reduce the blood levels of folic acid, biotin, calcium, vitamins B1 and B12, vitamin D, vitamin K and carnitine, but folate also decreases blood levels of the drug. Phenytoin can also interact with a number of different medications, including many antibiotics, anticoagulants, azoles, opiates, benzodiazepines, other anticonvulsants and oral contraceptives.
Phenytoin is available virtually everywhere and it is very inexpensive. It can be used topically as an analgesic, but this form is not commercially available and must be compounded
![]()
What is meldonium and why was it banned
https://www.wionews.com/sports/what-is-meldonium-and-why-was-it-banned-33353
Meldonium is used to treat ischaemia: A lack of blood flow to parts of the body, particularly in cases of angina, chronic heart failure, cardiomyopathy and other cardiovascular disorders.The drug also helps to adjust the body's use of energy and can boost stamina and endurance. It increases blood flow, which improves exercise capacity in athletes and increased blood flow means more oxygen to muscle tissue
Please also see links page
![]()
Psilopcybin and neuroplasticity is a topic I will review and update the site with
![]()
Lithium side effects can include fatigue. In some patients it has shown to combat fatigue. There are two types of medicinal Lithium Lithium is prescription and Lithium is otc. It may help CFS (page 3), TBIcf alttherapy (59) and OCD (68), supplements (8
![]()
therapeutic treatment of long covid as applied to chronic fatigue syndrome
List (click to open) click again to close
• Take frequent short rest breaks (559)
• Spend time in low-stimulation environment (198)
• Rest (572)
• Personal development (e.g. learn to say 'no', care less about opinion others, letting go of shoulds and musts, acceptance, become more relaxed and balanced) (450)
• Wheelchair (66)
• Ignore people who think ME/CFIDS is not real (363)
• Low-Dose Naltrexone (LDN) (89)
• Avoid biotoxins (82)
• Complete stillness & quiet (154)
• Diet changes (509)
• Avoid known allergens (149)
• Meditation (343)
• Gluten-free diet (250)
• Eliminate/ reduce sugar (399)
• Change job (212)
• Adequate rest (49)
• Avoid alcohol (442)
• Methylation treatments (74)
• Adequate sleep (49)
• Yeast treatments (125)
• T3 (58)
• "Recuperation" (55)
• Relaxation techniques (156)
• Avoid mold (168)
• Mindfulness (141)
• Eliminate/ reduce dairy (366)
• Perrin Technique (10)
• Inverting body position (with head down and feet up eg on a couch) (180)
• High Dosage VegEpa (EPA+EPO) (15)
• Do absolutely Nothing (168)
• B12 injections (205)
• Anti-yeast diet (65)
• Inner Spirit Therapy (12)
• Diaphragmatic breathing (221)
• Far Infrared Heat (Migun Bed) (58)
• Go to bed early and sleep longer (448)
• Marijuana (6)
• Massage (371)
• Thyroid hormone (59)
• Probiotics (402)
• Stay well-hydrated throughout the day (469)
• Oxytocin (20)
• Beta Blockers (for OI) (15)
• ketogenic diet (10)
• Betahistine (3)
• Physiotherapy (Connective Tissue Release) (6)
• Revitalizing Sleep Formula (14)
• Mobic (14)
• Energy Revitalization System vitamin powder (14)
• paleo/primal diet (22)
• Magnesium (oral) (374)
• Gupta Amygdala Retraining (49)
• Reiki (39)
• SHINE Protocol-Dr. Teitelbaum (23)
• Ayurveda (37)
• Orthomolecular Therapy (18)
• Chelation treatments (49)
• Lymphatic Massage (61)
• Sinus Surgery (6)
• Qigong (53)
• Co-codamol (27)
• Eat more vegetables and fruits (467)
• Liposomal Glutathione (31)
• vegetarian diet (19)
• horseback therapy (4)
• Lithium orotate (4)
• Atlas Profilax (4)
• Emotional Freedom Technique (EFT) (68)
• EECP (1)
• Adya Clarity Shots (1)
• bowel removal for cancer (1)
• MAF 878 (1)
• clarithromycin & hydroxychloroquine (1)
• Nicotinamide Riboside (1)
• carbidopa/levadopa (1)
• Clonazepam (Klonopin, Rivotril) (167)
• Stretching (414)
• Diflucan\--antifungals (33)
• Crystal Light Therapy (5)
• B vitamins (458)
• Cranio-Sacral Therapy (94)
• in-home treatment mobility exercises (2)
• ketotifen (2)
• fluefenazine/nortriiptiline clorhidrate (2)
• Proamatine (2)
• Earthing (18)
• Xanax (alprazolam) (92)
• Nexavir (9)
• Nystatin (22)
• Antivirals (84)
• carnitine (6)
• Theta Healing (6)
• Adrenal Stress End (16)
• Robaxin (3)
• Interferential TENS (13)
• Cordyceps (13)
• Sinus Treatments (Nasonex, etc) (66)
• Betaine-HCl (67)
• Transfer Factors (7)
• Malic Acid (153)
• Antihistamines (drowsy / first generation) (14)
• Stimulants (dextroamphetamine, amphetamine, Adderall, etc) (96)
• Horizant (1)
• alpha - gpc (1)
• Siffrol (1)
• Kavinace (1)
• Mirapex (1)
• Nimodipine (1)
• Aqua Flora for yeast (1)
• Azilect (1)
• desmopressin (1)
• Ampligen (8)
• Rebreathing carbon dioxide (8)
• Myer's Cocktail (43)
• Magnesium (topical) (76)
• Electrolyte beverage (eg. gatorade) (170)
• Guainfenesin (59)
• Rheumatrex, Trexall (methotrexate) (9)
• NAET for allergies (9)
• Acetyl-L-carnitine (166)
• Osteopathy (76)
• Pinecone Extract (ImmunExtra) (6)
• Vitamin D (424)
• Reverse Therapy for CFS (10)
• Baclofen (29)
• Ibuprofen (Advil, Motrin) (384)
• IVIg infusions (4)
• Zeolith (4)
• Famvir (4)
• Red Marine Algae (8)
• Theanine (16)
• Neurofeedback (28)
• Testosterone (94)
• Sublingual B12 (212)
• Root canal/cavitation removal (107)
• thyroid operation (1)
• MCT oil (1)
• ice baths (1)
• Phenocane (1)
• NAC (42)
• Hypnotherapy (26)
• Glucosamine/Chondroitin (84)
• Mushroom Extracts (AHCC, Shitaake) (18)
• Specific Carbohydrate Diet (SCD) (18)
• gardening/nature (35)
• Hyperbaric Oxygen (10)
• Cerefolin (folate, B12 & NAC) (53)
• Azathioprine (2)
• Cannabidiol (CBD) (2)
• Valcyte (2)
• UVA-URSI (11)
• Yoga (263)
• Helminthic Therapy (7)
• UltraClear products (12)
• Acupuncture (278)
• Xyrem/GHB (13)
• ALA (50)
• Armour Thyroid (4)
• Coenzyme Q10 (332)
• Omega 3 (fish oil) (393)
• Ultram (tramadol) (98)
• D-Ribose (103)
• Bioidentical estrogen (19)
• Petrovic Protocol (5)
• Omega 3,6,9 (352)
• Iron (54)
• Afipran (1)
• Sauna (1)
• GcMAF (6)
• Taurine (11)
• Lamictal (11)
• Ubiquinol (46)
• Ionized Water (56)
• Naproxen (Aleve) (146)
• DHEA (62)
• Chinese herbs (123)
• NK stim supplements (7)
• Oxymatrine (7)
• Isagenix (7)
• EPA-DHA (59)
• Acetaminophen / Paracetamol (Tylenol, Panadol) (344)
• Kinesiology (45)
• Licorice Root Extract (40)
• Savella (3)
• Vicodin (hydrocodone) (3)
• Chiropractic (234)
• L-Carnitine (203)
• Valtrex (14)
• Bioidentical Hormones, i.e. progesterone (36)
• Homeopathy (194)
• vegan diet (9)
• Non-sedating antihistamines (137)
• Fentanyl patch (15)
• Urine Therapy (4)
• Ritalin (43)
• 5-HTP (83)
• Iodine (58)
• Distract your attention away from the symptoms (417)
• Mickel Therapy (6)
• Immunovir (isoprinosine, inosine pranobex) (24)
• Ganciclovir (7)
• Moclobemide (1)
• Catapres (clonidine) (14)
• Skin brushing (71)
• Melatonin (319)
• Formula 3030 (2)
• Cool shower following exertion (93)
• Detox Foot Baths with mild electric current (36)
• Wheat Germ Extract supplements (Avemar) (3)
• NADH (112)
• DMG (25)
• GABA (Gamma Amino Butyric Acid) (33)
• Pregabalin (5)
• Sophora root (5)
• Antibiotics (217)
• Vitamin C (lypo spheric) (71)
• Psychotherapy (non CBT) (175)
• Pall Protocol (13)
• Fresh Vegetable Juices (88)
• Cortef (hydrocortisone / synthetic cortisol) (83)
• Green Smoothies (green vegetables and fruit) (68)
• MSM (53)
• Brainwave audio CD's (69)
• Aspirin (169)
• Cortisol (compounded) (16)
• Propranolol (beta-blocker) (8)
• Sodium Valproate (9)
• Doxycycline (43)
• Beta-interferon (1)
• Heparin (1)
• MAF 314 (1)
• Piracetam (1)
• Metanx (1)
• Hydrotherapy (1)
• Raw food diet (27)
• Bowen Technique (10)
• Lansoprazole (11)
• Soak feet in cold water (44)
• Cats Claw - Uncaria Tomentosa (55)
• Reishi mushrooms (26)
• Lightning Process (16)
• Rolfing (27)
• Whey Protein supplements: (Immunopro/ Immunocal) (38)
• bicycle with power options (8)
• Vitamin E (96)
• AllicinPlus (active garlic capsules (64)
• Flaxseed oil (44)
• Hot baths (10)
• Antiretrovirals (10)
• ativan (11)
• Inosine (30)
• Tai Chi (104)
• Calcium (63)
• Vitamin A (67)
• Florinef (fludrocortisone) (17)
• Lyrica (26)
• Hot showers (12)
• Gingko Biloba (88)
• Marshall protocol (12)
• Provigil (modafinil) (124)
• SAM-E (104)
• Olive Leaf Extract (46)
• Cognitive Behavioral Therapy (CBT) (205)
• Orthostatic conditioning/exercise (65)
• Doxylamine (Unisom) (41)
• Undenatured whey protein (80)
• Monolaurin (e.g., Lauricidin) (37)
• Celexa, Cipramil (citalopram) (114)
• Diphendydramine (Unisom, Benadryl) (161)
• Atenolol (beta blocker) (36)
• Rebounder (32)
• Trazodone (92)
• Cymbalta (duloxetine) (138)
• Neurontin (gabapentin) (149)
• Wellbutrin (bupropion) (149)
• Caffeine (378)
• Mild/ moderate exercise (577)
• Amitriptyline (Elavil) (113)
• Regular exercise program (208)
• Effexor (venlafaxine) (136)
• SSRIs total(Prozac, Effexor, Celexa) (224)
• Zoloft (sertraline) (148)
• Prozac (fluoxetine) (164)
• Paroxetine (Paxil, Seroxat) (118)
• Alcohol (229)
• Graded Exercise Therapy (GET)
CHRONIC FATIGUE SYNDROME: A TREATMENT GUIDE, 2nd Edition
AMPLIGEN
DESCRIPTION. Ampligen (poly I:poly C12U) is a mismatched double-stranded RNA (ribonucleic acid) with immodulatory and antiviral properties. Because Ampligen has not yet been approved by the Food and Drug Administration (FDA), its use to date has been experimental.
BACKGROUND. In the early 1980s, a molecule called Poly(I)-Poly(C) was discovered to inhibit tumor growth and stimulate interferon production. As a result, it was used in a number of cancer trials. However, it was found that the substance made patients quite ill with serious side effects. While Poly(I)-Poly(C) was extremely toxic, the toxicity decreased significantly when the structure of the RNA was altered. Fortunately, the effectiveness of the new substance (Ampligen) was not diminished, despite the change in structure.
In 1987 Ampligen was used experimentally in a small group of patients with AIDS (acquired immunodeficiency syndrome). The positive results of this trial seemed to confirm the claim that Ampligen works by enhancing natural killer cell function and influencing the 2-5A synthetase pathway. This pathway is vital in the defense against viral infections. According to Dr. Robert Suhadolnick of Temple University in Philadelphia, there are defects in key components in the antiviral system in some CFS/ME patients, the most notable of which are low latent 2-5A synthetase and upregulated RNase (ribonuclease) L activity (Journal of Interferon and Cytokine Research, 1997). Ampligen is thought to correct both of these defects.
USES IN CFS/ME. In August 1988, Dr. Daniel Peterson, a pioneer in CFS/ME treatment, was the first physician to use Ampligen on an extremely ill patient with CFS/ME. Because of the severity of the patient's illness, Dr. Peterson was able to obtain permission from the FDA to use Ampligen under compassionate care status. The results were impressive and encouraging. One year into therapy the patient had recovered near-normal function in some areas and demonstrated a 46-point increase in IQ. This justified the next pilot study by Dr. Peterson, as well as several other formal studies conducted independently.
At the 1990 CFIDS Conference in Charlotte, North Carolina, and at the Cambridge Symposium, Dr. Peterson reported positive results after treating 15 patients with Ampligen. At the end of 24 weeks, most of the patients demonstrated increased performance status (using Karnofsky scores) and exercise tolerance (as measured by treadmill testing). Cognitive improvement was demonstrated by improved memory and increased IQ scores. No significant toxicity was reported. Ampligen's antiviral properties were confirmed by evidence that human herpesvirus 6 (HHV-6) reactivation was absent after treatment and abnormal components of the 2-5A pathway returned to normal range. It is of interest that of the two or three patients who did not respond to Ampligen therapy, the only significant pretreatment difference was measurable differences in 2-5A synthetase pathways.
The encouraging results of Dr. Peterson's study paved the way for a larger FDA-approved double-blind study in 1991 involving 92 patients in four U.S. cities. Again the results were encouraging. Many of the participants had been severely disabled before treatment and required assistance for simple daily activities. More than half of those in the study who received Ampligen demonstrated improvement and many were able to carry out daily activities with minimal assistance.
A study in Brussels, Belgium, presented at the 1996 American Association for Chronic Fatigue Syndrome (AACFS) Conference, to evaluate the safety and efficacy of intravenously administered Ampligen also showed encouraging results. Eleven patients with myalgic encephalomyelitis (ME) were given intravenous Ampligen twice a week for 24 weeks. The Belgian physicians reported that at the end of 24 weeks, all 11 experienced some improvement. In addition, no adverse effects to treatment were noted. These positive results paved the way for expanded trials. It was hoped that with an expansion of clinical trials to Canada and Belgium, and Ampligen's subsequent approval for Canada's Emergency Drug Release Program, that the drug would soon be approved for use in the U.S.
Unfortunately, since 1996 little progress has been made in obtaining FDA approval of the drug. A seemingly endless series of lawsuits, missed deadlines and administrative setbacks effectively quashed the widespread support the drug had enjoyed in the 90s. To cap the matter, in 2009, after the completion of Phase III of Ampligen's drug trials, the FDA refused to grant Ampligen “new drug,” status which, in effect, relegated Ampligen once more to clinical trials.
PROTOCOL. Because this drug is still, after more than twenty years, in the trial phase, treatment protocols are still evolving. Ampligen is quite fragile, which makes administration difficult (it must be given intravenously). Two intravenous injections a week of 400 mg are given over a 6- to 12-month period, though some doctors recommend a course of treatment up to 18 months for more severely ill patients. Longer courses of treatment seem to produce longer lasting results.
PROS. No other drug has received more attention from the CFS/ME community than Ampligen. But even in the wake of delays, reversals and lawsuits, many doctors still defend Ampligen as the most effective drug for those patients who have acute viral onset, persistent herpesvirus infections, depressed natural killer cell function, and 2-5A synthesase/RNase L up-regulation. For those who have been bedridden for years, who are confined to wheelchairs, and whose lives have lost all semblance of normality,Ampligen may be a godsend, and the frustration of those who have experienced a return to a functional life during Ampligen trials, only to have it taken away again at the end of the trial, is more than justified.
Dr. Kenny DeMeirleir claims that close to 80% of his patients reported “complete clinical recovery” after taking an extended course of treatment. Patients report improvement in overall function, energy levels, cognitive performance, and some have been able to return to work. Dr. Lapp, who has been using Ampligen since 1998, reports significant improvement in 50% of his severely ill patients. It is important to note that while few doctors claim that Ampligen works for the majority of their patients, it seems to have a very positive effect on a subset of those who are the most seriously ill, and that, in and of itself, provides a good reason for Hemispherx to pursue Ampligen's final approval.
CONS. Although test results are encouraging, it is important to note that Ampligen is not a surefire cure. The percentage of patients who demonstrate substantial improvement with the drug has yet to be determined. Side effects are common. Although Hermispherx maintains that Ampligen is generally well tolerated, patients have reported diarrhea, constipation, flushing, temporary vision loss, muscle aches, depression, loss of libido, dizziness, chills, fever, malaise, anxiety, and loss of energy.
Dr. Peterson reported at the 1990 CFIDS Conference that some patients experienced an interferon-like reaction, with headaches, myalgias, and, rarely, hair loss. A puzzling effect noted by Dr. Paul Cheney was that although patients report overall lessening of symptoms, particularly cognitive symptoms, they do not necessarily equate this lessening of severity to “feeling good” (CFIDS Chronicle, Physicians Forum, 1991). Side effects usually subside after several months, but that may be too long for many patients to endure.
AVAILABILITY AND COST. As of 2011, Ampligen is available only at Dr. Lapp's Hunter-Hopkins clinic in Charlotte, NC, and Dr. Peterson’s Lake Tahoe clinic under an open-label trial. (An open-label trial is one in which all patients receive, and pay for, the drug.) Dr. Bateman’s Fatigue Consultation Clinic in Salt Lake City and Dr. Enlander's clinic in New York have also begun to seek recruits for an open-label trial. Hemispherx is planning to add several other sites around the U.S., as well as sites in Mexico and Argentina. In July 2012, Hemispherx announced that it had submitted a new drug application to ANMAT (Administracion Nacional de Medicamentos, Alimentos y Tecnologia Medica), the agency responsible for the national regulation of drugs, foods and medical technology in Argentina, under the ANMAT's Orphan Drug regulations.
Ampligen is quite expensive. A single infusion costs $150. At two infusions a week, that amounts to $1200 per month. Additional costs, such as medical visits, lab work and the administration of the infusions, can amount to $1000 a month. Altogether, one year of treatment will cost over $24,000. Patients must pay for the cost of the treatment because Ampligen is available on a cost recovery basis only. Some insurers will reimburse for administration costs and lab work, which can save roughly $12,000 a year. Medicare does not cover any expenses for investigational therapies.
MORE INFORMATION
The Hunter-Hopkins Center's report from the 9th Hemispherx Biopharma investigators meeting. Quite technical but very thorough: http://www.drlapp.net/meLetterMar2011.htm
NIH webpage on clinical trials. Shows current status of Ampligen trials. http://www.clinicaltrials.gov/ct2/show/NCT00215813?term=00215813&rank=1
Informative thread on patients' experiences with Ampligen. http://forums.phoenixrising.me/showthread.php?12999-Ampligen-Experiences
Dr. Lapp's Ampligen protocol: http://www.drlapp.net/ampligen.htm
Hemispherx Biopharma's page on Ampligen. http://www.hemispherx.net/content/rnd/drug_candidates.htm
A fascinating blog written by a New Zealand journalist who moved to the U.S. to participate in an open-label Ampligen trial: http://ampligen-treatment.blogspot.com/
San Francisco Ampligen trial (with prices): http://phoenixrising.me/forums/showthread.php?12305-Ampligen-Treatment-Study-(AMP-511)-starting-in-San-Francisco-Bay-Area
ProHealth's history of Ampligen: http://aboutmecfs.org.violet.arvixe.com/Trt/AmpHist.aspx
Cort Johnson's up-to-date news on the status of Ampligen: http://phoenixrising.me/archives/8819?utm_source=newsletter+subscribers&utm_campaign=9dd3ad21ce-April_Newsletter4_28_2012&utm_medium=email
ANTIBIOTICS
DESCRIPTION. Antibiotics (derived from the Greek anti meaning 'against', and bios meaning 'life') are substances that either kill microbes or inhibit their growth.
BACKGROUND. As with so many monumental discoveries, antibiotics are the result of a mistake. In 1928, Alexander Fleming, a brilliant (but messy) Scottish biologist, was investigating the properties of the bacterium staphylococcus. He had left his samples piled up on a bench before going away on holiday. When he returned, he discovered that one of the petri dishes had been invaded by mold, and that the bacteria that had come into contact with the mold had died. After overcoming his initial annoyance, Fleming realized that he had stumbled across a remarkable substance. He named it penicillin.
Since Fleming's remarkable discovery, antibiotics have become an integral feature of modern medicine. Their ability to kill bacteria and protozoa has saved millions of lives worldwide, making them one of the medical miracles of our time. However, Fleming noted that when antibiotics were used at too low a dose, or for too little time, the bacteria would become resistant. With the passage of time, it turned out that bacteria become resistant even with the proper administration of antibiotics. (Any microbe will adapt to a changing environment, producing, in the end, a stronger version.) This has led to the development of ever-stronger antibiotics, which, inevitably, have produced “super bugs” – bacteria which are resistant to all antibiotic therapy.
Basically, antibiotics kill bacteria by inducing oxidative stress. This is the same mechanism through which many parts of the immune system kill bacteria. Given the fact that bacteria are living organisms, it should not come as a surprise that bacteria utilize many of the same mechanisms to protect themselves from oxidative stress as do other cells. A recent study led by Evgeny Nudler, a professor of biochemistry at New York University, showed that nitric oxide (NO) produced by bacteria neutralizes many antibacterial compounds. By using NO's ability to destroy attackers, bacteria cleverly employ the body's own defense mechanisms to ward off the effects of antibiotics.
USES IN CFS/ME. The idea that CFS/ME is caused by a “bug” is not a new one. As early as the 1930s it was thought that CFS/ME (then called “atypical polio”) was caused by an enterovirus. The close association with Epstein-Barr virus (EBV) and other endemic viruses, as well as well-documented high levels of viral markers in CFS/ME patients, has led researchers to conclude that the illness is caused by a virus. However, a small, but significant, number of researchers has proposed the active involvement of bacteria in the development of CFS/ME.
One of the first researchers to propose a causal role for bacteria was Garth Nicolson. Nicolson found that both CFS/ME and Gulf War Syndrome (GWS) patients were infected with mycoplasma. (Mycoplasma are bacteria that lack a cell wall, and are thus impervious to many antibiotics). Nicolson proposed that ongoing mycoplasma infections were responsible for many immunological anomalies associated with both CFS/ME and GWS. He successfully treated GWS and CFS/ME patients with long courses of different antibiotics to eradicate mycoplasma infections. In a subsequent study, Nicolson found that many patients diagnosed with CFS/ME were subsequently diagnosed with Lyme Disease, which is caused by a rickettsial bacterium.
Several fascinating studies have indicated a causative role for rickettsial and chlamydial bacterial infections in CFS/ME. Phillipe Bottero, a French doctor practicing in Paris, found that all of his CFS patients tested positive for bacterial infections. An impressive 78.5% of Bottero's 98 CFS patients improved significantly after treatment with antibiotics. (His article is in Chronic Fatigue Syndrome: Critical Reviews and Clinical Advances). A smaller second group, composed of patients diagnosed with ADHD, schizophrenia and autism also showed a similar rate of improvement. Bottero proposed that due to the long survival of rickettsial infections in vascular linings, the resulting vasculitis could produce many of the symptoms common in CFS/ME.
Cecile Jadin, a Belgian surgeon, also found strong correlations between rickettsial infections and patients diagnosed with CFS/ME. Jadin reversed symptoms in five hundred patients previously diagnosed with CFS, FM, MS, depression, heart disease, and psychosis with a simple course of tetracycline.
In 2009 Frykholm found that ninety days of treatment with antibiotics, combined with vitamin B injections, cured one of his CFS/ME patients. When two patients with long-standing and incapacitating CFS/ME came to his clinic in 2007 he treated them both with antibiotics. After sixty days the first showed excellent improvement which continued on follow-up one year later, whereas the second, who also took antibiotics for sixty days, showed a significant improvement. While studies of this kind may ultimately raise more questions about the process of diagnosis than to etiology, it is nonetheless interesting to consider the role that bacterial infections play in perpetuating, if not causing, CFS/ME.
In the 1990s, Luther Lindner, a pathologist at Texas A&M, believed he had found the elusive agent that was the cause of CFS/ME, as well as other autoimmune diseases. While examining the blood of an MS patient, he found a novel bacterium. Lindner then identified the bacterium in the blood of patients with CFS/ME. Though the prospect of having discovered a potential cure for the illnesses was exciting, Lindner was cautious in his treatment recommendations. For while he noted good short-term response in CFS/ME patients, he also noted that the new strain was highly resistant to antibiotic treatment. Lindner cautioned against the use of antibiotic regimens without monitoring the number of organisms present. Paradoxically, he also found that “antibiotics can actually stimulate bacterial growth and make the patient worse.” He added that this can usually be predicted by sensitivity testing. Indeed, Lindner's theories may be borne out by the significant number of CFS/ME patients who report having taken long courses of antibiotics before falling ill.
An entirely different role for antibiotics as a CFS/ME treatment was explored by Vermeulen and Scholte. In their retrospective study of 99 CFS/ME patients, 58 patients reported a decrease in symptoms after taking azithromycin. All of the responding patients had low levels of acetylcarnitine. The authors concluded that “the efficacy of azithromycin in the responsive patients could be explained by the modulating effect on a chronic primed state of the immune cells of the brain, or the activated peripheral immune system. Their lower acetylcarnitine levels may reflect a decreased antioxidant defense and/or an increased consumption of acetylcarnitine caused by oxidative stress.” In short, the azithromycin was functioning as an immune system modulator in these cases, rather than as a bactericide.
PROTOCOL. Most CFS/ME physicians prescribe antibiotics when there is a clear indication of a bacterial infection. However, there are some protocols that involve low-dose antibiotics as part of an overall treatment strategy. The Marshall Protocol uses pulsed low-dose antibiotics to treat CFS/ME even in the absence of an active bacterial infection.
Dr. Teitelbaum also uses antibiotics to treat hidden infections. These are indicated if the patient has chronic lung congestion, low fever, recurrent scalp sores, a history of a bad reaction to other antibiotics, transient improvement with antibiotics, vertigo, and severe night sweats. In these instances, Dr. Teitelbaum assumes the presence of a bacterial infection that may be difficult to detect (e.g., Lyme, mycoplasma, chlamydia) and recommends a long course of antibiotics. Dr. Nicolson's course of antibiotic treatment can last as long as two years.
PROS AND CONS. CFS/ME patients report that antibiotics of various kinds can both exacerbate and improve symptoms. Common side effects include nausea, “brain fog”, and GI disturbances. Most CFS/ME patients find that they do better “pulsing” with low-dose antibiotics, and that longer courses of treatment are either ineffective or cause relapse. Some report that after initial “miraculous” improvement, they became much worse. A small number of patients have reported dramatic improvement.
FURTHER READING
“Study explains bacteria's resistance to antibiotics.” AFP Sept 13, 2009. http://www.google.com/hostednews/afp/article/ALeqM5jbBIAufNyKV0owj4rc08LmSA5GKg
Technical article explaining the mechanisms of antibiotics http://www.bu.edu/abl/files/nrm_kohanski.pdf
Garth Nicolson's article on the role of bacterial infections in CFS/ME and Gulf War Syndrome. http://www.immed.org/illness/fatigue_illness_research.html
Garth Nicolson's antibiotic protocols http://www.newtreatments.org/doc/Mycoplasma/12
Good summary of Nicolson's theories and protocols http://www.rense.com/general7/microplasm.htm
Doris Jones proposes that antibiotics may be the cause of CFS/ME. http://www.prohealth.com/fibromyalgia/blog/boardDetail.cfm?id=1015520&b1=CHWEBO
Ringing in ears caused by minocycline http://forums.phoenixrising.me/showthread.php?9291-Minocyclin
Article on Luther Linder's research: http://ottem.org/ccca/news/newsletters/vol16-1.htm
Luther Lindner's explanation of why antibiotics might potentially make CFS/ME worse. http://www.thisisms.com/forum/antibiotics-f28/topic572.html
Marshall Protocol and pulsed, low-dose antibiotics http://mpkb.org/home/protocol/mp_antibiotics
Dr. Teitelbaum on the use of antibiotics in CFS/ME http://www.endfatigue.com/health_articles_f-n_2/Infections-treating_hidden_antibiotic_cfs_fm.html
RESEARCH
Frykholm BO. “On the question of infectious aetiologies for multiple sclerosis, schizophrenia and the chronic fatigue syndrome and their treatment with antibiotics.” Med Hypotheses. 2009 Jun;72(6):736-9. http://www.ncbi.nlm.nih.gov/pubmed/19269110 (Abstract)
Nicolson, Garth L, Nancy L. Nicolson, and Joerg Haier. “Chronic Fatigue Syndrome Patients Subsequently Diagnosed with Lyme Disease Borrelia burgdorferi:
Evidence for Mycoplasma species Co-Infection.” Journal of Chronic Fatigue Syndrome. 2008; 14(4): 5-17. http://www.lymepa.org/Chronic%20Fatigue%20Syndrome%20patients%20subsequently%20diagnosed%20with%20Lyme%20disease%20and%20coinfections.pdf
Vermeulen RC, Scholte HR. “Azithromycin in chronic fatigue syndrome (CFS), an analysis of clinical data.” J Transl Med. 2006 Aug 15;4:34. http://www.ncbi.nlm.nih.gov/pubmed/16911783(Abstract)
PATIENT REVIEWS
CFS/ME patient reviews of doxycycline: http://www.revolutionhealth.com/drugs-treatments/rating/doryx-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Zithromax: http://www.revolutionhealth.com/drugs-treatments/rating/zithromax-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Biaxin: http://www.revolutionhealth.com/drugs-treatments/rating/biaxin-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of minocycline: http://www.revolutionhealth.com/drugs-treatments/rating/minocin-for-chronic-fatigue-syndrome-cfs-cfids-me
BOOK
Patarca Montero, Roberto and Kenny De Meirleir. Chronic Fatigue Syndrome: Critical Reviews and Clinical Advances. Informa Healthcare; 1st edition (October 30, 2000).
ANTICONVULSANTS
Gabapentin (Trade name:Neurontin), Gabitril, Lyrica (pregabalin)
Anticonvulsants are used to treat seizure disorders (epilepsy). More recently, they have been used to treat neuropathic pain, anxiety and insomnia. The most commonly prescribed anticonvulsants for CFS/ME are Neurontin (generic: gabapentin), Gabitril, and Lyrica (pregabalin).
FURTHER READING
Maija Haavisto's website: http://maija-haavisto.suite101.com/anticonvulsants-cfsme-and-fm-a65954
Good overview of the use of anticonvulsants for CFS/ME and FM.
GABAPENTIN (NEURONTIN)
DESCRIPTION: Gabapentin (trade name: Neurontin) is a GABA (gamma aminobutyric acid) analogue used to treat epilepsy.
BACKGROUND. GABA is the chief inhibitory neurotransmitter in the nervous system. Basically, nerves have only two responses to stimuli—either they fire, or they don't. The role of GABA in the nervous system is to prevent neurons from firing, essentially turning them off. As the nervous system depends on a balance of chemicals that promote firing (excitatory neurotransmitters) and those that don't (inhibitory neurotransmitters), GABA serves an essential regulatory function. Without GABA too many neurons would fire at once, resulting in seizures.
Neurontin was originally approved by the FDA for the treatment of epilepsy. However, since its approval, it has been marketed for many off-label uses, including pain, headaches, alcohol and cocaine withdrawal, hiccups, restless leg syndrome, hot flashes and fibromyalgia. In 2004, in one of the biggest lawsuits in pharmaceutical history, Pfizer, the manufacturer of Neurontin, was sued for fraud based on its marketing of the drug for many of these off-label purposes. A second lawsuit claimed that Pfizer engaged in "outright deception of the biomedical community, and suppression of scientific truth." However costly for Pfizer, lawsuits for off-label uses have not prevented doctors from continuing to prescribe Neurontin for insomnia, pain, anxiety disorders, and diabetes.
USES IN CFS/ME. Dr. Jay Goldstein (now retired) was one of the early proponents of Neurontin as a CFS/ME treatment. His theory was that the brain needed to be “reset” in CFS/ME patients, and to accomplish that goal, he used Neurontin. Dr. Seastrunk, a psychiatrist in Texas, believed that Neurontin helped minimize focal brain injury in CFS/ME and FMS patients. Dr. Cheney has also included Neurontin in his treatment protocol, believing that it exerts a protective effect on the brain.
In 2007, research supported by the National Institutes of Health's National Institute of Arthritis and Musculoskeletal and Skin Diseases showed that gabapentin can be an effective treatment for fibromyalgia. In a randomized, double-blind trial of 150 patients with FM, researchers found that patients taking daily doses of 1,200 to 2,400 mg of gabapentin experienced significantly less pain than those taking placebo.
PROTOCOL. Dr. Goldstein recommended a total daily dose of 5,000 mg (if lower doses were not beneficial). However, he first tested his patients with only 100-800 mg for possible reactions. Dr. Seastrunk recommended starting with small doses and increasing to 3,200 mg a day, taken throughout the day. Dr. Cheney's protocol started at 300 mg, taken three times a day. Dr. Teitelbaum recommends beginning with 100-300 mg at night, and slowly increasing up to 300-900 mg taken three times a day.
PROS AND CONS. CFS/ME patients report that gabapentin helps with pain and insomnia. However, because gabapentin reduces neuronal firing, it can also produce dizziness, tingling, “brain fog,” and a “drunk” feeling. One of the reported side effects is an increase in bladder pain among people with interstitial cystitis. When going off gabapentin, slowly decreasing the dose rather than stopping all at once is advised.
AVAILABILITY AND COST. Gabapentin (generic) is available at any pharmacy. It requires a prescription. A 100-tablet bottle (100 mg) costs from $24 to $32. Insurance usually covers.
FURTHER READING
Good description of the different function that GABA plays in the nervous system. http://www.denvernaturopathic.com/news/GABA.html
National CFS/ME foundation's report on Neurontin: http://www.ncf-net.org/forum/neurontin98.htm
“Neurontin and Brain Injury Treatment.” Dr. Seastrunk's views on Neurontin: http://www.ncf-net.org/forum/neurontin98.htm
“Researchers explore many uses for Neurontin; no CFS/ME trials planned.” CFIDS Chronicle, March-April 1999 http://www.cfids.org/archives/1999/1999-2-article04.asp
“Gabapentin Shown Effective for Fibromyalgia Pain.” http://members.boardhost.com/WellnessTrain/msg/1188292455.html
RESEARCH
Foldvary-Schaefer N, De Leon Sanchez I, Karafa M, Mascha E, Dinner D, Morris HH. “Gabapentin increases slow-wave sleep in normal adults.” Epilepsia. 2002 Dec;43(12):1493-7. http://www.ncbi.nlm.nih.gov/pubmed/12460250 (Abstract)
Kesselheim AS, Darby D, Studdert DM, Glynn R, Levin R and Avorn J. “False claims act prosecution did not deter off-label drug use in the case of neurontin.” Health Aff (Millwood). 2011 Dec;30(12):2318-27. http://www.ncbi.nlm.nih.gov/pubmed/22147859 (Abstract)
PATIENT REVIEWS
A woman with interstitial cystitis recounts her experience with Neurontin: http://www.ic-network.com/iclifestyles/may03.html
CFS/ME patient reviews of Neurontin: http://www.revolutionhealth.com/drugs-treatments/rating/neurontin-for-chronic-fatigue-syndrome-cfs-cfids-me
GABITRIL
DESCRIPTION. Gabitril (generic: tiagabine) is a selective GABA reuptake inhibitor used to treat seizure disorders.
BACKGROUND. Gabitril was first developed in 1988 by the Danish pharmaceutical company, Novo Nordisk. Currently, it is approved by the FDA for the treatment of partial seizures, although doctors prescribe it for treating panic disorder and neuropathic pain (including fibromyalgia). Gabitril is also used in combination with antidepressants and benzodiazepines for treating anxiety.
PROTOCOL. Dr. Goldstein considers Gabitril to be safe and effective at low doses. He cautions that if the dose is increased too rapidly, patients may become delirious or manic.
PROS AND CONS. Some patients report that Gabitril is a “wonder drug” for treating insomnia. Patients also report a reduction in pain and fatigue. Other patients report either no effect at all, or excessive sedation. The most frequently reported side effects of Gabitril are sedation, increase in “brain fog,” and gastric upset, and, in doses over 8 mg, tingling (paresthesia) in the hands. Gabitril can induce seizures in those without previous seizure disorder, particularly in people taking other GABA enhancers.
AVAILABILITY AND COST. Gabitril is available with a prescription at pharmacies. It is quite expensive. A 30-tablet bottle (2 mg) costs roughly $170. Insurance usually covers the cost.
PATIENT REVIEWS
CFS/ME patient reviews of Gabitril: http://www.revolutionhealth.com/drugs-treatments/rating/gabitril-for-chronic-fatigue-syndrome-cfs-cfids-me
LYRICA
DESCRIPTION. Lyrica (pregabalin, pronounced “pruh-GA-buh-lin”) is an anticonvulsant used to treat neuropathic pain and partial seizures.
BACKGROUND. Lyrica was designed by Richard Silverman, a medicinal chemist at Northwestern University, as a stronger version of gabapentin. Aside from its anti-seizure effects, it is used for post-herpetic neuralgia (shingles), and diabetic peripheral neuropathy. Pfizer has also claimed that Lyrica is useful for treating anxiety. Although Pfizer was later sued for making that claim, Lyrica has been approved in Europe for treating generalized anxiety disorder. In 2010, sales reached $3,063 million. Lyrica was the first medication approved by the FDA for the treatment of fibromyalgia.
USES IN CFS/ME. Lyrica is used mainly as a sleep aid and for pain. While most doctors feel that it is no more effective than gabapentin, the decreased risk of habituation makes it an attractive alternative.
In a study published in the journal Pediatrics in 2009, Drs. Felicia B. Axelrod and Dena Berlin successfully treated a small group of children suffering from daily dysautonomic crises with Lyrica. Dysautonomic crises are severe upsets to the sympathetic nervous system, which are characterized primarily by profound nausea and retching, as well as flushing, tachycardia, and excessive production of gastric and pulmonary mucus. After measuring the effects of Lyrica, Axelrod and Berlin found that 53% of the patients experienced a greater than 50% reduction in crises.
While this was a small study, it is highly significant for the CFS/ME community. Dysautonomia is found in 96% of the CFS/ME population, and while not all experience dysautonomic crises, those who do may find relief with Lyrica.
PROTOCOL. Physicians start patients with a low dose of Lyrica and increase it gradually. Therapeutic effects appear after one week. Dr. Teitelbaum recommends 50-250 mg a night as a sleep aid.
PROS AND CONS. In many respects, Lyrica is similar to benzodiazepines (minor tranquilizers). But, unlike benzodiazepines, effects do not decrease over time. Lyrica does not disrupt sleep cycles, and produces less cognitive impairment than benzodiazepines. It also has a low potential for dependence. Patient reviews of Lyrica are mixed. Some patients have found that it helps enormously with fatigue, while other report it increases fatigue. Most patients report that it helps them more with pain than any other symptom. Side effects include jitters, dizziness, and nausea.
AVAILABILITY AND COST. Lyrica is available at any pharmacy with a prescription. It costs roughly $3 a pill. Insurance usually covers the cost.
FURTHER READING
Axelrod, Felicia B., and Dena Berlin. “Pregabalin: A New Approach to Treatment of the Dysautonomic Crisis.” Pediatrics 2009;124;74. http://pediatrics.aappublications.org/content/124/2/743.full.pdf
PATIENT REVIEWS
CFS/ME patient reviews of Lyrica: http://www.revolutionhealth.com/drugs-treatments/rating/lyrica-for-chronic-fatigue-syndrome-cfs-cfids-me
ANTIDEPRESSANT DRUGS
CAUTION: The FDA has instituted a “black box” label warning for antidepressants, indicating that antidepressants may increase the risk of suicidal thinking and behavior in some children and adolescents. A black-box warning is the most serious type of warning in prescription drug labeling.
DESCRIPTION. Antidepressant drugs are a class of pharmaceutical products that influence neurochemicals in the brain.
BACKGROUND. The National Institute of Mental Health estimates that one in five adults can expect to experience at least one episode of mood disorder in the course of a lifetime. Although antidepressants were developed to treat mood disorders such as anxiety and depression, clinicians have found that the symptoms of many chronic illnesses seem to respond to antidepressant therapy. Antidepressants have been used to treat chronic pain syndromes, migraine headaches, irritable bowel syndrome, bladder and urinary problems, and bulimia. Antidepressants are currently the third most prescribed drug in the U.S. According to the CDC, one in ten Americans over the age of twelve is currently taking an antidepressant.
The first antidepressants, monoamine oxidase inhibitors (MAOIs), were discovered by accident in the 1950s, when doctors in a Swiss tuberculosis clinic noticed euphoria in patients treated with an MAOI called iproniazid. By the late 1950s, MAOIs were developed to treat depression and severe panic disorder. This class of drug operates by inhibiting the action of monoamine oxidase, the enzyme that breaks down epinephrine (adrenaline), norepinephrine (noradrenaline), serotonin, and other monoamines.
In the late 1960s, a more targeted drug, the tricyclic antidepressant, was introduced. The tricyclics (TCAs) were originally developed from antihistamines, and like MAOIs induced heightened mood in patients. Tricyclics operate by increasing the amounts of serotonin and/or norepinephrine in the brain. However, the tricyclics produced several side effects, so in the late 1980s, a new neurochemical modulator, Prozac (fluoxetine), was approved by the Food and Drug Administration (FDA). Prozac is one of the family of drugs known as selective serotonin reuptake inhibitors (SSRIs). These act directly on a brain cell's ability to reabsorb serotonin, a neurotransmitter involved in many neurological functions, including sleep, digestion, blood flow, and, of major importance, mood elevation.
Unfortunately, the SSRIs produced sexual dysfunction, so in 1994 yet another class of antidepressants, serotonin-norepinephrine reuptake inhibitors (SNRIs), was developed by Wyeth. It was thought that by acting on two neurotransmitters the SNRIs would avoid the major side effects of the SSRIs, as well as helping with chronic pain.
USES IN CFS/ME. Antidepressants are perhaps the most widely prescribed pharmaceuticals for CFS/ME. Patients often are dismayed and concerned when their physicians suggest an antidepressant. It appears they are being diagnosed with depression, which, although sometimes a symptom of CFS/ME, is clearly not the underlying cause. Nonetheless, low-dose antidepressants have a place in the treatment of a number of CFS/ME symptoms.
Most CFS/ME patients have low amounts of serotonin and dopamine, two neurochemicals which have profound effects on sleep, cognitive function, and digestion. As a consequence, antidepressants have proven helpful in improving sleep, energy levels, and cognitive function. In addition, SSRIs, SNRIs and tricyclics have been shown to have anti-inflammatory and immunomodulatory effects. A secondary, though significant, effect of antidepressants is to increase blood volume by reducing urinary output. Pain and fatigue often increase urinary volume, which in turn can lead to reduced blood pressure and blood volume, along with a loss of metabolites. Antidepressants can improve kidney function, leading to improved metabolism and a reduction of overall fatigue.
Although there are various antidepressants to choose from, not all patients with CFS/ME respond well to these medications. Often CFS/ME patients with sensitivities to medications cannot tolerate any antidepressant, even in the smallest doses. In a survey of patients with chemical sensitivities conducted by a DePaul University research team, more than 50% of respondents reported negative effects of antidepressants.
Dr. Fred Friedberg, author of Coping With Chronic Fatigue Syndrome: Nine Things You Can Do, also found that a substantial proportion (about one-third) of 249 patients with CFS/ME reacted negatively to antidepressants. This finding is borne out by a treatment survey conducted in 2010 by the ME Association in which 30%-38% of respondents reported that antidepressants, of all classes, made them feel worse.
It is crucial for physicians and patients to remember that CFS/ME patients usually require much lower doses of these medications than other patients, and therefore the dose prescribed should be one tenth or less (depending on the sensitivity of the patient) of the standard dose. In his book, The Doctor's Guide to Chronic Fatigue Syndrome, Dr. David Bell, pediatric CFS/ME specialist, states that giving patients with CFS/ME a standard dose of antidepressants can virtually serve as a diagnostic test for the illness – most patients are immobilized by it.
That being said, antidepressants do provide some degree of symptomatic relief for many patients. It is important, however, to be attentive to side effects, which frequently mimic the symptoms of the illness itself. Excessive fatigue and drowsiness, headaches, nausea, diminished libido, insomnia, and agitation can either be due to the effects of the drug or to the CFS, so it is important to be observant and monitor the dosage carefully.
FURTHER READING
“Using Antidepressants to Treat Chronic Fatigue Syndrome.” Dr. Charles Lapp. CFIDS Chronicle, Summer 2001. http://www.cfids.org/archives/2001rr/2001-rr3-article01.asp
Dr. Lapp's treatment protocols for antidepressants. Contains a useful chart. http://www.cfids.org/archives/2001rr/2001-rr3-article01.asp?view=printhttp://www.prohealth.com/library/showarticle.cfm?libid=8801
Interesting thread on antidepressants used for gut problems. http://phoenixrising.me/forums/showthread.php?6321-Thoughts-on-the-methylation-treatment-for-CFS/page5
Lists antidepressants, side effects, brand names by country, “things your doctor won't tell you.” http://www.crazymeds.us/pmwiki/pmwiki.php/Main/HomePage
BOOK
Dr. Cheney recommends patients and physicians read the book Prozac Backlash: Overcoming the Dangers of Prozac, Zoloft, Paxil and Other Antidepressants by Joseph Glenmullen, M.D., a psychiatrist at the Harvard Medical School
TRICYCLIC ANTIDEPRESSANTS
CAUTION: Tricyclic antidepressants increase the amount of norepinephrine in the brain. They cannot be given in conjunction with MAOIs because of the risk of producing dangerously high blood pressure. The National Institutes of Health (NIH) does not recommend tricyclics for children or teens.
DOXEPIN
Brand: Sinequan, Silenor, Adapin
USES IN CFS/ME. Doxepin, one of the most commonly used medications in the treatment of CFS/ME, is of major benefit in treating sleep disturbance. In a study conducted by Weber et al, 3 – 6 mg of doxepin administered before bed improved total sleep time without causing next-day sedation. Krystal et al found that as little as 1 – 3 mg of doxepin increased slow wave sleep (stage 3 and 4) in elderly patients. It is believed that doxepin may help correct the slow-wave sleep deficit found in both CFS/ME and fibromyalgia. Improvement in sleep often brings an increase in energy levels and reduction in the pain associated with CFS/ME and fibromyalgia. Many patients with CFS/ME also report improvement in allergies as a result of doxepin's potent histamine-blocking properties. In this regard, Dr. Cheney believes that doxepin at low doses may function as an immune modulator. By softening immune system activation, doxepin can relieve sore throats, swollen glands and congestion.
PROTOCOL. Low doses (2 to 10 mg) of doxepin, taken 1 to 2 hours before bedtime, are usually prescribed to treat CFS/ME symptoms. Liquid formulations allow for even smaller doses. Because CFS/ME patients can be very sensitive to doxepin, Dr. Cheney recommends starting at two drops of liquid doxepin (10mg/cc) on the tongue, increasing up to 10 drops (5mg or ½ cc). Liquid doxepin can mixed into four ounces of water or juice.
PROS. Most patients report improved quality of sleep, better endurance, and energy. While some patients experience daytime sedation during the first few days, this problem usually resolves rapidly. Benefits are often noted fairly quickly, within a few days.
CONS. Side effects include weight gain, constipation, and dry mouth. Too high a dose can result in nightmares. Many patients with CFS/ME report excessive sedation or a drugged feeling and therefore cannot tolerate treatment. Paradoxically, some feel depressed after taking the drug (but not before).
AVAILABILITY AND COST. Liquid doxepin costs about $17 for a 120 cc bottle. (If you are taking two drops on the tongue, 120 ccs will last a very long time). Both pill and liquid forms are available by prescription in generic and brand-name formulations. Insurance usually covers.
FURTHER READING
Good review of sleep studies with low-dose doxepin http://brainposts.blogspot.com/2011/01/low-dose-doxepin-for-insomnia-treatment.html
AMITRIPTYLINE
Brand: Elavil, Vanatrip, Endep (Australia; Canada; New Zealand; South Africa); Domical (United Kingdom)
USES IN CFS/ME. Amitriptyline is beneficial for treating pain, sleep disturbance, headaches, and gastrointestinal problems and may be recommended if doxepin produces excessive sedation. In addition, amitriptyline is often helpful in treating interstitial cystitis, a disorder that affects many women with CFS/ME. Interstitial cystitis symptoms that may respond to amitriptyline are frequent urination, and bladder and pelvic pain. Dr. Alan Wein, a urologist who specializes in treating interstitial cystitis, has noted that amitriptyline is effective for nearly 50% of his patients, probably because of its antihistamine properties.
PROTOCOL. Dosage varies, but generally 10 mg or less nightly is prescribed. Dr. Myhill starts at 5 mg to minimize side effects. Some patients report better results with amitriptyline by “pulsing” the medication (taking it every third or fourth night).
PROS. Benefits are noted quickly. The most frequent benefits reported by people with CFS/ME are improved sleep and reduced pain.
CONS. The side effects of amitriptyline are similar to those of doxepin, although exacerbation of muscle weakness in CFS/ME seems to be more common with amitriptyline than with other antidepressants. Some patients have had to discontinue the drug because of weight gain, dry mouth, and palpitations. Dr. Lapp notes that while amitriptyline may help patients improve sleep, it can reduce deep sleep, which impairs its effectiveness over the long term. There is some evidence that amitriptyline may cause CoQ10 deficiency, resulting in oxidative stress and altering the function of mitochondria. In a 2011 study, Bautista-Ferrufino et al recommend supplementation with CoQ10 during treatment with amitriptyline.
AVAILABILITY AND COST. Amitriptyline is available by prescription and is inexpensive. The generic drug costs about $10 for a 30-day supply. Insurance usually covers.
FURTHER READING
Good summary of the uses of Elavil for CFS/ME: http://phoenixrising.me/?page_id=4710
PATIENT REVIEWS
CFS/ME patients' reviews of Elavil: http://www.everydayhealth.com/drugs/elavil-for-chronic-fatigue-syndrome-cfs-cfids-me/review?page=2
RESEARCH
Bautista-Ferrufino, María Rosa, Mario D. Cordero, José Antonio Sánchez-Alcázar, Matilde Illanes, Ana Fernández-Rodríguez, Plácido Navas, Manuel de Miguel. “Amitriptyline induces coenzyme Q deficiency and oxidative damage in mouse lung and liver.” Toxicology Letters. Volume 204, Issue 1, 4 July 2011, Pages 32-37. http://www.sciencedirect.com/science/article/pii/S0378427411001342 (Abstract)
NORTRIPTYLINE, DESIPRIMINE, IMIPRAMINE, CLOMIPRAMINE, TRIMIPRAMINE
Generic: Nortriptyline Brand: Pamelor, Sensoval, Aventyl , Allegron, Noritren, Nortrilen
Generic: Desipramine Brand: Norpramin, Pertofrane
Generic: Imipramine Brand: Tofranil
Generic: Trimipramine Brand: Sermontil
Generic: Clomipramine Brand: Anafranil
USES IN CFS/ME. Nortriptyline, desipramine and imipramine are second-generation tricyclic antidepressants which primarily block the reuptake of norepinephrine, and, to a lesser degree, serotonin. All three are used in patients with CFS/ME, though not as frequently as first-generation tricyclics. They are helpful in treating fatigue, pain, sleep disturbance, and anxiety. Their main side effects are similar to those of other tricyclic antidepressants: dry mouth, constipation, and weight gain (due to increased appetite). Although the second-generation tricyclics are often prescribed for sleep, they often interfere with sleep onset. Other side effects experienced by people with CFS/ME include shakiness, agitation and nausea.
Clomipramine and trimipramine, both of which were first developed in the 1960s, are in wider use in Europe than in the U.S. Like the other tricyclics, their mode of action is to block the uptake of serotonin and norepinephrine.
AVAILABILITY AND COST. Prices for second-generation tricyclics vary. Nortriptyline (generic) can be purchased for as low as $10 for a 30-day supply. Desipramine is slightly more expensive, ranging from $15 - $30 for a 30-day supply, while imipramine can be purchased for less than $10 for a 30-day supply. Insurance usually covers.
PATIENT REVIEWS
CFS/ME patient reviews of Pamelor: http://www.revolutionhealth.com/drugs-treatments/rating/pamelor-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of trimipramine: http://www.revolutionhealth.com/drugs-treatments/rating/surmontil-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of clomipramine: http://www.revolutionhealth.com/drugs-treatments/rating/anafranil-for-chronic-fatigue-syndrome-cfs-cfids-me
FURTHER READING
General information on trimipramine: http://en.wikipedia.org/wiki/Trimipramine
SELECTIVE SEROTONIN REUPTAKE INHIBITORS
CAUTION: SSRIs must not be taken within 14 days of discontinuing MAOIs. The NIH recommends against giving SSRIs to children or teens.
FLUOXETINE
Brand: Prozac, Sarafem, Rapiflux, Selfemra, Lovan (Australia), Oxactin (United Kingdom), Fluctin (Germany).
BACKGROUND. Fluoxetine (Prozac), the first SSRI to be approved in the late 1980s, differs from earlier antidepressants in that its mode of action is more specific. It works directly on altering the level and action of serotonin only (the tricyclic antidepressants inhibit uptake of norepinephrine as well). The SSRIs are often prescribed in place of tricyclic antidepressants because they have fewer side effects. Unlike other antidepressants, SSRIs do not cause sedation. In fact, fluoxetine can often act as a stimulant to increase energy. Nor does it cause the dry mouth, palpitations, and dry cough that are common with tricyclic drugs.
USES IN CFS/ME. Dr. Nancy Klimas, CFS/ME specialist and immunologist at the University of Miami, has studied the effect of SSRIs on the immune system. At the 1990 CFIDS conference in Charlotte, North Carolina, Dr. Klimas reported that more than half of 25 CFS patients given fluoxetine for three months showed moderate to marked improvement. Improvements in the number of natural killer cells seem to indicate that fluoxetine (and other serotonin-influencing drugs) may have a modulating effect on the immune system. However, in spite of these encouraging reports, no subsequent study has shown that fluoxetine has a greater effect than placebo on CFS/ME patients.
PROTOCOL. When used in CFS/ME, fluoxetine is generally given in considerably smaller dosage (2 to 10 mg, taken in the morning) than the standard dose used to treat depression.
PROS. Fluoxetine is effective in treating the fatigue of CFS/ME, the hallmark symptom of the syndrome. Other symptoms that may respond to treatment are pain, cognitive dysfunction, and sometimes excessive sleep. The drug is also helpful in treating the physiological depression that may accompany CFS/ME as a result of metabolic changes, as well as the secondary depression that stems from the devastating experience of having a chronic, debilitating illness. An additional benefit is that, unlike the tricyclic antidepressants, fluoxetine does not cause weight gain.
Fluoxetine has been shown to have a significant effect on patients with FM. In 2002, Arnold et al conducted a randomized, double-blind study, which showed improvement in pain, fatigue and depression in fibromyalgia patients. A similar study conducted in 1996 by Goldenberg et al found that the combination of fluoxetine and amitriptyline produced improvements in pain, sleep, and global well-being. (In Handbook of Primary Care Psychology, by Leonard J. Haas)
CONS. A number of people with CFS/ME are unable to tolerate the side effects of fluoxetine and have stressed emphatically that they will never try it again. Reports of anxiety, agitation, and even excessive sedation (a paradoxical reaction not unusual in CFS/ME patients) are common. In some cases the side effects of fluoxetine are profound, producing dissociation, flatness of affect and loss of a sense of self.
Because fluoxetine acts as a stimulant, people who have difficulty sleeping almost universally report worsening of insomnia. In addition, many clinicians advise their patients who have been taking MAOIs to allow a longer than usual interval (up to 5 weeks) before taking fluoxetine. This drug's long half-life may also require a longer interval after discontinuation before starting new antidepressant treatments. A double-blind study conducted by Dr. J.H. Vercoulen of the University Hospital of Nijmegen in The Netherlands concluded that fluoxetine (20 mg/day) had no beneficial effect on fatigue or any other symptoms of CFS (Lancet, 1996). Dr. Cheney has strongly advised against long-term use of fluoxetine, citing possible permanent disruption of serotonergic pathways.
AVAILABILITY AND COST. Fluoxetine is available in liquid to allow smaller doses. The cost can be as low as $4 a month for generic. Insurance usually covers the cost. Not recommended for patients with diabetes.
PATIENT REVIEWS
CFS/ME patient reviews of Prozac: http://www.revolutionhealth.com/drugs-treatments/rating/prozac-for-chronic-fatigue-syndrome-cfs-cfids-me
REFERENCES
Haas, Leonard J, ed. Handbook of Primary Care Psychology. Oxford University Press, USA, 2004.
Vercoulen J et al. “Randomized, double-blind, placebo-controlled study of fluoxetine in chronic fatigue syndrome.” Lancet. 1996; 347: 858-61 and 1770-2.
SERTRALINE, PAROXETINE
Generic: Sertraline Brand: Zoloft, Lustral (Britain, Ireland, Israel)
Generic: Paroxetine Brand: Paxil, Pexeva, Seroxat (Britain), Aropax (Australia, New Zealand)
USES IN CFS/ME. Sertraline (Zoloft) and paroxetine (Paxil) are two newer drugs that are similar to fluoxetine, but because they are associated with fewer side effects may be more easily tolerated. Both drugs have a shorter half-life than fluoxetine does. Both have been used to treat CFS/ME for treating symptoms such as fatigue, cognitive dysfunction, mood swings, pain, sleep disorders, and immune dysfunction.
PROS AND CONS. As with other SSRIs, patient experiences vary widely. Some patients report an increase in energy and relief from pain, while others report nausea, loss of appetite, a “floating feeling,” and hormonal complications. Withdrawal symptoms of paroxetine may be intense, producing flu-like symptoms, nausea, irritability, anxiety, and crying jags. A few patients have mentioned that they felt as bad while taking these drugs as they did with other antidepressants, reminding us that many patients cannot tolerate any form of antidepressant. For these patients, alternative treatments have been suggested, including vitamins, amino acids, herbs, and other complementary therapies.
PATIENT REVIEWS
CFS/ME patient reviews of Zoloft: http://www.revolutionhealth.com/drugs-treatments/rating/zoloft-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Paxil: http://www.revolutionhealth.com/drugs-treatments/rating/paxil-for-chronic-fatigue-syndrome-cfs-cfids-me
CITALOPRAM
Brand: Celexa; Cipromil (Britain, Australia)
USES IN CFS/ME. Celexa is sometimes prescribed for POTS (postural orthostatic tachycardia syndrome), so those patients with syncope (fainting), NMH (neurally mediated hypotension), and related disorders may benefit from Celexa. It is not as frequently prescribed for CFS/ME as other antidepressants, due to numerous side effects.
PROS AND CONS. Some patients report a lessening of symptoms, particularly those associated with PMS. Others report severe migraines, nose bleeds, insomnia, nightmares, and confusion. Sexual dysfunction is a common side effect. Patients should start at a very low dose.
PATIENT REVIEWS
CFS/ME patient reviews of Celexa: http://www.revolutionhealth.com/drugs-treatments/rating/celexa-for-chronic-fatigue-syndrome-cfs-cfids-me
EXCITALOPRAM
Brand: Lexapro, Cipralex, Seroplex, Lexamil, Lexam, Entact
Excitalopram is an SSRI noted for its high selectivity of serotonin. It is reputed to be a more potent antidepressant than its “parent,” citalopram. Excitalopram has had a history of controversy since its introduction in the 1990s, and has generated a number of lawsuits. Nonetheless, excitalopram is one of the SSRIs that has been used for CFS/ME, though not as widely as other antidepressants.
PATIENT REVIEWS
CFS/ME patient reviews of Lexapro: http://www.google.com/search?rlz=1C1GGGE_enUS379US379&aq=f&gcx=w&sourceid=chrome&ie=UTF-8&q=lexapro
MONOAMINE OXIDASE INHIBITORS (MAOIs)
CAUTION: Foods and medications containing a high amount of tyrosine (fermented foods, wine, cheese, pickles, decongestants) can interact with MAOIs, producing sharply elevated blood pressure and increasing the risk of stroke.
PHENALZINE, TRANYLCYPROMINE
Generic: Phenalzine Brand: Nardil, Nardelzine
Generic: Tranylcypromine Brand: Parnate, Jatrosom
USES IN CFS/ME. MAOIs are used much less frequently than other antidepressants to treat CFS/ME. The side effects associated with phenalzine (Nardil ) and tranylcypromine (Parnate) can be severe. An additional drawback is the dietary restrictions that accompany MAOI use. Foods that contain the amino acid tyramine (aged cheese, yogurt, wine, avocado, among many others) must be avoided to prevent severe hypertensive crisis. Because these foods are so common, patients may find compliance difficult. While some patients with CFS/ME have found MAOIs effective, others have reported agitation and insomnia. One patient believed an MAOI may have contributed to a prolonged relapse, producing even greater neurological and cognitive problems than she had experienced previously.
AVAILABILITY. MAOIs are available from any pharmacy with a doctor's prescription. Most major insurance carriers do not cover MAOIs for the treatment of CFS/ME.
OTHER ANTIDEPRESSANTS
BUPROPION
Brand: Wellbutrin, Aplenzin, Budeprion, Buproban, Zyban
CAUTION: Bupropion should not be taken by patients with a history of seizures.
USES IN CFS/ME. Bupropion is an atypical antidepressant frequently used to treat the fatigue associated with CFS/ME. Bupropion is the first antidepressant to increase dopamine, a neurotransmitter often found to be low in CFS/ME patients. Bupropion is believed to be both a norepinephrine and dopamine reuptake inhibitor.
PROS. Physicians who specialize in the treatment of CFS/ME have prescribed bupropion when SSRIs have failed, and find it of benefit in improving energy and controlling mood. In some patients, bupropion does not produce the unpleasant side effects noted with other antidepressants. The drug may be taken alone or with other tricyclic antidepressants to improve sleep. Patients have reported increased energy, alleviation of depression, increase in concentration, and better sleep.
CONS. Bupropion is short acting, much like stimulants (e.g., Ritalin). Because bupropion raises dopamine, it is more habit-forming than other antidepressants. Side effects can be similar to those of SSRIs (jitters, anxiety, insomnia). Many patients find that bupropion, like CNS stimulants, provides only a short burst of energy, followed by a crash. Even patients who feel that bupropion has provided significant relief for cognitive symptoms have reported “cyclic thoughts” (like having a song stuck in your head). Patients have also reported headaches, nightmares, shakiness, rapid heartbeat, weight gain, and stomach irritation. The biggest drawback to the use of bupropion is the risk of seizures. Bupropion is not recommended for patients who are sensitive to stimulants, or who have a history of seizures or heart problems.
PROTOCOL. The standard initial prescribed dose is 75 mg daily. CFS/ME patients may wish to start with a third of the standard dose to check for tolerance.
AVAILABILITY AND COST. Bupropion is available at any pharmacy with a prescription. A one-month supply costs from $10-$24. It can be ordered online with a prescription. Insurance usually covers.
PATIENT REVIEWS
CFS/ME patient reviews of Wellbutrin: http://www.revolutionhealth.com/drugs-treatments/rating/wellbutrin-for-chronic-fatigue-syndrome-cfs-cfids-me
TRAZODONE
Brand: Desyrel, Oleptro, Trialodine (Deprax in Spain, Molipaxin in Britain, Thombran in Europe, Trazorel in Canada )
USES IN CFS/ME. Among the most sedating antidepressants, Desyrel is often used to treat insomnia. Desyrel stimulates deep sleep (stage 3 and stage 4) and is particularly helpful for those who wake up too early. It is not, however, as helpful as many of the other antidepressants in treating anxiety and depression in CFS/ME. Some patients report improved sleep with a low dose of Desyrel, but experience severe orthostatic hypotension with higher doses. Desyrel has fewer anticholinergic side effects than tricyclics, but patients still report dry eyes and mouth, and constipation. The most commonly reported side effects include nausea, excessive sedation, nightmares, dizziness, and unrefreshing sleep. Morning grogginess (“hangover”) is common.
PROTOCOL. The prescribed dose in CFS/ME is generally 25 to 50 mg at bedtime. Dr. Bell recommends 25 mg taken ½ hour to two hours before bed.
AVAILABILITY AND COST. A 30-day supply of the generic drug (25mg) costs about $7.
VENLAFAXINE
Brand: Effexor
USES IN CFS/ME. When it was approved for commercial use, Effexor (venlafaxine) received a remarkable amount of publicity and was touted as a newer and better Prozac. Effexor is chemically unrelated to the other antidepressants and has a unique mode of action, blocking serotonin, norepinephrine, and dopamine reuptake. However, effects of the drug in CFS/ME have been less than dramatic. Many patients report that Effexor worsens anxiety, and, paradoxically, depression. Withdrawal symptoms can be severe, including dizziness, nausea and headaches. Dr. Jay Goldstein commented that, while Effexor may have been marketed as "the best thing since sliced bread," his experience taught him to view it simply as another alternative treatment, rather than the most effective antidepressant (CFIDS Chronicle, Physicians Forum, Fall 1993). Dr. Goldstein reported nausea and hypertension as possible side effects.
AVAILABILITY AND COST. The generic is available at pharmacies and online regardless of dosage at roughly $10 for a 30-day supply (prices vary).
PATIENT REVIEWS
CFS/ME patient reviews of Effexor: http://www.revolutionhealth.com/drugs-treatments/rating/effexor-for-chronic-fatigue-syndrome-cfs-cfids-me
DULOXETINE
Brand: Cymbalta; Yentreve and Ariclaim (Europe)
USES IN CFS/ME. Cymbalta, one of three medications currently approved for the treatment of fibromyalgia. is a serotonin-norepinephrine reuptake inhibitor (SNRI) primarily prescribed for pain. Although Cymbalta is often prescribed by rheumatologists for their patients with fibromyalgia, most CFS/ME doctors prefer tricyclics or SSRIs over Cymbalta.
PROS and CONS. Many CFS/ME patients report that Cymbalta makes them restless and anxious. But patients who have had success with other stimulants may find that Cymbalta improves energy and mood. Because of its short half-life, discontinuation symptoms can be quite severe, including depression, irritability, agitation, sensory disturbances, dizziness, headache, insomnia, and seizures.
PROTOCOL. Doctors recommend beginning at a low dose (20 mg) and then gradually increasing as needed. Cymbalta can be pulsed (taken every second or third day).
AVAILABILITY AND COST. Cymbalta is available at any pharmacy with a prescription. A month's supply of the generic at 20 mg costs roughly $28.
PATIENT REVIEWS
CFS/ME patient reviews of Cymbalta: http://www.revolutionhealth.com/drugs-treatments/rating/cymbalta-for-chronic-fatigue-syndrome-cfs-cfids-me
MIRTAZAPINE
Brand: Remeron; Avanza, Axit (Australia); Zispin SolTab (Britain and Ireland); Norset (France); Remergil (Germany)
BACKGROUND. Remeron is a tetracyclic antidepressant, one of the few drugs that falls into the class of noradrenergic and specific serotonergic antagonists (NaSSAs). The NaSSAs act by inhibiting adrenergic and serotonin receptors. Remeron is dispensed orally in a tablet that dissolves on the tongue.
PROS AND CONS. The most common side effect of Remeron is weight gain, but as with tricyclics, CFS/ME patients may also experience blurred vision, dry mouth, constipation, dizziness and sedation. Many patients report sugar cravings. On the positive side, some patients report that Remeron has helped improve sleep. Dr. Lapp prescribes Remeron when there has been significant weight loss coupled with insomnia.
AVAILABILITY AND COST. Remeron is available at most pharmacies. A month's supply of 15 mg of the brand version costs roughly $25.
PATIENT REVIEWS
CFS/ME patient reviews of Remeron: http://www.revolutionhealth.com/drugs-treatments/rating/remeron-for-chronic-fatigue-syndrome-cfs-cfids-me
ANTIFUNGAL AGENTS
Nystatin, Diflucan, Nizoral, Sporanox
DESCRIPTION. Antifungal drugs are used to treat Candida albicans and other fungal infections.
NYSTATIN
BACKGROUND. In the 1940s, two scientists found a bacterium in soil that inhibited the growth of molds. They discovered that the bacterium binds to ergosterol, a major component of the cell membrane of the fungus. When the bacterium was sufficient concentrations, it formed pores in the membrane that produced leakage and eventually led to the death of the fungus. They named the substance “nystatin,” after New York State, where it was discovered. The drug was patented in the 1950s, and for the next twenty years nystatin was primarily used in suppositories to treat vaginitis. It was popularized in the early 1980s, when studies by several clinicians chronicled the successful treatment of chronic candidiasis (yeast infection) with nystatin.
USES IN CFS/ME. Because candidiasis is a condition that produces extreme fatigue, depression, muscle pain, concentration problems, along with other symptoms which are common in CFS/ME, many CFS/ME patients turned to antifungal regimens in the 1980s. Although some physicians consider candidiasis controversial and without scientific basis, many CFS/ME clinicians use nystatin and other antifungal agents to treat Candida overgrowth. Dr. Murray Susser and Dr. Michael Rosenbaum, among other physicians, used antifungal medications when symptoms of Candida infection were present, especially when accompanied by a medical history of antibiotic or steroid use that may have contributed to Candida overgrowth. As an additional aid to determining whether an antifungal regimen might be helpful, a number of physicians use stool tests to measure Candida.
PROTOCOL. Many CFS/ME physicians suggest using the powdered form of nystatin, citing that it works better than the pill form and is more pure (free of dyes
or additives). The target dose is ¼ teaspoon, four times a day. A much lower dose (1/16 tsp once a day) should be used initially to prevent die-off reactions.
Dr. Teitelbaum recommends a target dose of two tablets three times a day (500,000 units), starting with one tablet a day and increasing by one tablet a day until you are up to the target dose for five to eight months. He recommends that if nausea occurs the dose be reduced to two tablets a day, or replaced by nystatin powder mixed in water. In Chronic Fatigue Syndrome and the Yeast Connection, Dr. William Crook notes that flushing, fever, and agitation may indicate that the dose is too high. Indications that the dose is too small include excessive fatigue, cold, and achiness.
PROS. Nystatin is considered safe when taken in oral or topical form. As nystatin is not absorbed through the gut, side effects from the drug are minimal. A surprisingly large number of patients report that nystatin (in combination with dietary changes and nutritional supplements as part of Candida control) has helped improve symptoms of CFS/ME. Patients often report increased energy, improved immune function, and better overall health after taking nystatin. Some symptoms (e.g., thrush, gastrointestinal complaints) respond quickly to treatment, but it can take weeks or months before overall improvement is observed.
CONS. While a number of patients note steady improvement over time, others experience no benefit after long trials of nystatin, and still others are not able to tolerate the drug at all. It is important to note that with all antifungal medications the phenomenon of "die-off" may be the actual cause of side effects; that is, as the antifungal medication kills the yeast cells, the dead cells secrete toxins into the body and symptoms may worsen initially. Symptoms of die-off include increased fatigue, muscle aches, and headaches, as well as diarrhea, nausea, upset stomach and vomiting. It can be difficult to differentiate between symptoms that could be due to die-off, intolerance for the drug, or perhaps simply a "bad day."
AVAILABILITY AND COST. Nystatin is available over the counter in suppository form to treat vaginitis and is widely available in creams for topical use. It is available in pill, tablet, liquid, lozenge, and powder form by prescription at most pharmacies. The powder comes in 15-, 30-, and 60-gram bottles. Hi-Tech Pharmacal Co, Inc. Amityville, NY 11701 and Paddock Laboratories, Inc. Minneapolis, MN 55427 are the two companies that currently produce nystatin powder. The powder is quite expensive at over $100 for a 30-gram bottle. Nystatin, in all forms, is usually covered by insurance.
DIFLUCAN
BACKGROUND. Diflucan (fluconazole), an antifungal introduced in the United States in 1990, is extremely valuable in treating the life-threatening Candida infections that sometimes occur in immunocompromised patients, such as those with AIDS or advanced cancer.
Diflucan differs from nystatin in that it is absorbed through the intestinal wall and traverses the bloodstream, thereby penetrating anywhere excessive yeast
colonization is found. Therefore, in theory at least, Diflucan may be more beneficial than nystatin to treat pervasive yeast infections.
USES IN CFS/ME. Many clinicians have found Diflucan beneficial for treating CFS/ME symptoms. A respected CFS/ME specialist, Dr. Carol Jessop, has used antifungal therapies when patients have symptoms suggestive of Candida overgrowth. She has stated that although other agents may be of benefit, Diflucan was her treatment of choice. Dr. Jessop found that because Diflucan penetrates the central nervous system, her patients experienced improvement in cognitive problems. This was not the case with nystatin or Nizoral. On the other hand, Dr. Jay Goldstein, who used Diflucan chiefly to treat gastric disturbances, reported only limited success (CFIDS Chronicle, Physician's Forum, Spring 1991).
PROTOCOL. Dr. Teitelbaum prescribes 200 mg for 6-12 weeks. If die-off symptoms appear, he recommends dropping the dose to 25 mg a day for 3 to 14 days.
PROS AND CONS. Diflucan is usually well tolerated. The principal side effects are nausea and other gastrointestinal complaints. Diflucan works very quickly, which means patients will see results almost immediately. For some patients this means an immediate improvement—for others, immediate side effects.
AVAILABILITY AND COST. Diflucan is available by prescription. The generic (fluconazole) costs roughly $1 a tablet. Insurance plans usually cover the cost (if your insurance does not include Diflucan, you may qualify for a compassionate low-cost supply; contact Pfizer, Inc., 866-706-2400 or, for an application form and more information go to: http://www.pfizerhelpfulanswers.com/pages/misc/Default.aspx
PATIENT REVIEWS
CFS/ME patient reviews of Diflucan: http://www.revolutionhealth.com/drugs-treatments/rating/diflucan-for-chronic-fatigue-syndrome-cfs-cfids-me
NIZORAL
Nizoral (ketoconazole) is somewhat similar to Diflucan but is used less frequently because of its serious side effects, including liver toxicity and endocrine system disturbances. Nizoral can also lower adrenal hormone levels. Although the drug is effective and inexpensive, many physicians are cautious about prescribing it. Patients taking Nizoral generally undergo blood tests, including a liver profile, every thirty days. Nizoral is available by prescription. A 30-day supply generally costs about $85. It is usually covered by insurance.
SPORANOX
USES IN CFS/ME. Like Diflucan and Nizoral, Sporanox is used to treat Candida overgrowth. Because it is less toxic to the liver, it is safer than Nizoral. Dr. Teitelbaum has observed that yeast that is resistant to Diflucan is usually resistant to Sporanox. The drug is generally well tolerated. The most common side effects are transient nausea and headache. As with Diflucan, Sporanox can cause liver inflammation. Dr. Teitelbaum recommends taking lipoic acid as a liver protector when taking either drug.
PROTOCOL: Doses range from 100 to 200 mg/day.
AVAILABILITY AND COST: Sporanox is available at most pharmacies. The cost of a month's supply of 100 mg tablets is roughly $450 brand, $250 for generic (itraconazole). Because the drug is expensive, it is advisable to check with your insurance carrier to see if it is covered.
PATIENT REVIEWS
CFS/ME patient reviews of Sporanox: http://www.revolutionhealth.com/drugs-treatments/rating/itraconazole-for-chronic-fatigue-syndrome-cfs-cfids-me
SEE: Candida
ANTIHISTAMINES
Benadryl, Claritin, Allegra, Zyrtec, Chlor-Trimeton, Atarax and Vistaril, Dramamine
DESCRIPTION. Antihistamines are a class of drugs that compete with histamine for cell receptor sites on effector cells, thereby blocking the effects of histamine.
BACKGROUND. Antihistamines have been used for many years to treat allergies and allergic reactions. Some antihistamines are also used to treat motion sickness and mild Parkinson's disease.
USES IN CFS/ME. Because many patients with CFS/ME have allergies (usually preceding but often developing after the onset of CFS/ME), antihistamines are often prescribed for relief of seasonal allergies. But in addition to allergies, patients with CFS/ME often develop an intolerance to histamine itself. (For this reason, anesthesiologist Patrick Glass recommends that CFS/ME patients avoid anesthetics containing histamine releasers, such as sodium pentothal, during surgery. For more tips on anesthesia see: http://www.squidoo.com/anesthesia-with-CFS)
Histamine is found in a number of foods, particularly fermented foods, and additives. Because histamine is a vasodilator, reactions to these foods and additives can mimic true allergies, producing flushing, lowered blood pressure, headache and palpitations. Aside from treating allergies, antihistamines are also of benefit in treating many other symptoms of CFS/ME, including insomnia, bladder problems (interstitial cystitis), anxiety, and muscle pain. Benefits are noted rapidly, usually within 24 hours.
BENADRYL (diphenhydramine)
USES IN CFS/ME. Benadryl is useful for treating hives, seasonal allergies, upper airway congestion, and severe allergic reactions (anaphylactic shock). The drug is very sedating and can be used as a sleep aid for CFS/ME-related insomnia if taken at bedtime. Like other antihistamines, Benadryl is not addictive, and thus may offer a good alternative to habit-forming sleeping pills. However, as Dr. David Bell points out in The Doctor's Guide to Chronic Fatigue Syndrome, Benadryl can lose effectiveness with continuous use for longer than a few weeks and therefore may be better used only occasionally.
Some patients note that, although Benadryl ensures a good night's sleep, rotating it with a benzodiazepine prevents developing a tolerance to either drug (see Benzodiazepines). Although Benadryl is generally well tolerated, adverse reactions – notably agitation and tachycardia – have been reported. If you are taking other medications, it is important to check with your physician before trying Benadryl, especially if you are prone to heartbeat irregularities.
AVAILABILITY AND COST. Benadryl is inexpensive, costing less than $7 per bottle or package. It is also available as a dye-free pill and in liquid form, which may be of benefit to CFS/ME patients with chemical sensitivities. Benadryl can be purchased without a prescription.
CLARITIN (loratadine)
USES IN CFS/ME. Claritin is a second-generation antihistamine useful in the treatment of seasonal allergy symptoms, such as runny nose, sneezing, itching, and watery eyes. Because it is very similar in structure to the tricyclic antidepressants, it may cause similar side effects (urinary retention, blurred vision, dry mouth, GI disturbances). In spite of being described as a “non-sedating” antihistamine, Claritin does produce drowsiness. Some patients have reported that they feel “zombie-like” after taking Claritin. Others report that Claritin has brought great relief from hay fever symptoms without adverse effects.
AVAILABILITY AND COST. Prescription strength Claritin is available over the counter at pharmacies supermarkets. A package of 24 gels costs roughly $20.
PATIENT REVIEWS
CFS/ME patient reviews of Claritin: http://www.revolutionhealth.com/drugs-treatments/rating/claritin-for-chronic-fatigue-syndrome-cfs-cfids-me
ALLEGRA (fexofenadine)
Fexofenadine is a second-generation antihistamine that does not readily cross the blood-brain barrier, and so causes less drowsiness than first-generation antihistamines (such as Benadryl). Like other antihistamines, it works by antagonizing the H1 receptor. As Allegra is non-sedating, it is recommended for patients who suffer from allergies, and who also have hypersomnia. Allegra comes in a tablet and as a liquid. Allegra works better if it is not taken with fruit juices such as orange, grapefruit, or apple juice. It is available over-the-counter at pharmacies and supermarkets. A package of 15 tablets costs roughly $7.
ZYRTEC (cetirizine)
Zyrtec is a second-generation antihistamine that crosses the blood-brain barrier only slightly, thereby reducing its sedating effects. In 2008 it was the highest grossing non-food product in the U.S., generating sales in excess of $300 million. Unlike other antihistamines, Zyrtec is only taken once a day, preferably at the same time. Paradoxically, Zyrtec D's (decongestant) stimulating effect may help insomnia. One CFS/ME patient reported that after suffering from frequent panic micro-arousals on a nightly basis, taking Zyrtec D actually helped her stay asleep. The Zyrtec elevated her metabolic rate, preventing the sudden release of adrenaline that was preventing her from getting into a deep sleep.
AVAILABILITY AND COST. Zyrtec is available at pharmacies and supermarkets. A package of 30 tablets costs roughly $20.
CHLOR-TRIMETON (chlorpheniramine maleate)
Chlorpheniramine is a first-generation antihistamine with relatively weak sedative effects. Chlorpheniramine is normally used to treat allergies, however, it also functions as a serotonin and norepinephrine reuptake inhibitor (SNRI). One patient with long-term CFS/ME reported that a dose of 2 mg of Chlor-Trimeton improved her sleep and she felt less miserable in the day. “There was less aching, less fatigue, a little more mental clarity.” After the drug effect reached a plateau, she increased the dose and noticed that all her symptoms improved, not just sleep disturbances (CFIDS Chronicle, Winter 1994).
AVAILABILITY AND COST. Chlor-Trimeton is available over the counter. It is relatively inexpensive at less than $8 for 24 tablets.
ATARAX, VISTARIL (hydroxyzine)
BACKGROUND. Hydroxyzine is an older first-generation antihistamine used for allergies, motion sickness, nausea and mild anxiety. Although it has sedative effects, it is not addictive, nor does it produce the side effects common to tranquilizers and anxiolytics. Hydroxyzine is frequently used in conjunction with opioid pain killers to increase the effectiveness of the drugs without increasing toxicity.
USES IN CFS/ME. Hydroxyzine has a wide range of uses in treating CFS/ME symptoms, including anxiety, pain and interstitial cystitis. Dr. Paul Cheney prescribes Vistaril to treat muscle pain (CFIDS Chronicle, Spring 1995).
Two physicians who specialize in treating interstitial cystitis, Dr. Grannum Sant and Dr. Theoharis Theoharides of Tufts University, have published several papers detailing the effectiveness of hydroxyzine. Dr. Theoharides noted that several patients given hydroxyzine experienced improvement in urinary frequency and bladder pain. He theorizes that this drug may inhibit secretion of mast cells, a type of cell involved in allergic reactions that may be responsible for many symptoms in interstitial cystitis. Dr. Theoharides states that hydroxyzine is unique in that other antihistamines do not seem to be effective in treating interstitial cystitis (Seminars in Urology, 1991). Symptoms often recur after discontinuation of the drug. However, the success rate is high and the risks low, compared with more invasive therapies for interstitial cystitis.
PROS AND CONS. Although Vistaril is often prescribed for anxiety, it can paradoxically cause panic and anxiety attacks. Some patients report that Vistaril “knocks them out,” which may be beneficial for people with insomnia.
PROTOCOL. The initial dosage is 25 mg a day, which can be slowly increased to 100 mg. Daytime sedation, the most common side effect, generally disappears in a few days. Hydroxyzine is fast-acting, with results seen within 30 minutes. When used for anxiety, its effectiveness is generally limited to a few months. Hydroxyzine is not recommended for the elderly.
AVAILABILITY AND COST. Atarax and Vistaril are available by prescription, in brand-name or generic formulations. The generic form of these drugs is inexpensive. Thirty tablets of 25 mg generic drug cost about $12.
DRAMAMINE (meclizine)
Meclizine is a first generation antihistamine very similar to hydroxyzine. It is used primarily to treat vertigo, dizziness, and motion sickness. In CFS/ME, it is frequently prescribed to treat vertigo as well as balance problems, nausea, motion sickness, and Meniere's disease. Dramamine is safe to use. The most common side effect is excessive sedation. DiVertigo, a natural herbal alternative to Dramamine can also be purchased at pharmacies, as well as health food stores. DiVertigo is a liquid blend of lavender peppermint, frankincense, chamomile, myrrh and ylang-ylang, which is rubbed behind the ear rather than swallowed.
AVAILABILITY AND COST. Over-the-counter Dramamine costs roughly $15 for 36 tablets. In-house pharmacy brands are considerably less expensive. DiVertigo costs roughly $20.
SEE: Allergies, Sleep Disturbances, Urinary Problems
REFERENCE
Theoharides TC, Sant GR. “Bladder mast cell activation in interstitial cystitis.” Semin Urol. 1991 May;9(2):74-87. http://www.ncbi.nlm.nih.gov/pubmed/1853017 (Abstract)
ANTIVIRAL AGENTS
Acyclovir, Famvir, Amantadine, Valacyclovir, Valganciclovir
DESCRIPTION. Antiviral agents are a group of drugs used to inhibit the replication of viruses.
USES IN CFS/ME. Most CFS/ME physicians in the United States adhere to the theory that CFS/ME is caused by a virus. Although the causal virus has not yet been identified, reactivated latent viral infections are not only quite common in CFS/ME patients, but highly problematic, as the reactivated viruses produce many of the symptoms characteristic of the illness. As a consequence, antivirals have a long track record in treating CFS/ME. Most CFS/ME doctors have incorporated antivirals of one kind or another into their protocols, particularly for patients with either high viral titers, or who have had a viral onset of the illness.
Dr. Guyer, Director of The Advanced Medical Center in Indianapolis, Indiana, uses antivirals for patients with viral onset of CFS/ME, that is, those patients who initially had mononucleosis, or “flu,” from which they never recovered. Dr. Guyer reports that these patients typically have lab findings of depressed natural killer cells, hormone deficiencies, elevated RNase L levels, and elevated antibodies to Human Herpesvirus 6 (HHV-6), cytomegalovirus (CMV), Epstein-Barr virus (EBV) and other viruses.
Several doctors have reported success with antiviral treatments for a subset of their patients. Dr. Lerner, an infectious disease specialist who has been investigating and treating CFS/ME for more than 20 years, found that long-term antiviral therapy was very effective for his patients with high viral titers, sometimes providing these patients with nearly full recovery.
ACYCLOVIR
BACKGROUND. In the early 1980s, acyclovir (Zovirax) was hailed as one of the first drugs to be proven effective against genital herpes. Although later shown to be not as universally helpful as researchers first thought, acyclovir does relieve the severity, duration, and frequency of outbreaks for many patients with genital herpes. Acyclovir is not a cure for the infection because it does not kill the virus but merely inhibits its ability to replicate. In addition to treating herpes simplex, which causes genital herpes, acyclovir has been used with some success to treat other types of herpesvirus infections, such as chickenpox (varicella zoster virus), shingles (herpes zoster), cytomegalovirus (CMV), and infectious mononucleosis (Epstein-Barr virus), among others.
USES IN CFS/ME. In the mid-1980s, Epstein-Barr virus was thought to be the cause of the illness now known as CFS/ME. Because Epstein-Barr virus is one of the herpesviruses, it was logical for acyclovir to be used to treat cases of what was then called chronic Epstein-Barr virus or chronic mononucleosis. At that time, physicians using acyclovir noted symptomatic improvement in many of their patients. However, the first formal study was not completed until 1988, when Dr. Steven Straus of the National Institutes of Health (NIH) headed a double-blind, placebo-controlled study to determine the effectiveness of acyclovir against CFS/ME. Dr. Straus' results revealed no difference between the placebo group and patients given acyclovir (New England Journal of Medicine, 1988).
Notwithstanding these inconclusive results, many physicians familiar with CFS/ME continue to prescribe acyclovir, citing both their success rate and the flawed methods of the Straus study as justifications. Dr. Charles Lapp, for example, reported “remarkable results with this medication.” Dr. Guyer, Director of The Advanced Medical Center in Indianapolis, Indiana, recommends acyclovir for patients with viral onset of CFS/ME (after mononucleosis or other viral infection), especially in the presence of high titers of herpesvirus, recurrent shingles, or other clinical evidence of viral infection (CFIDS Chronicle, Spring 1991).
PROTOCOL. The oral form is most commonly recommended because intravenous injections carry some risk of toxicity. Daily doses range from 800 to 4000 mg divided throughout the day. Topical creams or ointment can be applied directly to the skin to treat surface blisters and other lesions. Despite the associated risks, patients with acute infections may require intravenous administration. Because resistance can develop, 30- to 60-day intervals between courses of therapy are recommended to ensure continued effectiveness.
PROS AND CONS. Acyclovir, while not a cure for CFS/ME, may lessen the viral load in patients with CFS/ME who demonstrate a lot of viral activity (high titers of herpesvirus, recurrent flu-like symptoms, shingles). A number of patients with CFS/ME have reported success with acyclovir in controlling shingles and eliminating chronic sore throat.
In their book, CFIDS: An Owner's Manual, Barbara Brooks and Nancy Smith reported success with acyclovir, claiming it to be the most important component of their respective treatments. Positive results are far from universal, however. An equal number of patients with CFS/ME report little or no benefit, even after months of trial. For those who do receive some benefit, the results are generally short-lived. Many patients must take the drug daily to see any result at all. Acyclovir, although usually well tolerated, produces frequent side effects, notably light-headedness, nausea, and headache. Patients with kidney disease should not take acyclovir.
AVAILABILITY AND COST. Oral acyclovir is available by prescription. Oral acyclovir can be purchased for as little as $30 a month (200 mg tablets). Insurance plans usually cover the cost.
PATIENT REVIEWS
CFS/ME patient reviews of Zovirax: http://www.revolutionhealth.com/drugs-treatments/rating/zovirax-for-chronic-fatigue-syndrome-cfs-cfids-me
REFERENCES
Physician's Forum. CFIDS Chronicle, Vol 1, Issue 1, March 1991.
Straus, Steven, Dale, JK, Tobi, M, et al. “Acyclovir Treatment of the Chronic Fatigue Syndrome.” New England Journal of Medicine. 26:1692-1698,1988.
FAMVIR
Famvir (famcyclovir) is an oral antiviral used for herpesviruses, particularly herpesviruses 6 and 7, two viruses that play an important role in CFS/ME. Technically, Famvir is a prodrug; that is, a substance that is converted into an active drug once in the body. Famvir functions the same as Zovirax, but with fewer side effects. There is some indication that it may be more effective, as well.
Currently, only a few CFS/ME clinicians prescribe Famvir, so not much information is available as to its effectiveness in treating CFS/ME. Dr. Guyer has observed the patients who experience milder symptoms of shorter duration, accompanied by elevated levels of IgG to EBV, seem to do well with Famvir.
AVAILABILITY AND COST. Famvir is available by prescription. This drug is quite expensive. A one -month supply can cost as much as $700, depending on the dosage.
REFERENCE
“Dale Guyer, M.D., on Treating Chronic Fatigue Syndrome & Fibromyalgia: 'Covering the Bases & Peeling Back the Layers of the Onion.'” ProHealth.com. June 13, 2006 http://www.prohealth.com/library/showarticle.cfm?libid=9761
AMANTADINE
Amantadine (Symmetrel) is prescribed for viral infections (type A influenza virus) and Parkinson's disease. It acts by blocking the penetration of cell membranes by the infectious material from viruses. As an antiviral agent, it is of no benefit unless administered at the onset of infection. In patients with CFS/ME who cannot tolerate flu shots, amantadine might be a good alternative, especially for those patients susceptible to frequent episodes of influenza. In CFS/ME, its most common use is not as an antiviral agent but as a stimulant. It is used to treat fatigue and lethargy in mild cases. Common side effects include insomnia, confusion, headaches, and dizziness. Amantadine interacts with antidepressants and antihistamines. Some patients with CFS/ME cannot tolerate this drug so the initial dose should be small.
AVAILABILITY AND COST. Amantadine is available by prescription. A one-month supply of the generic amantadine costs approximately $12.
PATIENT REVIEWS
CFS/ME patient reviews of amantadine: http://www.revolutionhealth.com/drugs-treatments/rating/symmetrel-for-chronic-fatigue-syndrome-cfs-cfids-me
VALACYCLOVIR (Valtrex)
DESCRIPTION. Valacyclovir is an oral pro-drug that converts to acyclovir once ingested. It is more bioavailable than acyclovir and is therefore more effective.
BACKGROUND. Valtrex is marketed for herpes simplex, but in 2009 Hoshino et al found that it also reduced the replication of EBV. They concluded that latent EBV (Epstein-Barr virus) might be completely eradicated by Valtrex if reinfection did not occur.
USES IN CFS/ME. A 2007 study by Dr. Lerner of CFS/ME patients with EBV reactivation found that Valtrex resulted in both increased physical functioning and improved heart functioning (reduced sinus tachycardia, decreased abnormal cardiac wall movements) as well as reducing EBV antibody levels. By the end of the 36-month trial many patients were able to resume normal activities. Patients with both EBV and CMV infections did not improve.
PROTOCOL. Valtrex is prescribed at 2000 mg/day, and then reduced. Patients can expect to take it for over a year.
PROS AND CONS. Valtrex may be very effective for patients with high herpesvirus and EBV titers alone. It is less effective against HHV-6 than Valcyte.
AVAILABILITY AND COST. Valtrex is available with a prescription from most pharmacies. It is expensive. A one-month supply can cost upwards of $350.
PATIENT REVIEWS
CFS/ME patient reviews of Valtrex: http://www.revolutionhealth.com/drugs-treatments/rating/valtrex-for-chronic-fatigue-syndrome-cfs-cfids-me
VALGANCYCLOVIR (Valcyte)
DESCRIPTION: Valcyte is an antiviral drug approved for treating cytomegalovirus (CMV) infections. Valcyte is a prodrug, converting quickly to ganciclovir after oral administration.
USES IN CFS/ME. In 2001 and 2002, Lerner et al conducted small trials of Valcyte which showed that the drug reduced EBV titers and significantly improved the symptoms of a subset of patients. In 2007 Dr. Jose Montoya of Stanford Hospital Infectious Disease Clinic, conducted a double blinded placebo controlled clinical trial to determine whether CFS/ME patients with elevated antibody titers for HHV-6 and EBV would benefit from valganciclovir treatment. The trial enrollment was small (30 patients), however the study indicated that patients on Valcyte experienced significant cognitive improvement.
Valcyte is one of the newer antivirals, so there is not yet a lot of feedback on its success rate in the CFS/ME population. The Holtorf Medical Group in Torrance, California, has used Valcyte since 2003 for treating CFS/ME, and has found it to be effective in patients with “flu-like symptoms or having symptoms that started with a flu-like illness; elevated IgG or EA against Epstein bar virus, cytomegalovirus and/or HHV-6; low natural killer cell activity; high RNAse-L activity; high ACE (>35); coagulation activation; high tumor necrosis factor (TNF); low melanocyte stimulation hormone (MSH); high interleukin-6 (IL-6); low WBC; increased 1-25 vitamin D/25 vitamin D ratio and/or elevated or decreased total IgA, IgM or IgG levels.” In the absence of similar testing, it would be difficult to evaluate which patient sub-group would best benefit from Valcyte.
PROS AND CONS. Patients who have taken Valcyte for several months have reported significant side effects, including muscle weakness, flu-like symptoms and joint pain in spite of a dramatic decline in viral titers. Nearly all patients feel significantly worse for the first two to four weeks. Valcyte is prohibitively expensive. A one-month supply costs between $1500 and $2000.
SEE: In Search of a Cause
FURTHER READING
Summary of Valtrex studies: http://aboutmecfs.org.violet.arvixe.com/Trt/TrtValtrex.aspx
Summary of Dr. Lerner's antiviral research and treatment of CFS/ME patients. http://aboutmecfs.org.violet.arvixe.com/Int/Lerner.aspx
Dr. Guyer discusses his antiviral protocol: http://www.prohealth.com/library/showarticle.cfm?libid=13222
RESEARCH
Lerner, A Martin, Safedin Beqaj, James T Fitzgerald, Ken Gill, Carol Gill, James Edington. “Subset- directed antiviral treatment of 142 herpesvirus patients with chronic fatigue syndrome.” Dovepress Journal: May 2010 Volume 2010:2 Pages 47 – 57
ARTESUNATE (Hepasunate)
DESCRIPTION. Artesunate is a semi-synthetic anti-malarial drug derived from artemisia annua (wormwood).
BACKGROUND. While artemisia has been used for centuries as an herbal anti-parasitic, it wasn't until the 1960s that Chinese scientists developed an artemisinin drug to combat malaria. Since then, artesunate and other artemisia-based drugs have been used worldwide to combat malaria. However, it was not until 2007 that the FDA approved artesunate for the treatment of severe malaria in the United States. The action of artesunate is still unclear, but it is thought to kill the parasite by destroying its mitochondrial membrane.
USES IN CFS/ME. Recent cell studies indicate that artesunate significantly reduces viral protein production in HHV-6 infected cells. An in vitro study in 2005 confirmed that artesunate also significantly reduces cytomegalovirus (CMV) replication in cells. Because so many CFS/ME patients test positive for HHV-6 and CMV reactivation, artesunate may provide a means to control, if not eliminate, the symptoms associated with the proliferation of the viruses. Although this drug is experimental, some doctors are using it to treat CFS/ME, with positive results. Dr. Cheney has observed a reduction in viral titers, and a cessation of diastolic heart dysfunction.
PROTOCOL. Dr. Cheney puts his patients on 50 mg of Hepasunate (the form of artesunate available for online purchase) three days a week (empty ½ capsule under the tongue, hold for a minute, swish, and spit), and wormwood elixir 4 days a week (½ tsp in water, swish and spit).
PROS AND CONS. This supplement is highly experimental for CFS/ME, which means that few doctors use it, and, as a consequence, patients who take it independently may not be monitored for side effects, toxicity, or drug interactions.
As one might expect, reports from patients who have tried artesunate are mixed. Some report a significant reduction in fatigue and flu-like symptoms. Others report dizziness, diarrhea and malaise. There is no way of determining from these reports whether the side effects (or improvements) are due to the dosage, brand or, perhaps, completely independent factors. This is a “use at your own risk” medication, so you are advised to exercise caution and go slowly. The twice a week swish and spit method is the gentlest way to introduce artesunate.
AVAILABILITY AND COST. Hepasunate (the brand Dr. Cheney uses) can be purchased online for $50 for a bottle of 50 capsules. Before trying artesunate, please read the following Phoenix Rising forum discussing the experiences of patients who have followed Dr. Cheney's artesunate protocol. It contains details of the experiences of patients who have taken artesunate, as well as links to useful articles.
FURTHER READING
CFS/ME patient forum on artesunate: http://forums.phoenixrising.me/showthread.php?601-Artesunate-Cheney-dosage-and-benefits
This thread provides detailed information about side effects, dosage, and efficacy.
Supplier of Hepasunate in the U.S.: http://www.hepalin.com/hepasunate50.htm
Efferth, Thomas, Marta R. Romero, Dana G. Wolf, Thomas Stamminger, Jose J. G. Marin, and Manfred Marschall. “The Antiviral Activities of Artemisinin and Artesunate.” Clin Infect Dis. (2008) 47 (6):804-811. http://cid.oxfordjournals.org/content/47/6/804.long
This is an excellent article on the history, mechanisms and effects of artesunate.
RESEARCH
Auerochs S, Korn K, Marschall M. “A reporter system for Epstein-Barr virus (EBV) lytic replication: anti-EBV activity of the broad anti-herpesviral drug artesunate.” J Virol Methods. 2011 May;173(2):334-9. Epub 2011 Mar 17. http://www.ncbi.nlm.nih.gov/pubmed/21396962
Chou S, Marousek G, Auerochs S, Stamminger T, Milbradt J, Marschall M. “The unique antiviral activity of artesunate is broadly effective against human cytomegaloviruses including therapy-resistant mutants.” Antiviral Res. 2011 Nov;92(2):364-8. http://www.ncbi.nlm.nih.gov/pubmed/21843554
Efferth T, Kaina B. “Toxicity of the antimalarial artemisinin and its derivatives.” Crit Rev Toxicol. 2010 May;40(5):405-21. http://www.ncbi.nlm.nih.gov/pubmed/20158370
Gordi T, Lepist EI. “Artemisinin derivatives: toxic for laboratory animals, safe for humans?” Toxicol Lett. 2004 Mar 1;147(2):99-107.
Milbradt J, Auerochs S, Korn K, Marschall M. “Sensitivity of human herpesvirus 6 and other human herpesviruses to the broad-spectrum antiinfective drug artesunate.” J Clin Virol. 2009 Sep;46(1):24-8. http://www.ncbi.nlm.nih.gov/pubmed/19501020
BENZODIAZEPINES
Klonopin (clonazepam), Valium (diazepam), Xanax (alprazolam)
DESCRIPTION. Benzodiazepines are central nervous system depressants. They are classed as minor tranquilizers. Benzodiazepines comprise a very large group of drugs, with over 30 distinct formulations, and nearly 100 brand names.
BACKGROUND. The benzodiazepines are a group of drugs used to treat anxiety, skeletal muscle spasm, insomnia, and panic. Their calming effect is produced by a general slowing of the central nervous system. Within a decade of their introduction on the market, they had become one of the most frequently prescribed medications in the United States and, by the late 1980s, more than 10% of the U.S. population had taken some form of tranquilizer.
Although the benzodiazepines do not pose as many problems as the major tranquilizers, they also produce tolerance and dependence. Benzodiazepines can be classified into two main groups, depending on their half-life (how long it takes to clear half the drug from the body). In general, the shorter acting benzodiazepines (with a half-life of 4 to 20 hours) are more habit forming than those with a longer half-life (24 to 72 hours). In cases where dependence develops, doses should be tapered off slowly to avert withdrawal symptoms (anxiety, jitters, insomnia, confusion, sweating, heart palpitations, and depression).
USES IN CFS/ME. The benzodiazepines are frequently prescribed, often in combination with a small dose of antidepressant, to treat insomnia. The logic behind prescribing both drugs is that one gets you to sleep and the other keeps you asleep. The majority of CFS/ME physicians also recommend some form of benzodiazepine for patients with panic disorder or agitation due to upregulation of the sympathetic nervous system.
It is important to note that benzodiazepines are usually prescribed in small doses to treat CFS/ME. Normal doses of these drugs can produce paradoxical reactions, creating the very symptoms the drug is supposed to control. Even tiny doses can produce adverse reactions in patients hypersensitive to chemicals and drugs. It may be worthwhile to do a toothpick test (crush the pill and take only what clings to the end of a moistened toothpick) before embarking on a full program.
KLONOPIN (in Canada, Rivotril) (clonazepam)
BACKGROUND. Klonopin (clonazepam) acts directly on the limbic system, thalamus, and hypothalamus to produce anticonvulsant effects. It has been used since the late 1970s to control seizures. Klonopin is easily absorbed through the digestive tract and has a half-life of 24 to 72 hours. Effects are noticeable within 20 minutes and can last for 12 hours.
USES IN CFS/ME. Klonopin is the most widely recommended benzodiazepine for patients with CFS/ME. Dr. Cheney, a long-time proponent of the benefits of Klonopin, prescribes it to protect the brain against what he calls “excitatory neurotoxicity.” Most CFS/ME patients have excess amounts of neuroexcitatory neurotransmitters in their nervous systems, resulting in a brain which is overstimulated. The “tired and wired” feeling CFS/ME patients so often describe is the result of this excess stimulation. Because Klonopin is so long-acting, it serves to down regulate the nervous system. Klonopin is also beneficial for treating insomnia, especially if taken in conjunction with Sinequan. A number of patients have reported that Klonopin helps improve cognitive symptoms, particularly poor concentration and “brain fog.” Some patients also report that Klonopin helps alleviate flu-like achiness.
PROTOCOL. The dose recommended to treat CFS/ME-related insomnia is low, generally 0.5 to 1 mg taken before bedtime for insomnia. Dr. Cheney also recommends daytime doses of a quarter of a tablet to increase energy and concentration.
PROS AND CONS. The side effects of Klonopin are mild, especially compared to those of some of the other benzodiazepines. Some patients with CFS/ME, however, experience sedation, excessive thirst, depression, and gastrointestinal upset even with small doses. Like all benzodiazepines, it loses its efficacy over time. If taken for longer than a month, Klonopin should not be discontinued suddenly. On the positive side, Klonopin appears to be well tolerated by many patients with CFS/ME. Patients report that the generic form is less effective than brand.
AVAILABILITY AND COST. Klonopin is available by prescription. A 30-day supply of the generic drug (clonazepam, 0.5 mg) costs about $2. The cost is usually covered by insurance (but check for time limitations).
PATIENT REVIEWS
CFS/ME patient reviews of Klonopin: http://www.revolutionhealth.com/drugs-treatments/rating/klonopin-for-chronic-fatigue-syndrome-cfs-cfids-me
VALIUM
BACKGROUND. Valium (diazepam) was introduced in the United States in 1963. It acts by depressing the area of the central nervous system that controls the emotions (limbic system). It is also used as an anticonvulsant in patients with epileptic seizures and to relieve skeletal muscle spasms. Side effects from long-term use can include depression, drowsiness, lethargy, fainting, slurred speech, tremor, blurred or double vision, gastrointestinal disorders, nausea, and respiratory depression. It has a half-life of 20 to 50 hours. Onset occurs within 30 minutes to an hour, with peak action in 1 to 2 hours.
USES IN CFS/ME. Valium is less frequently recommended than Klonopin, nevertheless some people have found it to be very effective. In most cases, Valium is used for insomnia. It is taken just before bed. As with Klonopin, it should be taken at the lowest possible dose. If side effects or tolerance develop, Valium should be eliminated by slowly tapering off the dose.
AVAILABILITY AND COST. Valium is available by prescription. A one-month supply (30 tablets) of the generic drug at the lowest dose (2 mg) costs about $15.
XANAX
BACKGROUND. Xanax (alprazolam) was introduced in 1982 to treat anxiety, muscle spasms, and insomnia. It is also widely prescribed to treat panic attacks, agitated depression, and phobias. Xanax is more rapidly metabolized and eliminated than other benzodiazepines and causes less “hangover.” It has a half-life of 12 to 15 hours, rapid onset (about 15 minutes), and its peak action occurs within 1 to 2 hours.
USES IN CFS/ME. Because Xanax acts so quickly, it is usually recommended to treat panic and anxiety attacks. It is not often prescribed for persistent insomnia, although it may be recommended on a short-term basis. As with other benzodiazepines, Xanax should be taken at the lowest possible dose. It is not recommended as a daily medication, but only as needed to alleviate the effects of panic or anxiety due to overactive nervous system responses. It is highly addictive.
AVAILABILITY AND COST. Xanax is available by prescription. It is inexpensive; a supply of 30 tablets of the generic drug (alprazolam) at the lowest dose (0.25 mg) costs about $7.
SEE: Cognitive and Emotional Symptoms, Sleep Disorders
PATIENT REVIEWS
CFS/ME patient reviews of Xanax: http://www.revolutionhealth.com/drugs-treatments/rating/xanax-for-chronic-fatigue-syndrome-cfs-cfids-me
BETA BLOCKERS
Propanolol (Inderol), Atenolol (Tenormin), Labetalol (Normodyne), Nebivolol (Bystolic)
DESCRIPTION. Beta blockers slow heart activity by interfering with adrenal hormones.
BACKGROUND. Beta blockers are used primarily to treat angina and high blood pressure, and to control irregular heartbeat in damaged hearts. They can also be used to prevent migraine headaches, control ocular fluid pressure, and reduce anxiety. Beta blockers work by occupying the specific receptors in the heart, airways, and blood vessels (beta1 and beta2 adrenergic receptors) designed to receive the stimulating neurohormone, norepinephrine. By preventing the action of norepinephrine, beta blockers reduce the force and rate of heartbeats and prevent dilation of blood vessels surrounding the brain and of the airways leading to the lungs. The action of most beta blockers makes them useful for treating neurally mediated hypotension (NMH), an abnormal reflex interaction between the heart and brain. Patients with NMH experience sudden drops in blood pressure, leaving them feeling faint and weak. Beta blockers are used to help maintain constant blood pressure in NMH.
USES IN CFS/ME. According to Dr. Lapp, various forms of dysautonomia (including NMH), postural orthostatic tachycardia syndrome (POTS), and other forms of orthostatic intolerance occur in 96% of CFS/ME patients. Researchers of the Northern CFS/ME Clinical Network and Newcastle University found that POTS is three times more likely to occur in CFS/ME patients than in the general population. And researchers at Johns Hopkins University have published findings that seem to demonstrate a link between CFS/ME and NMH. Beta blockers have been prescribed to treat to treat low blood pressure common in CFS/ME, NMH and POTS as well as idiosyncratic heart problems (palpitations, mitral valve prolapse, and rapid or irregular heartbeat) and, in some circumstances, anxiety and headaches.
PROTOCOL. The beta blockers usually recommended for NMH are propranolol and atenolol (Tenormin). CFS/ME doctors recommend a very low dose. Beta blockers are normally prescribed as part of a program that includes increased intake of dietary salt and Florinef (fludrocortisone), a steroid drug (see Florinef). Beta blockers should not be taken with any food, drug, or other medication that contains caffeine or alcohol because the combination may increase heart rate or blood pressure. Dr. Light proposes that low-dose Nordyne, a combined alpha and beta adrenergic antagonist used to treat high blood pressure, might be of benefit for patients who don't respond to propanolol.
PROS. In 1995 a Johns Hopkins University study led by Issam Bou-Holaigah and Peter Rowe created quite a stir in the CFS/ME community (Journal of the American Medical Association, 1995). Of the 22 patients with CFS/ME and NMH treated in this study, nine reported full recovery and seven noted some improvement on beta blockers. (However, it should be noted that not all of these patients received beta blockers; some were given only Florinef.) These initial results were encouraging. Reports from CFS patients have since been mixed, but some claim substantial improvement from beta blockers.
CONS. Symptoms of CFS/ME do not always respond favorably to beta blockers. Some patients report little or no effect. A little over 50% report that symptoms actually get worse. Moreover, long-term and severe cases have not shown substantial improvement using this regimen. Beta blockers can cause the very symptoms they are supposed to alleviate: orthostatic hypotension (the feeling of fainting on standing), fatigue, dizziness, light-headedness, depression, and headaches.
Other common side effects include drowsiness, decreased sex drive, nervousness, depression, nightmares, upset stomach, constipation, and diarrhea. An additional consideration for those who have taken beta blockers for a long period of time is that the drug should not be discontinued suddenly but should be tapered off gradually over several weeks to avert irregularities in heart rate. People with poor circulation in the arms and legs, a frequent problem in CFS/ME, are also cautioned not to take beta blockers because these drugs make the problem worse. Beta blockers may also lower melatonin levels in the body, which may lead to insomnia. Those with mast cell disorders should not take beta blockers.
AVAILABILITY AND COST. Beta blockers are available by prescription. The cost ranges from $4 a month for the older beta blockers to $10 a month for the newer ones. Beta blockers are usually covered by insurance.
FURTHER READING
Dr. Lapp on orthostatic intolerance: http://www.cfids.org/about-cfids/diagnostic-testing.asp
CFIDS Association of America's review of medications used to treat orthostatic intolerance. http://www.cfids.org/cfidslink/2009/070104.asp
Survey of CFS/ME patients using beta blockers: http://www.cfidsresearch.com/2011/02/22/beta-blockers/
PATIENT REVIEWS
A patient's experience with atenolol: http://www.revolutionhealth.com/drugs-treatments/rating/tenormin-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Bou-Holaigah, Issam, Rowe, Peter C, Ran, Jean, and Calkins, Hugh. “The Relationship Between Neurally Mediated Hypotension and the Chronic Fatigue Syndrome.” Journal of the American Medical Association. 274(12):961-967,1995. http://www.ncbi.nlm.nih.gov/pubmed/7674527 (Abstract)
Raj, Satish MS, Bonnie Black, RN, Italo Biaggioni MD, Sachin Y. Paranjape, Maricelle Ramirez, William D. Dupont, PhD, David Robertson, MD. “Propranolol Decreases Tachycardia and Improves Symptoms in the Postural Tachycardia Syndrome: Less is More.” Circulation. 2009; 120: 725-734. http://circ.ahajournals.org/content/120/9/725.full
CALCIUM CHANNEL BLOCKERS
Nicardipine, Nimodipine, Nifedipine, Verapamil
DESCRIPTION. Calcium channel blockers inhibit the transmembrane influx of calcium ions into cardiac and smooth muscle.
BACKGROUND. Calcium channel blockers work by preventing calcium ions from entering smooth muscle cells. Calcium is especially important for the functioning of these cells and specialized cells in the heart. When calcium levels are lowered, the result is a relaxation of blood vessels, allowing an increased supply of blood and oxygen to the heart while decreasing its work load. As a consequence of their effect on blood vessels, calcium channel blockers are useful in treating cardiovascular disorders, such as angina (chest pain) and coronary artery disease, and to lower blood pressure. These drugs also may improve exercise capacity and subsequently reduce the need for surgery in patients with cardiac problems.
USES IN CFS/ME. At the 1990 CFIDS conference in Los Angeles, Dr. Ismael Mena presented evidence of cerebral dysfunction in patients with CFS/ME. Using neurological spectroscopic scanning techniques, Dr. Mena reported that 71% of CFS/ME patients have low blood flow (hypoperfusion) in the temporal lobe of the brain. He further reported that after treatment with calcium channel blockers, some of these patients exhibited clinically improved cerebral blood flow (CFIDS Chronicle, Spring/Summer 1990).
A number of CFS/ME clinicians have noted improvement in cognitive function in patients given calcium channel blockers. Cardene also is helpful in treating migraine-type headaches. Dr. Jay Goldstein also observed improvements in cognitive function and energy level in patients given calcium channel blockers. He also noted increased exercise tolerance, decreased tender point sensitivity, and alleviation of panic disorder with nimodipine.
In October 1994, Dr. Robert Keller, Medical Director of the Center for Special Immunology in Miami, reported improvement of symptoms in 25 patients with CFS/ME after treatment with the calcium channel blocker verapamil. Within one month of finding the optimal dose of verapamil, patients reported improvement in fatigue, memory, and myalgia. Dr. Keller also reported a decrease in the number of activated T cells, demonstrating that calcium channel blockers may have some immunomodulatory properties.
In 2000, Chauduri et al correlated the symptoms of CFS/ME, particularly fluctuating fatigue, with abnormal ion channel function. This finding appears to have been borne out by an interesting double-blind study carried out by Dr. Weibe, in which a patient reported dramatic declines in fatigue, sleep disturbance, pain and mental “fog” after being given nimodipine as opposed to placebo.
PROTOCOL. The most commonly prescribed calcium channel blockers in patients with CFS/ME are nimodipine, nicardipine, and verapamil. Doses must be individualized for each patient, but generally are quite low.
Nimodipine 30 mg, 2 or 3 times daily
Nicardipine 20 mg, 2 or 3 times daily
Verapamil 120 to 240 mg, taken nightly
PROS. Symptomatic relief can be obtained quickly with calcium channel blockers; therefore a trial is often worthwhile in many cases, even in the absence of a single-photon emission computed tomography (SPECT) scan. Improved cognitive function, fewer headaches, increased energy, and decreased muscle spasms have all been reported with use of these drugs.
CONS. Although calcium channel blockers can be effective for some of the more problematic CFS/ME symptoms (e.g., cognitive dysfunction), side effects can be a problem. The most common are lowered blood pressure (which can be serious if blood pressure is already low), severe pressure headaches, dizziness, gastrointestinal problems (diarrhea, constipation), and weakness. In addition, hypertensive effects can be exaggerated by concomitant use of other drugs that affect blood pressure, such as beta blockers. Tagamet (cimetidine) also increases the effects of calcium channel blockers. The use of calcium channel blockers requires close supervision by a physician due to their effects on blood pressure. Most CFS/ME doctors do not include calcium channel blockers in their protocols, except for patients who have high blood pressure. Not recommended for people with a history of kidney problems.
AVAILABILITY AND COST. Calcium channel blockers are available by prescription. Nimodipine is expensive, costing between $1.75 and $5.00 a pill. Nicardipine and verapamil are much less expensive, about $10 - $15 for 30 tablets. Insurance usually covers.
FURTHER READING
A detailed discussion by Cort Johnson of the role ion channels play in CFS. http://aboutmecfs.org.violet.arvixe.com/Rsrch/NeurologicalChannelopathy.aspx
Weibe, E. “Managing Chronic Fatigue Syndrome: Two Case Reports.” Can Fam Physician.1996 November;42: 2214–2217. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2146911/?page=1
RESEARCH
Chaudhuri, A., W.S. Watson, J. Pearn and P.O. Behan. “The Symptoms of Chronic Fatigue Syndrome are Related to Abnormal Ion Channel Function.” Med Hypotheses. 2000 Jan;54(1):59-63. http://www.ncbi.nlm.nih.gov/pubmed/10790725 (Abstract)
CENTRAL NERVOUS SYSTEM STIMULANTS
Ritalin, Dexedrine, Lonamin, Provigil, Strattera
DESCRIPTION. Central nervous system (CNS) stimulants are a class of drugs that, much like the amphetamines, speed CNS responses by releasing stored norepinephrine from nerve terminals in the brain.
BACKGROUND. CNS stimulants have played an important role in human history. The cultivation of chocolate, which contains small amounts of caffeine (a xanthine alkaloid) goes back to 1100 B.C. Chocolate's reputation as an aphrodisiac is, no doubt, partially due to its stimulating effects. Tea, which contains about 3% caffeine, has been under cultivation since the 10th century B.C. Coffee, which is approximately 1.2% caffeine, has been consumed as a stimulant since the 13th century. In fact, coffee was so stimulating that it was banned under Charles II, who blamed the drink for inciting the people to sedition. (Pope Clement VIII also banned coffee until it was revealed that he himself was a major importer of the “devil's drink,” whereupon he immediately baptized the brew, making it safe to drink.)
In the 19th and early 20th century, cocaine, another CNS stimulant, was used to treat depression. Sigmund Freud, an early proponent of the curative powers of cocaine, recommended cocaine as a cure for depression, sexual impotence, and as an anesthetic. Amphetamines, first synthesized in 1887, were used for asthma, and in the 1940s became widely used for weight loss. By the 1960s CNS stimulants were prescribed as treatments for a variety of disorders, including hyperactivity, depression, and attention deficit disorder (ADD). In 2004 the FDA approved the stimulant modafinil (Provigil) for the treatment of narcolepsy.
USES IN CFS/ME. CNS stimulants are generally used to increase energy and cognitive function. The drug most commonly recommended for CFS/ME patients is Ritalin (methylphenidate), although Dexedrine (dextroamphetamine) is also sometimes prescribed. Lonamin (phentermine), a mild CNS stimulant that activates dopamine in the brain, is sometimes recommended in CFS/ME patients with hypersomnia or significant cognitive impairment. The mild stimulation induced by a low dose of any of these drugs can often dispel feelings of lethargy and “brain fog” and, because effects are so immediate, they can act as a quick fix in an emergency.
While there is great appeal in seeing immediate improvement in energy levels and cognitive function, most CFS/ME clinicians prescribe these drugs with caution. Dr. Cheney believes that the disabling fatigue of CFS/ME may be a protective mechanism. Therefore, creating energy artificially may in the long run cause relapse and may even exacerbate the disease process.
PROTOCOL. Dosage varies according to the individual needs of the patient, as determined by a physician. Patients with CFS/ME, however, are advised to start with the smallest dosage to avert the negative effects of overstimulation. Dexedrine, for example, is prescribed at the lower than usual dose of 5 to 10 mg. Lonamin dosage varies between 15 and 30 mg (taken in the morning).
For the subset of CFS/ME patients with fibromyalgia, Dr. Bateman recommends Adderall, starting with the lowest dosage and working up to 5-20 mg. two to three times a day. Dr. Bateman also uses Provigil (modafinil) 50-400 mg (long-acting) as well as Wellbutrin, a stimulant antidepressant.
Dr. Lapp recommends using low doses of CNS stimulants such as Ritalin, Adderall or Provigil for fatigue. Dr. Lapp has found that “Provigil not only improves fatigue, but also somnolence, mental clarity, attention deficits, and depression."
Surprisingly, while Dr. Teitelbaum advises that CFS/ME patients steer clear of coffee, he recommends 10-30 mg of Ritalin taken three times a day up to a maximum of 60 mg/day. Dr. Teitelbaum observes that “the medications ritalin and dexedrine can be very helpful at lower doses in those with chronic fatigue syndrome, as they help stabilize the low blood pressure and the low dopamine levels found in chronic fatigue syndrome.”
Dr. Rowe recommends that ME/CFS patients with orthostatic intolerance take low doses of vasoconstrictor medications, including Ritalin and Dexedrine to treat blood pooling. He recommends 5 mg in the morning repeated, if necessary, four hours later.
PROS. It appears that the less ill the patient the better the response. The boost received from these drugs may enable patients with mild symptoms to work full-time or part-time. Most people use CNS stimulants on an "as needed" basis to provide extra energy on particularly long or important days. Many patients report a lessening of “brain fog” as well as increased focus and stamina. Doses for these patients have been very small.
CONS. Whereas CNS stimulants have been effective in some patients, they are of modest to little benefit for most. Stimulants, while appearing to provide more energy, tax the system. As a consequence, they are beneficial only if the system is strong to begin with. A number of patients report feeling much worse while taking stimulants. The most common side effects are anxiety, excitation, insomnia, gastrointestinal problems, dizziness, headache, palpitations, dry throat, appetite loss, chest pain, and hypertension. Patients also report that Ritalin causes anxiety and paranoia. With nearly all CNS stimulants, patients report rebound fatigue after the drug wears off.
As with other medications that affect the CNS, some patients experience a paradoxical reaction of extreme fatigue and weakness. Drug interactions are numerous, including antidepressants (especially MAOIs), anticonvulsants, and caffeine. As with MAOIs, foods high in tyramine should be avoided (see Urinary Tract Problems). CNS stimulants are contraindicated in patients with cardiovascular disease or hyperthyroidism.
AVAILABILITY AND COST. CNS stimulants are available by prescription, either as brand name or generic drug. Most of the older varieties are fairly inexpensive. Ritalin, for example, costs about $25 a month. Provigil, a newer drug, costs upwards of $250 a month. Insurance usually reimburses the cost.
FURTHER READING
Dr. Bateman's protocol, including stimulants: http://www.offerutah.org/cfsmetreatment.htm
Drs. Bateman, Natelson, and Lapp discuss CNS stimulant protocols for fibromyalgia and CFS/ME. http://www.fmnetnews.com/articles-hot.php
Summary of CNS stimulants used for CFS/ME patients: http://phoenixrising.me/?page_id=2299
Summary of Provigil's use in CFS/ME: http://phoenixrising.me/?page_id=4803
Summary of dexedrine's use in CFS/ME: http://phoenixrising.me/?page_id=4762
Effects of caffeine and CNS stimulants on patients with CFS/ME. Observations on use of CNS stimulants by Drs. Teitelbaum and Papernik: http://www.everydayhealth.com/chronic-fatigue-syndrome/relief-with-caffeine.aspx
PATIENT REVIEWS
CFS/ME patient ratings of Adderall: http://www.revolutionhealth.com/drugs-treatments/rating/adderall-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of dexedrine: http://www.revolutionhealth.com/drugs-treatments/rating/dexedrine-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of methylphenidate (Ritalin and Concerta). http://www.revolutionhealth.com/drugs-treatments/rating/methylphenidate-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of phentermine: http://www.revolutionhealth.com/drugs-treatments/rating/phentermine-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Provigil: http://www.revolutionhealth.com/drugs-treatments/rating/provigil-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Strattera: http://www.revolutionhealth.com/drugs-treatments/rating/pamelor-for-chronic-fatigue-syndrome-cfs-cfids-me
CYTOTEC (misoprostol)
CAUTION: Do not take Cytotec during pregnancy.
DESCRIPTION. Cytotec (misoprostol) is a synthetic prostaglandin analogue that replaces depleted gastric prostaglandins.
BACKGROUND. Cytotec is routinely used to prevent gastric ulcers in elderly or debilitated patients who are receiving nonsteroidal anti-inflammatory drug (NSAID) therapy. In these patients, the actions of natural prostaglandins (hormone-like substances that regulate inflammation, blood vessel dilation, and a host of other physiological responses) are blocked.
USES IN CFS/ME. Cytotec is primarily recommended for patients who are taking non-steroidal anti-inflammatory drugs (NSAIDs). Cytotec not only protects the stomach lining from the damaging effects of pain killers, it also appears to protect the small intestines. Dr. Leo Galland believes the drug can prevent “leaky gut,” a condition in which the small intestine becomes overly permeable, thereby leading to food sensitivities and allergies. Cytotec is also used to treat Interstitial Cystitis (IC), a condition experienced by many people with CFS/ME. In 1998 Kelly et al found that 24 out of 25 patients with IC improved after receiving misoprostol, with minimal side effects.
PROTOCOL. Physicians recommend taking four 100 mcg tablets a day (one with each of three meals and one before bedtime). When reducing dosage, the bedtime dose should be the last tablet eliminated.
PROS AND CONS. Patients who have taken Cytotec to treat the symptoms of IC describe it as a “miracle.” Many patients who have tried Cytotec for food sensitivities report an increase in the number of foods they can tolerate and a decrease in related gastrointestinal symptoms. Patients with severe food intolerance have noted sustained improvement even after eventually discontinuing Cytotec. Cytotec has relatively few side effects. The most common side effects are diarrhea, flatulence, nausea, headache, and, rarely, vaginal bleeding. If side effects last longer than a week or are severe, the dosage should be lowered. Cytotec is contraindicated in pregnant women, because it may induce miscarriage.
AVAILABILITY AND COST. 100 pills of the generic cost between $30 and $55. Cytotec is available by prescription, and the cost is covered by most insurance plans. Uninsured patients may meet the manufacturer's criteria for its "Patients in Need" program and qualify for a free supply (contact Searle, 5200 Old Orchard Rd., Skokie, IL 60077; 800-542-2526).
FURTHER READING
A general review of the therapeutic uses of misoprostol. http://www.ncbi.nlm.nih.gov/pubmed/11191738
RESEARCH
Kelly JD, Young MR, Johnston SR, Keane PF. “Clinical response to an oral prostaglandin analogue in patients with interstitial cystitis.” Eur Urol. 1998;34(1):53-6. http://www.ncbi.nlm.nih.gov/pubmed/9676414 (Abstract)
DIAMOX
DESCRIPTION. Diamox (acetazolamide) is a carbonic anhydrase inhibitor.
BACKGROUND. Diamox was introduced in 1953 as a diuretic. Because it reduces intraocular pressure, it is used to treat glaucoma. Diamox can also be used to treat edema, high-altitude sickness, and as an anticonvulsant. Diamox blocks the action of carbonic anhydrase, an enzyme that helps form hydrogen and bicarbonate ions from carbon dioxide and water. It promotes excretion of sodium, potassium, water, and bicarbonate. By blocking carbonic anhydrase in the central nervous system and increasing carbon dioxide tension, Diamox also helps decrease abnormal neuronal discharge that may lead to convulsions. Because Diamox lowers blood pH, and encourages respiration, it has been prescribed to help with sleep apnea as well. Other uses include absence seizures, periodic paralysis and congestive heart failure.
USES IN CFS/ME. Dr. Cheney has found Diamox very useful to treat pressure-type headaches in CFS/ME patients. He also found that it helped balance problems, and, over time, improved neurocognitive function, as it increases blood flow to the brain. Patients taking Diamox often report increased energy.
PROTOCOL. Diamox usually is prescribed at 250 mg to be taken two or three times a day. The Academy of Medicine of New Jersey recommends 500 mg of Diamox prior to bedtime to lower cerebral spinal blood pressure in patients with headaches. In A Doctor's Guide to Chronic Fatigue Syndrome, Dr. Bell advises starting Diamox at very low doses. He recommends using this drug with caution and discontinuing if side effects should appear. Because Diamox is a diuretic, potassium supplementation or potassium-rich foods (bananas and apricots) may be necessary. Diamox can be taken with food to lessen the chance of nausea or stomach irritation.
PROS AND CONS. For severe, hard-to-treat headaches, Diamox can be a real boon. It is also one of the few drugs that can actively help with cognitive impairment. Diamox acts within a couple of weeks; therefore, a long trial is not necessary. On the negative side, it can create metabolic acidosis, weakness, skin tingling, loss of appetite, and near-sightedness; may cause allergic reactions in people allergic to sulfa drugs; and may activate gout or cause syndromes similar to lupus if taken for extended periods. Diamox can increase the effects of tricyclic antidepressants. Not recommended for patients with kidney stones.
AVAILABILITY AND COST. Diamox is available by prescription only. It is inexpensive. A one-month supply costs roughly $10. Insurance usually covers.
SEE: Headaches
FURTHER READING
The Academy of Medicine of New Jersey's 2002 manual on treating CFS/ME. http://www.njcfsa.org/Manual.pdf
The 1995 Cheney lectures. http://homepage.mac.com/doctormark/Medical/CFS/CFSpapers/cheneylecturescfs.html
EPOGEN (PROCRIT)
DESCRIPTION. Epogen is human erythropoietin, a glycoprotein that controls red blood cell production in bone marrow.
BACKGROUND. Epogen has been approved for treating anemia caused by kidney failure or chemotherapy, and after certain types of surgery in order to decrease the need for blood transfusions. Epogen has also been used to treat orthostatic hypotension, a condition in which blood pressure drops upon standing, causing light-headedness, dizziness or fainting.
USES IN CFS/ME. Dr. Hugh Calkins, a cardiologist at Johns Hopkins, has observed that CFS/ME is closely associated with neurally-mediated hypotension (NMH). He found that 90% of CFS/ME patients have some form of NMH. This observation was independently confirmed by Dr. David Streeten who discovered that among two groups of patients with orthostatic intolerance (OI), one had an abnormally low volume of red blood cells, and another had low plasma circulation. As it turned out, both of these were people with CFS/ME. Dr. Streeten treated these patients using protocols and medications for OI, including Florinef, beta-blockers and epogen to raise standing blood pressure. It wasn't until he was contacted by Dr. Bell, whose CFS/ME patients were exhibiting the same symptoms, that Dr. Streeten realized he had successfully treated a group of CFS/ME patients. Since that time, most doctors in the CFS/ME community have incorporated NMH treatments into their protocols.
In an important study conducted at the University of Miami, Hurwitz et al observed that 60-70% of CFS/ME patients show below normal red blood cell volume. The authors concluded that “the findings indicate that lower cardiac volume levels, displayed primarily by subjects with severe CFS, were not linked to diminished cardiac contractility levels, but were probably a consequence of a co-morbid hypovolaemic condition.” This study was significant because it proved that diminished blood volume was pervasive among CFS/ME patients. Unfortunately, while Procrit increased red blood cell volume, fatigue and exercise intolerance did not improve in the treated group.
PROTOCOL. Very few CFS/ME doctors use Procrit. Dr. Shoemaker treats his patients with 8,000 units of Procrit twice a week for five doses and then decreases the dosage to 4,000 to 6,000 every three to five days. This rather intensive protocol has not gone without criticism from doctors who point out that the “off label” use of Procrit for non-anemic patients is risky.
PROS AND CONS. Procrit is by no means a proven treatment for the correction of low blood volume in CFS/ME. In fact, even weeks after correcting low red blood cell volume in CFS/ME patients, Hurwitz et al noted that there was no corresponding reduction in symptoms. Procrit includes a boxed warning that “ESAs [Erythropoiesis-Stimulating Agents ] increase the risk of death, myocardial infarction, stroke and thrombosis.” Needless to say, CFS/ME patients should give careful thought to the possible risks before embarking on a protocol that includes Procrit.
FURTHER READING
Safety update from the makers of Procrit: http://www.procrit.com/
CFS/ME Forum review of treatments for NMH in CFS/ME: http://www.ncf-net.org/forum/orthostatic98.htm
Fall 2002 CFIDS Chronicle Q&A with Dr. Hurwitz about Procrit. http://www.cfids.org/archives/2002/2002-4-article01.asp
RESEARCH
Hurwitz, Barry E., Virginia T. Coryell, Meela Parker, Pedro Martin, Arthur LaPerriere, Nancy G. Klimas, George N. Sfakianakis and Martin S. Bilsker. “Chronic fatigue syndrome: illness severity, sedentary lifestyle, blood volume and evidence of diminished cardiac function.” Clinical Science (2010) 118, (125–135) (Printed in Great Britain) http://www.clinsci.org/cs/118/cs1180125.htm
FLEXERIL
DESCRIPTION. Flexeril (cyclobenzaprine) is a muscle relaxant used to treat pain and skeletal muscle spasms.
BACKGROUND. Flexeril is closely related to tricyclic antidepressants such as Elavil and Tofranil. The drug works by blocking nervous system impulses from the spinal cord to skeletal muscle. Researchers are not entirely sure how Flexeril specifically blocks pain impulses. Some claim that the drug's tricyclic properties (blocking the uptake of serotonin and norepinephrine) exert direct analgesic effects. Other studies seem to indicate that the inhibition of serotonergic pathways alone are responsible for a decreased firing of motor neurons.
USES IN CFS/ME. Flexeril is a commonly prescribed medication that can be extremely beneficial in treating the fibromyalgia component of CFS/ME. Because it is sedating, it is also used to treat insomnia.
PROTOCOL. For muscle pain, 10 mg one to three times a day is recommended. To treat insomnia, Dr. Teitelbaum recommends 10 mg at bedtime. Patients who are sensitive to medications may wish to start with 5 mg or lower.
PROS AND CONS. Flexeril is an older drug with a good safety record and minimal side effects. The most common side effects are excess sedation the next day (a “sleep hangover”) and dry mouth. Both CFS/ME and fibromyalgia patients report that Flexeril is most useful for episodes of muscle spasms or back pain. Most patients who are intolerant to other sleep medications report that it relieves insomnia. Flexeril is not addictive, but, as is the case with many sleeping pills, it tends to lose its effectiveness over time. Because of its anticholinergic effects, Flexeril is contraindicated in patients who have taken an MAOI within 14 days, have a history of heart arrhythmias, or are taking other anticholinergic drugs (such as antihistamines).
AVAILABILITY AND COST. Flexeril is available by prescription, in generic or brand-name formulations. The drug is inexpensive. A one-month supply of the generic costs as little as $7 and is covered by most insurance policies.
SEE: Pain, Sleep Disorders
PATIENT REVIEWS
CFS/ME patient reviews of Flexeril: http://www.revolutionhealth.com/drugs-treatments/rating/flexeril-for-chronic-fatigue-syndrome-cfs-cfids-me
FLORINEF
DESCRIPTION. Florinef (fludrocortisone) is a synthetic corticosteroid.
BACKGROUND. Florinef is primarily used to treat patients with Addison's disease, a condition in which the adrenal glands do not produce sufficient adrenal steroids. Florinef is also a first-line treatment for orthostatic intolerance; it helps the body retain salt which otherwise would be passed in the urine. Because it has mineralocorticoid activity, its effects are limited to regulation of electrolyte and water balance. Like other corticosteroids, Florinef will raise blood sugar levels.
USES IN CFS/ME. Florinef received considerable attention as a CFS/ME medication as the direct result of a highly publicized Johns Hopkins study of neurally mediated hypotension (NMH). In NMH, sudden decreases in blood pressure leads to fainting (syncope), light-headedness, trouble concentrating, and dizziness. As nearly all of the CFS/ME patients in the Johns Hopkins study tested positive for NMH, researchers have been hopeful about treatments that would address this particular symptom. Florinef, because of its ability to increase sodium retention, helps to raise blood pressure. In so doing, many symptoms associated with decreased blood pressure can be relieved.
PROTOCOL. Most physicians currently working with CFS/ME patients recommend starting at a low dose to avert any possible drug reactions. Prior to taking Florinef, Dr. Rowe recommends increasing salt and fluid intake, then beginning with ¼ tablet. He increases the dose by ¼ tablet every 4 to 7 days until a final dose of one tablet (0.1 mg) is reached. If there are no significant side effects, he recommends increasing to a maximum of 1½-2 tablets a day. Dr. Bell has observed that Florinef seems to work best on younger patients. One patient noted that Florinef must be taken exactly every 24 hours or symptoms return; thus a rigid schedule is advised once the medication is started.
Because Florinef causes the body to excrete more than the usual amount of potassium, a potassium supplement is advised. In addition, plenty of fluids should be consumed while taking this medication. The side effects of headache or stomach ache can be lessened when Florinef is taken with a full glass of water. The small amount of lactose in Florinef may cause some discomfort to those who are lactose intolerant or allergic to milk protein.
PROS AND CONS. Although Florinef has been highly touted as an overall CFS/ME treatment, CFS/ME specialists have pointed out that the success rate is not high with this drug. Two randomized control studies conducted in 1998 and 2000 failed to show any improvement in a group of adult CFS/ME patients. In 2001 Rowe et al found that mono-treatment with Florinef fared no better than placebo in a group of 100 CFS/ME patients. Dr. Myhill has listed Florinef as one of the treatments “not worth trying.” She noted that Florinef produced nothing but swollen ankles in her patients.
Florinef can produce serious side effects, the most common of which are high blood pressure and depression. Florinef can also deplete the body of electrolytes (potassium, calcium and magnesium). Common side effects include difficulty sleeping, light-headedness, headache, appetite changes, nausea, increased sweating, and nervousness. Because of these side effects, some doctors recommend starting with licorice, which can mimic the action of steroids, but is a more gentle treatment.
Before embarking on a course of treatment with Florinef or its substitutes, patients are advised to undergo thorough testing to confirm NMH. Because these drugs affect blood pressure, treatment must be closely supervised by a physician.
AVAILABILITY AND COST. Florinef is available by prescription. A 30-day supply of 0.1 mg tablets costs about $14.
SEE: Cardiac and Cardiovascular Symptoms; Herbs (licorice).
FURTHER READING
Cort Johnson's excellent review of Florinef. http://aboutmecfs.org.violet.arvixe.com/Trt/TrtFlorinef.aspx
The Outs and Ins of OI. Excellent article by Kimberly McCleary on OI in CFS/ME. Includes treatments: http://www.research1st.com/2011/06/19/the-outs-and-ins-of-oi/
PATIENT REVIEWS
Review of Florinef by an Australian with CFS/ME who has tried (and reviewed) many treatments. http://livingwithchronicfatiguesyndrome.wordpress.com/2010/07/27/fludrocortisone-for-cfs/
CFS/ME patient reviews of Florinef: http://www.revolutionhealth.com/drugs-treatments/rating/fludrocortisone-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Peterson PK, Pheley A, Schroeppel J, Schenck C, Marshall P, Kind A, Haugland JM, Lambrecht LJ, Swan S and Goldsmith S. “A preliminary placebo-controlled crossover trial of fludrocortisone for chronic fatigue syndrome.” Arch Intern Med. 1998 Apr 27;158(8):908-14. http://www.ncbi.nlm.nih.gov/pubmed/9570178 (Abstract)
Rowe PC, Calkins H, DeBusk K, McKenzie R, Anand R, Sharma G, Cuccherini BA, Soto N, Hohman P,Snader S, Lucas KE, Wolff M, Straus SE. “Fludrocortisone acetate to treat neurally mediated hypotension in chronic fatigue syndrome: a randomized controlled trial.” JAMA. 2001 Jan 3;285(1):52-9. http://www.ncbi.nlm.nih.gov/pubmed/11150109 (Abstract)
GAMMA GLOBULIN
DESCRIPTION. Gamma globulin is a class of blood plasma proteins that contain antibodies.
BACKGROUND. Gamma globulin, or immunoglobulin, is a blood product pooled from many donors and processed so that it contains a high concentration of immunoglobulin G (IgG) and other antibodies that mitigate against and prevent certain diseases. Gamma globulin has been in use for more than 40 years to prevent hepatitis, particularly in health care workers, as a prophylactic during epidemics of measles and rubella, as an immune modulator in Kawasaki syndrome and in myasthenia gravis (a disease that affects the muscles).
USES IN CFS/ME. Although it has fallen out of favor in recent years, gamma globulin was one of the earliest CFS/ME treatments. The rationale behind the use of gamma globulin is twofold. First, it was reasoned that if CFS/ME were caused by a virus, particularly a common virus that most of the general public had been exposed to (such as Epstein-Barr virus), gamma globulin would contain certain antibodies to fight the virus.
Second, certain patients with CFS/ME had demonstrated deficiency of IgG subclasses and it was proposed that gamma globulin could correct this deficiency. While gamma globulin has sometimes been helpful in treating CFS/ME, it is not easy to determine why. It seems that patients who demonstrate IgG deficiency do not always respond better to gamma globulin therapy than do those without IgG deficiency. Several studies, both controlled and open, have been completed in the United States and other countries with inconclusive results.
In 1986 Dr. James Oleske and colleagues from the New Jersey School of Medicine in Newark conducted an open trial of 12 patients with chronic Epstein-Barr virus infection (CFS/ME) with IgG or IgG subclass deficiency. These patients underwent intravenous gamma globulin therapy for one year. Symptoms improved in eight and showed no improvement in four, but did not worsen in any patients.
Also in 1986, Dr. Richard DuBois of Atlanta, Georgia, reported the results of a double-blind controlled study of patients with chronic mononucleosis syndrome (CFS/ME) treated with intramuscular gamma globulin. Symptoms in 52% of the patients who received gamma globulin improved after treatment.
In 1988 Dr. Phillip Peterson of the University of Minnesota headed a double-blind controlled trial of intravenous gamma globulin in 30 patients with CFS/ME. Patients received an infusion of gamma globulin every month for 6 months. Of these 30 patients, 12 (40%) had low IgG concentrations and 29 (9%) had a viral onset. Given the immunological deficiencies, a presumed viral component, and a severely affected group of patients, the results fell short of expectations. No significant difference was demonstrated between the placebo and drug responses.
In 1991 Dr. Denis Wakefield of Sydney, Australia, concluded a study of 49 patients with CFS/ME enrolled in a double-blind placebo-controlled study of intravenous gamma globulin. Twenty-three patients received gamma globulin infusions over 90 days, with encouraging results. Symptoms in 10 patients improved. In addition, several immune parameters tested showed improvement after treatment. Some side effects were reported, but they may have been due to the high dose of gamma globulin. Dr. Wakefield and his colleagues reported interest in undertaking a larger trial with a lower dose of gamma globulin.
In 1997 Australian pediatrician Dr. K.S. Rowe published the results of a study of 70 adolescents (ages 12 to 18 years) with chronic fatigue syndrome who received intravenous gamma globulin therapy. After three months of treatment, significant improvement was noted, but there were some side effects.
In 2001 Dr. Rowe's long-term study of pediatric patients who were followed for seven years also showed that patients experienced significant improvement. Unfortunately, there has been little research after 2001 into the potential benefits gamma globulin.
PROTOCOL. Intravenous gamma globulin may be infused once a month for six months or longer. Intramuscular (IM) gamma globulin can be injected once or twice a week for six weeks, after which the patient is reassessed. Dr. Paul Cheney has noted that IM gamma globulin is not as effective as intravenous administration (CFIDS Chronicle, Spring 1995).
PROS. Many leading clinicians continue to use gamma globulin therapy, with varying degrees of success. Gamma globulin is not usually a first-line treatment and is often used after other therapies have been attempted. Dr. Cheney has found gamma globulin particularly useful in helping reduce the frequency of upper respiratory tract infections in some patients. Dr. Murray Susser and Dr. Michael Rosenbaum, authors of Solving the Puzzle of Chronic Fatigue Syndrome, state that, although CFS/ME requires an integrative approach, if they had to choose the single most effective treatment, it would be gamma globulin. A number of more severely ill patients note improvement of almost all symptoms – notably, cognition, energy, and mood.
CONS. A significant number of patients note little or no benefit. Side effects include headaches, dizziness, and nausea, particularly if the dose is high or the rate of infusion is too fast. A number of patients with CFS/ME have expressed concern about the safety of gamma globulin, inasmuch as it is a blood product. Most physicians believe it is safe because, to date, there is no record of anyone contracting human immunodeficiency virus (HIV) from gamma globulin therapy. However, in early 1994 there were reports in newspapers concerning batches of gamma globulin overseas that were contaminated with hepatitis C virus.
In May 1994 a new manufacturing process for intravenous gamma globulin was developed that inactivates any viral contaminants. Gamma globulin therapy is now considered safe. Nevertheless, it is important to carefully discuss the risks and benefits with a physician.
AVAILABILITY AND COST. Gamma globulin is obtained through a physician and is usually administered in the office. Intravenous infusions are costly and can run as much as $3000 a month. Some insurance companies reimburse the cost if the claim carefully documents specific immune dysfunction such as IgG subclass deficiency or hypogammaglobulinemia. Intramuscular gamma globulin is much less costly, generally around $50 a vial.
RESEARCH
Rowe KS. “Double-blind randomized controlled trial to assess the efficacy of intravenous gammaglobulin for the management of chronic fatigue syndrome in adolescents.” J Psychiatr Res. 1997 Jan-Feb;31(1):133-47. http://www.ncbi.nlm.nih.gov/pubmed/9201655 (Abstract)
Rowe, Katherine S. MBBS, MD, MPH, Dip Ed (Lond), FRACP. “Five-Year Follow-Up of Young People with Chronic Fatigue Syndrome Following the Double Blind Randomised Controlled Intravenous Gammaglobulin Trial.” Journal of Chronic Fatigue Syndrome (The Haworth Medical Press, an imprint of The Haworth Press, Inc.) Vol. 5, No. 3/4, 1999. http://www.co-cure.org/infores6.htm
GcMAF
DESCRIPTION. GcMAF is a naturally occurring substance in the human body which destroys pathogens by activating macrophages. The acronym stands for Gc (a vitamin D binding protein) Macrophage Activating Factor.
BACKGROUND. In the early 1990s, Dr. Nobuto Yamamoto, director of the Division of Molecular Immunology and Immunotherapy at the Socrates Institute for Therapeutic Immunology in Philadelphia, Pennsylvania, discovered a substance that inhibited tumor production in mice. Throughout the 1990s Dr. Yamamoto continued his research, expanding it to cases of cancer in humans. But it wasn't until 2008 that Dr. Yamamoto published his groundbreaking study on breast cancer. In this study, weekly injections of GcMAF were given to 16 breast cancer patients. Within three months the tumors were eradicated, with no recurrence over the next four years.
Subsequent studies with GcMAF used for colorectal and prostate cancer yielded similar results. In all cases the tumors disappeared with no recurrence. The rationale behind the success of GcMAF is that when the naturally occurring Gc protein is destroyed by cancer cells (more specifically by an enzyme called nagalase) it hamstrings the immune system's ability to make sufficient tumor-destroying macrophages. The result is an immunosuppressed state which allows the cancer to spread. Injecting GcMAF into cancer patients restores the compromised immune system, which then successfully combats the cancer.
The implications for other immune compromised patients are enormous. In 2009 Dr. Yamamoto published a study demonstrating that after fewer than 18 weekly administrations of GcMAF, HIV infection was also completely eradicated. According to the study, "no recurrence occurred and their healthy CD + cell counts were maintained for 7 years."
USES IN CFS/ME. Given the spectacular results of the Yamamoto studies one would have expected to have seen front-page spreads in the New York Times. However, apart from Reuters, the news agencies barely took notice. As of today, no clinics in the U.S. are using GcMAF as a treatment for cancer. Several prominent CFS/ME physicians, however, have begun using GcMAF for patients who test high in nagalase.
Dr. Kenny De Meirleir treated 108 of his CFS/ME patients with weekly administration of GcMAF. This group of patients showed high amounts of nagalase, which Dr. De Meirleir notes can be produced by intestinal bacterial infections as well as herpes and retroviral infections. (Dr. Chia also points out that nagalase can be elevated as a result of enteroviral infections, which produce small intestinal bacterial overgrowth (SIBO) leading to subsequent immune system dysregulation.) After an average of 15 weeks of treatment, 68 of the 108 patients reported significant improvement in fatigue, sleep, pain, cognitive impairment, orthostatic intolerance, and digestive disturbances. (See below for a link to Dr. De Meirleir's presentation.)
Because GcMAF causes an increase in immune system activation, Dr. De Meirleir recommends starting with a very low dose of GcMAF. Some CFS/ME patients have undiagnosed infections which could lead to Immune Reconstitution Inflammatory Syndrome (IRIS). Once the immune system is stimulated, symptoms due to co-infections can worsen. Of Dr. De Meirleir's 108-patient cohort, 20-30% of them experienced IRIS.
Dr. Cheney has also begun to treat patients with GcMAF, as well as with a natural yogurt probiotic MAF (MAF 314) developed by Professors Ruggiero and Pacini in Italy. GcMAF demonstrated a response rate of 79% (15 out of 19 patients), which is similar to Dr. De Meirleir's results. The oral MAF 314 demonstrated a response rate of 76% over a period of only 28 days.
PROTOCOL: There are several protocols currently in use. Most CFS physicians begin with 0.20 - 0.25 ml via injection (IM) weekly. Dr. Cheney starts his severely ill patients at a much lower dose administered sublingually, then gradually increases the dose. Typically, the full course of treatment is 8-20 weeks. In order to be effective, GcMAF requires adequate levels of vitamin D. Patients should be tested for vitamin D levels prior to beginning treatment. (Optimal ranges fall between 42 and 60). Patients should also be tested for nagalase levels before treatment and on a monthly basis after beginning GcMAF.
Physicians may recommend concurrent antiviral treatment with Nexavir if the viral load is high. Artesunate may also be prescribed, as well as adjunctive supplementation with B vitamins.
Anti-inflammatory drugs, such as corticosteroids (prednisolone, prednisone, etc.) and NSAIDs (ibuprofen, aspirin, etc.) should be avoided while taking GcMAF as these will interfere with the treatment. Morphine analogs (oxycodone, tramadol, etc.), beta blockers, and cytotoxic medications (Sendoxan, Vepesid, Taxol, etc.) should be avoided. Aspartame and carrageenan, two food additives, can also block GcMAF.
GcMAF is contraidicated for patients with MS.
PROS AND CONS. GcMAF is an experimental drug, which means not much is known about its effects on the CFS/ME population other than the few studies performed by Drs. De MeirLeir and Cheney. As with other medications, patients report a wide range of responses, from feeling significantly worse to an almost miraculous recovery of strength and energy. Frequently, a patient will notice improvement over the first six weeks, and then experience a decline. This may be due to exhaustion of vitamin D reserves. For this reason, continuing supplementation with vitamin D may be advised.
AVAILABILITY AND COST. Drs. Cheney, Enlander and De Meirleir are currently using GcMAF with their CFS/ME patients. The price for 2.2 ml of GcMAF (about 8 doses at .25 per dose) is roughly $1000 ($800 euros). Because of the risk of IRIS, it is not recommended that CFS/ME patients take GcMAF without the supervision of a knowledgeable physician. MAF 314 can be obtained from Dr. Cheney's clinic for $3500. Dr. Enlander is currently developing a less expensive form of probiotic MAF (MAF 378) in New York. The test for nagalase levels can be ordered by physicians from Health Diagnostics. It costs $65. GcMAF must be refrigerated
TESTING
Health Diagnostics and Research Institute (formerly Vitamin Diagnostics, Inc.)
South Amboy Medical Center
540 Bordentown Ave., Suite 2300
South Amboy, New Jersey 08879
Telephone: (732) 721-1234
Fax: (732) 525-3288
Testing for nagalase.
SUPPLIERS
GcMAF
Clos de Balade 21
1140 Evere
Brussels
Belgium
Website: http://www.gcmaf.eu/info/
BGLI Bio Group Laboratories
Tel: 31-3576-00-176 (GMT+2) (Netherlands)
Website: http://www.bgli.nl/ (There is a contact form on the site)
FURTHER READING
Dr. Kenny De Meirleir's talk on GcMAF and its use in treating CFS/ME: http://cfspatientadvocate.blogspot.com/2011/11/mt-sinai-mecfs-conference-de-meirleir.html
Dr. Cheney's GcMAF studies: http://www.cheneyclinic.com/gcmaf-studies-presented-at-iacfsme-meetings-in-ottawa/833
Excellent information on GcMAF, including where to find clinics in Europe that use GcMAF, patient forums, and purchasing information: http://www.gcmaf.eu/info/
European lab that offers testing for nagalase: http://www.europeanlaboratory.nl/
Phoenix Rising forum threads on GcMAF discussing Kenny De Meirleir's use of GcMAF, where to purchase, and how to obtain testing for nagalase: http://forums.phoenixrising.me/showthread.php?6019-GcMAF-for-XMRV-Gc-protein-derived-macrophage-activating-factor-anyone-taking-it/page116
and
http://forums.phoenixrising.me/showthread.php?6019-GcMAF-for-XMRV-Gc-protein-derived-macrophage-activating-factor-anyone-taking-it/page117
Patient thread on MAF 314: http://phoenixrising.me/forums/showthread.php?14838-MAF-314
"Who Responds to GcMAF." Very technical discussion of gene types http://www.cfscentral.com/2011/01/who-responds-to-drug-gcmaf.html
Good article about cancer and GcMAF by Bill Sardi http://www.thenhf.com/article.php?id=633
Another good follow-up article by Bill Sardi: http://www.thenhf.com/article.php?id=771
Cancer and GcMAF: http://www.center4cancer.com/glyco-protein.php
Professor Ruggiero's website on GcMAF and MAF 314 http://www.marcoruggiero.org/pdf/Oct%2022.pdf
“Compassionate Use Treatment of CFS with GHP (GcMAF)” Dr. Paul Cheney, Sept. 2011. http://www.gcmaf.nl/documents/research/Compassionate%20use%20Treatment%20of%20CFS%20with%20GHP%20(%20GcMAF%20).pdf
Dr. Cheney's pilot study of GcMAF.
PATIENT EXPERIENCES
A Cheney patient blog about her experience with GcMAF. This blog is very detailed, with information about dosage, testing and patient responses. http://nopostergirl.com/2011/04/16/the-post-appointment-post/
Cheney patient blog on GcMAF http://blogwormwood.blogspot.com/2011/05/gcmaf.html
RESEARCH
Yamamoto N, Suyama H, Yamamoto N, Ushijima N. “Immunotherapy of metastatic breast cancer patients with vitamin D-binding protein-derived macrophage activating factor (GcMAF).” Int J Cancer. 2008 Jan 15;122(2):461-7. http://www.ncbi.nlm.nih.gov/pubmed/17935130 (Abstract)
Yamamoto N, Suyama H, Koga Y. “Immunotherapy of metastatic colorectal cancer with vitamin D-binding protein-derived macrophage-activating factor, GcMAF.” Cancer Immunol Immunother. 2008 Jul;57(7):1007-16. http://www.ncbi.nlm.nih.gov/pubmed/18058096 (Abstract)
Yamamoto N, Suyama H, Yamamoto N, “Immunotherapy for Prostate Cancer with Gc Protein-Derived Macrophage-Activating Factor, GcMAF.” Transl Oncol. 2008 Jul;1(2):65-72. http://www.ncbi.nlm.nih.gov/pubmed/18633461 (Abstract)
Yamamoto N, Ushijima N, Koga Y. “Immunotherapy of HIV-infected patients with Gc protein-derived macrophage activating factor (GcMAF).” J Med Virol. 2009 Jan;81(1):16-26. http://www.ncbi.nlm.nih.gov/pubmed/19031451 (Abstract)
GUAIFENESIN
DESCRIPTION. Guaifenesin is an expectorant that helps clear mucus from congested passageways by increasing production of respiratory tract fluids. It is the primary active ingredient in many cough syrups.
USES IN CFS/ME. Dr. Paul St. Armand, an endocrinologist at the University of California at Los Angeles, first began working with patients with fibromyalgia in the 1960s. From his observations, Dr. St. Armand speculated that patients with fibromyalgia and CFS/ME might have an inherited metabolic defect that causes faulty excretion of phosphates. According to Dr. St. Armand, if phosphate accumulates in the mitochondria of cells, then the production of adenosine triphosphate (ATP) is impaired, leading to a loss of cellular energy. The accumulation of phosphates also leads to increased calcium within the cells, possibly creating the tender points so commonly seen in fibromyalgia. It appeared to Dr. St. Armand that this defect in phosphate excretion could account for the symptoms of fibromyalgia and CFS/ME.
In support of his theory, Dr. St. Armand observed that gout medications, which increase excretion of both uric acid and phosphate, produced positive results in FM patients, although they did have serious side effects if used long term. To Dr. St. Armand's delight another medication, guaifenesin, produced the same results, without the side effects.
PROTOCOL. For people with CFS/ME, guaifenesin LA (long acting) is usually prescribed. It can be purchased in pill form, without added antihistamines or decongestants. Dr. St. Armand recommends an initial dosage of 300 mg of pure guaifenesin twice a day. If that proves ineffective, the dosage is increased to 600 mg twice a day. About 30% of his patients may require higher doses. Dr. St. Armand claims that two months of treatment reverses a year of illness, which should provide a baseline for calculating how long the medication may be needed – for example, a person who has been ill for four years will need eight months of treatment.
Dr. St. Armand cautions that for guaifenesin to be effective, salicylate must not be used (salicylate or salicylic acid ingredients are in Pepto-Bismol, Ben-Gay, Myoflex Creme, aspirin, Alka-Seltzer, cosmetics, plant-containing shampoos and conditioners, plant-derived vitamins, and herbal remedies). Dr. St. Armand also recommends that patients take a calcium and magnesium supplement with meals to block absorption of phosphates in food.
PROS. No controlled studies have been performed to confirm or disprove the effectiveness of guaifenesin in treating symptoms of CFS/ME, so commentaries on this drug are anecdotal. One patient with long-term CFS/ME reported dramatic symptomatic improvement with guaifenesin (Mass CFS/ME Update, Summer 1996). She began taking guaifenesin in 1994 to treat a stubborn bout of bronchitis and was surprised to note a number of other symptoms began improving. After several months she noticed she was beginning to have clusters of "good days" and that her pain was "almost nonexistent." She also noted improvements in cognitive function, energy, and vision.
CONS. Although few side effects are directly attributable to guaifenesin, most CFS/ME patients report that their symptoms initially worsen while their systems are being “cleaned out.” Often a patient may feel much worse for the first two to four months of treatment (some even longer), the most common side effect being severe pain. Dr. St. Armand warns that this treatment "takes confidence and strength" because results may not be seen for several months. He also warns that patients with both fibromyalgia and hypoglycemia will not notice any improvement with guaifenesin treatment unless the hypoglycemia is corrected (see Hypoglycemia for dietary and other recommendations). Although Dr. St. Armand believes the long-term benefits are worthwhile for patients with fibromyalgia, many patients with CFS/ME may be justifiably wary of risking relapse.
Patients interested in trying guaifenesin should also note that although Dr. St. Armand claims significant improvement among his patients, studies have not replicated his results. A double-blind controlled study conducted at the Oregon Health Sciences University by Dr. Robert M. Bennett and Dr. Sharon Clark found no difference between the guaifenesin and placebo groups after a year of treatment. Neither did they find an increase in urinary excretion of phosphates, which seems to undercut the basis for guaifenesin's theoretical mode of action. In addition, muscle studies by Muhammad Yunus, M.D., of University of Illinois College of Medicine, and Dr. Robert Simms have shown that calcium phosphate deposits have never been a problem in fibromyalgia. Currently, none of the major CFS/ME clinics or doctors include guaifenesin in their protocols.
AVAILABILITY AND COST. Guaifenesin is available through online distributors. ProHealth sells a 100-pill bottle of fast-acting guaifenesin (400 mg) for $15.79. The long-acting variety costs about $50.00 a bottle.
BOOKS AND ARTICLES
St. Armand, Paul and Claudia Craig Marek. What Your Doctor May Not Tell You About Fibromyalgia: The Revolutionary Treatment That Can Reverse the Disease. Wellness Central. 2006.
St. Armand, R. Paul M.D. “Chronic Fatigue and Fibromyalgia: One Disease, Two Names.” 1999. http://www.fibromyalgiatreatment.com/Research_TwoNames.htm
FURTHER INFORMATION
Guaifenesin protocol. Includes a list of doctors and practitioners http://fibromyalgiatreatment.com/
The Fibromyalgia Network's consumer alert on guaifenesin http://www.fmnetnews.com/resources-alert-product6.php
Guaifenesin support group. Last updated in 2007: http://www.psha-inc.com/guai-support/sf/FAQ-GuaiProductTroubleshooter.htm
PATIENT REVIEWS
CFS/ME patient reviews of guaifenesin: http://www.revolutionhealth.com/drugs-treatments/rating/mucinex-for-chronic-fatigue-syndrome-cfs-cfids-me?page=2&view=treatment
H2 BLOCKERS - TAGAMET AND ZANTAC
DESCRIPTION. Tagamet (cimetidine) and Zantac (ranitidine) are histamine H2 receptor antagonists that inhibit acid secretion in the stomach.
BACKGROUND. Before the Food and Drug Administration (FDA) approval of Tagamet in 1977, the pain resulting from duodenal ulcers was nearly impossible to treat with standard medications. While not a cure, Tagamet is thought to allow ulcers to heal by blocking acid secreted by the stomach in response to histamine. Millions of patients now take Tagamet and Zantac (approved in 1983) and a substantial number have obtained significant relief from pain. Tagamet, Zantac, and two other approved H2 blockers, Axid (nizatidine) and Pepcid (famotidine), are also prescribed to treat heartburn and gastritis.
In the early 1980s, Dr. Jay Goldstein used Tagamet to treat infectious mononucleosis (confirmed by monospot test, enlarged spleen, and other clinical findings consistent with the diagnosis) in a college student. The symptoms resolved within 24 hours. Dr. Goldstein's rationale for treatment was based on the fact that Epstein-Barr virus, which causes mononucleosis, is a herpesvirus and, in most herpes infections, there is an increased number of T suppressor cells. It had been recently demonstrated that T suppressor cells had H2 receptors on their surfaces, and it was thought that the cells were activated by histamine. Dr. Goldstein theorized that perhaps the T suppressor cells could be inactivated by Tagamet, an H2 blocker. His theory appears to have validity, as Dr. Goldstein reported positive results in 90% of cases of mononucleosis treated with Tagamet. He has received positive feedback from physicians around the United States who have replicated his results (CFIDS Chronicle, 1988 Compendium).
In 1990 Ashir Kumar, a researcher at Michigan State University, supported Dr. Goldstein's findings with his own research. In several studies, he found that cimetidine (Tagamet) enhanced immune function. “Patients who received cimetidine were shown to exhibit enhanced cell-mediated immunity as evaluated by increased response to skin-test antigens, restoration of sensitivity following development of acquired tolerance, and increased responses of lymphocytes to mitogen stimulation. Patients also demonstrated that patients with herpes zoster and herpes simplex who were given cimetidine may have benefited therapeutically from the drug.”
In an interesting corollary to its other uses, some urologists prescribe H2 blockers for interstitial cystitis when other medications are not tolerated.
USES IN CFS/ME. In 1985 Dr. Goldstein began to see his first cases of what was then called chronic Epstein-Barr virus infection (now CFS/ME). Using the same logic that he used to treat mononucleosis, Dr. Goldstein gave his patients Tagamet and Zantac. He found over the course of years that at least 20% of patients with CFS/ME responded favorably to treatment with H2 blockers. Although the cause of CFS/ME remains undetermined, it is known that in CFS/ME there is activation of T suppressor cells, probably due to viral activity. It is believed that H2 blockers have a modulatory effect on the immune system in that they probably inhibit overproduction of lymphokines responsible for some of the flu-like symptoms of CFS/ME.
Several leading CFS/ME clinicians, including Dr. Charles Lapp, use H2 blockers to treat gastrointestinal symptoms as well as for immune system modulation. Dr. Murray Susser and Dr. Michael Rosenbaum used H2 blockers to treat immune system dysfunction.
PROTOCOL. Most patients take only low doses of these H2 blockers (even a sliver of a pill can be effective, according to Dr. Goldstein). Others are able to tolerate the standard prescribed dose for ulcers: Tagamet 300 to 400 mg, one or more tablets per day; Zantac 75 to 300 mg/day.
PROS. H2 blockers work rapidly, and results can often be seen in less than two weeks, thereby making a trial worthwhile. Many patients have reported a variety of benefits. CFS/ME patients with allergies feel much better overall after taking Zantac. Some have found significant relief from digestive disturbances. Not surprisingly, given the effects that H2 blockers have on the immune system, people with CFS/ME also report that Tagamet gives them more energy and lessens the weak, achy feeling of CFS/ME.
CONS. Dr. Goldstein has noted that some patients feel nervous and agitated while taking Tagamet. Other clinicians believe H2 blockers cause depression (a less common side effect according to the Physicians’ Desk Reference). Because Tagamet may interact with and increase blood concentrations of many drugs, some of which are commonly prescribed in CFS/ME (e.g., antidepressants and benzodiazepines), it is important to advise your physician of all medications you are taking. Zantac may be prescribed more frequently than Tagamet to treat symptoms of CFS/ME, because it interacts with fewer medications and may pose less risk for side effects. Both Tagamet and Zantac will either aggravate pre-existing hypochloridia, or cause it. High levels of Zantac are known to cause an unusual condition in men which produces breast enlargement (gynecomastia).
AVAILABILITY AND COST. Tagamet and Zantac are available by prescription and over the counter at any pharmacy. Over-the-counter Tagamet HB 200 and Zantac 75 mg are available for between $10 and $15.
FURTHER READING
Kumar A. “Cimetidine: an immunomodulator.” Department of Pediatrics and Human Development, Michigan State University, East Lansing 48824. DICP 1990 Mar;24(3):289-95. http://www.ncbi.nlm.nih.gov/pubmed/2138376 (Abstract)
Overview of immunological effects of H2 blockers. http://www.lef.org/magazine/mag2001/mar2001_report_tagamet_1.html
Thread discussing histamine blockers in CFS/ME patients, including Zantac and Tagamet. http://forums.phoenixrising.me/showthread.php?2077-Tagamet-(cimetidine)-for-CFS/ME-(worked-for-me)/page2
Article discussing gynecomastia after excess Tagamet. http://gerd.emedtv.com/cimetidine/cimetidine-and-gynecomastia.html
HORMONES
Growth Hormone, Testosterone, Thyroid Hormones
Hormones are chemical messengers that are released from glands in the endocrine system. Because hormones can be released directly into the bloodstream, they affect nearly every function in the body. Hormones are responsible for stimulating growth, regulating the immune system, initiating “fight or flight” responses, sexual maturation and reproduction, hunger, thirst, mood swings, metabolic regulation, and maintaining homeostasis. A deficiency or dysregulation of hormone production will produce profound effects on the body.
Endocrine system disturbances are common, if not universal, among CFS/ME patients. As a consequence, hormone production is also affected. Unfortunately, hormones are usually released in spurts, and their effects, while widespread, are not constant. This makes hormone regulation through medical intervention problematic. A steady dose of hormones may, in fact, worsen symptoms. That being said, patients who consistently test low in certain hormones may benefit greatly from supplementation with bio-identical or synthetic hormones. Because of their widespread effects on the body, hormone treatments should always be monitored by a physician.
FURTHER READING
“Endocrine Causes of Chronic Fatigue: A Review of Symptoms, Treatments.” CFIDS Chronicle, Spring 2003. http://www.cfids.org/archives/2003/2003-2-article02.asp
This is a good summary of various endocrine disturbances that can cause fatigue.
GROWTH HORMONE
DESCRIPTION. Growth Hormone (GH) is a peptide hormone produced in the pituitary gland.
BACKGROUND. Growth Hormone is primarily responsible for increasing height in children, although it has a number of other functions as well, including increasing protein synthesis, stimulating the growth of internal organs, maintaining pancreatic islets, and stimulating the immune system. Medically, it is prescribed for children with growth failure stemming from GH deficiency.
In rare cases, adults will develop GH deficiency. Usually, this is caused by structural problems in the pituitary gland (tumors), although unexplained disruptions in hormone production can also occur. When a physician suspects GH deficiency, he or she will test for the presence of IGF-1 in the body to determine if GH levels are low. (GH secretion leads to IGF-1 production.) As most GH is secreted during deep sleep, patients may be kept overnight to measure GH levels.
Because GH builds muscle mass, strengthens bones and increases energy, it has become a popular, if dubious, supplement for athletes, who use it to improve performance. Too much GH can result in acromegaly, or gigantism. Due to its reputed anti-aging effects, GH has also been promoted as a “fountain of youth,” which has no doubt spurred the increase of off-shore manufacturers.
USES IN CFS/ME. Disturbances in the HPA (hypothalamus-pituitary-adrenal) axis have been well-documented in CFS/ME patients. One of the earliest studies to show that GH is affected by HPA axis dysfunction was conducted by Allain et al in 1997. The research team found that people with CFS/ME showed abnormalities of the GH-IGF (insulin growth factor) axis. A subsequent study by Moorkens et al, using a larger cohort, found that CFS/ME patients showed significant impairment of GH response during insulin-induced hypoglycemia, as well as a low nocturnal GH secretion. A number of studies have also shown low GH secretion among fibromyalgia patients. (See Holtorf article below for an excellent summary of relevant research.)
The causes of GH deficiency in CFS/ME and FM patients are various. Disruptions in the HPA axis will certainly contribute to lower production of GH. It has also been speculated that because GH is secreted during stage 3 and 4 sleep, widespread insomnia in these two groups, and the subsequent reduction of deep sleep, may be a contributory factor.
PROTOCOL. The synthetic equivalent of GH, Somatropin, is administered through injection. The standard dose is 0.2 mg three times a week. Dr. Cheney uses a much lower dose with his patients, as little as 0.2 mg once a week. He notes that higher doses cause “crashes.”
PROS AND CONS. Like most hormone treatments, the effects of Somatropin are felt throughout the body, which means it should be used with caution. Because GH upregulates the immune system, this could potentially aggravate symptoms in people with CFS/ME. Those for whom Somatropin has been of benefit report a dramatic increase in energy, as well as the additional benefit of “beautiful skin.”
AVAILABILITY AND COST. Somatropin is available by prescription only (although there is a large black market of suppliers). Somatropin is highly regulated, and difficult to obtain without a confirmation of deficiency. A single 5 mg vial costs $1500. Unfortunately, there is no substitute for GH. Taking natural GH precursors (arginine, ornithine, lysine, glutamine, GABA) is ineffective.
FURTHER READING
Good general information on Somatropin: http://www.somatropin.net/
Dr. Holtorf's excellent article on HPA axis dysfunction and GH in CFS/ME and FM. (Scroll down to find it.): http://www.holtorfmed.com/index.php?section=downloads&file_id=57
Excellent article about GH deficiency in FM http://www.myalgia.com/growth_hormone_deficiency_in_fib.htm
Dr. Cheney discusses the role of GH in CFS/ME. Includes treatment protocols http://www.dfwcfids.org/medical/advances.html
Interesting patient discussion of GH: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=999131
PATIENT REVIEWS
Patient review of somatropin: http://www.revolutionhealth.com/drugs-treatments/rating/somatropin-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Allain TJ, Bearn JA, Coskeran P, Jones J, Checkley A, Butler J, Wessely S, Miell JP. “Changes in growth hormone, insulin, insulinlike growth factors (IGFs), and IGF-binding protein-1 in chronic fatigue syndrome.” Biological Psychiatry. 1997 Mar 1;41(5):567-73. http://www.ncbi.nlm.nih.gov/pubmed/9046989 (Abstract)
Moorkens G, Berwaerts J, Wynants H, Abs R. “Characterization of pituitary function with emphasis on GH secretion in the chronic fatigue syndrome.” Clin Endocrinol (Oxf.) 2000 Jul;53(1):99-106. http://www.ncbi.nlm.nih.gov/pubmed/10931086 (Abstract)
TESTOSTERONE
DESCRIPTION. Testosterone is the principal male hormone. It is produced in the testes.
BACKGROUND. Testosterone is the hormone responsible for the development of primary male sexual characteristics (sex organs), as well as secondary characteristics such as growth of body hair, increase in bone and muscle mass, and deepening of the voice. Testosterone promotes energy and a sense of well-being, and helps regulate the HPA axis. Women also produce testosterone, although at only a tenth of male levels. Low-dose testosterone is sometimes recommended for women at risk of osteoporosis.
As men age, their production of testosterone decreases. While this is a natural process, some men experience an abrupt or dramatic decline, sometimes brought about by disease processes. This abrupt decline has been dubbed "male menopause" (although gradual declines are often referred to as "male menopause" as well). The medical community has mixed views on male menopause. Some doctors offer hormone replacement therapy, just as they do their female patients, while others view male menopause as a myth.
USES IN CFS/ME. As with other hormone deficiencies, low levels of testosterone are fairly common in CFS/ME patients. In men, this will be felt as a loss of libido, as well as a decrease in muscle strength, depression, anxiety, and bladder problems – all of which are symptoms common among CFS/ME patients of both sexes. As testosterone has such wide-ranging effects on the body, doctors should prescribe testosterone only after blood tests confirm low levels.
PROS AND CONS. Men who have taken testosterone report an increase in energy. Some men experience "teenage problems" (acne).
AVAILABILITY AND COST. Testosterone is available as an injection, gel or patch. Of the three modes of delivery, the gel (Androgel) is the least problematic. (Patches can fall off, and injections require a doctor.) Androgel is applied to the arms. It dries quickly, and leaves no residue. A 30-day supply of Androgel costs about $100, so check to see if your insurance will cover the cost.
FURTHER READING
Article about male menopause: http://men.webmd.com/guide/male-menopause
Good summary of male menopause and CFS/ME http://www.prohealth.com/library/showarticle.cfm?libid=8114
PATIENT REVIEWS
CFS/ME patient reviews of testosterone: http://www.revolutionhealth.com/drugs-treatments/rating/testosterone-for-chronic-fatigue-syndrome-cfs-cfids-me
THYROID HORMONES
CAUTION: Taking an initial high dose of T3 can lead to heart attack.
DESCRIPTION. Thyroid hormones are tyrosine-based hormones produced in the thyroid, a butterfly-shaped gland in the neck.
BACKGROUND. Thyroid hormones regulate metabolism and, as a consequence, can act on nearly every cell in the body. They increase basal metabolic rate, regulate long bone growth (along with growth hormone), and increase the body's sensitivity to adrenaline and noradrenaline. Thyroid hormones also regulate protein, fat, and carbohydrate metabolism. They stimulate the metabolism of vitamins, which means thyroid hormones regulate how much energy is available to cells. There are two primary thyroid hormones, T4 (thyroxine) and T3 (triiodothyonine). T4 is first converted in the body to T3, which is two to three times more potent than T4, and then to T2 and T1. All four are essential for the basic functioning of the human body.
USES IN CFS/ME. Fatigue is one of the hallmark symptoms of low thyroid function, therefore it is not surprising that CFS/ME patients are often suspected of having hypothyroidism. Other hypothyroid symptoms, such as low body temperature, cold intolerance, depression, hair loss, and weight gain are also quite common among CFS/ME patients, indicating that low thyroid function could be the root of many CFS/ME symptoms.
According to Dr. Teitelbaum, low thyroid function is one of the most underdiagnosed conditions in America. The reason many doctors miss the diagnosis, even in the presence of "text book" symptoms, is that testing is inadequate. Up until a few years ago the gold standard for testing the thyroid was to measure TSH levels (thyroid stimulating hormone). TSH, the hormone which stimulates the thyroid to release hormones, is produced in the pituitary gland, which means that as long as a patient has a normally functioning pituitary, the TSH results will be within normal range – regardless of how faulty his or her thyroid may be.
When clinicians realized the TSH test was inadequate, they began to use free T3 and T4 levels to determine low thyroid function, but those tests, like the previous one, missed many patients with low thyroid function, including Hashimoto's disease patients, whose thyroids are being attacked by their own immune systems, as well as nearly everyone with HPA axis dysfunction (e.g., fibromyalgia and CFS/ME patients).
This lack of sensitivity in testing has led some CFS/ME physicians to prescribe thyroid hormone supplementation to their patients even in the absence of abnormal test results.
PROTOCOL. Thyroid hormones come in two forms, synthetic and natural. T4 (Synthroid, levothyroxine) and T3 (Cytomel) are both synthetic. (T4 helps with lethargy and T3 helps with cognitive problems, "brain fog," and mental focus.) Armour Thyroid is a natural glandular which contains all four thyroid hormones (T1, T2, T3, and T4). Nature-Throid, another natural glandular, contains T3 and T4.
How patients respond to thyroid hormone therapy is highly individualized. Some do well on synthetic formulations, others do better with natural glandulars. (Although, it should be noted that Hashimoto's disease patients tend to respond better to synthetic formulations.) People with primary hypothyroidism need to take both T3 and T4, as their thyroids will not make the conversion.
Dr. Myhill advises that CFS/ME patients have their thyroid hormones checked often while on medication. Too high a dose can lead to thyrotoxicosis, a dangerous condition in which the patient experiences sweating, fever, heart palpitations, and, potentially, heart attack. Patients starting thyroid hormone therapy should always begin with the lowest possible dose.
PROS AND CONS. There is no doubt that patients with concomitant hypothyroidism experience an overall improvement with the administration of thyroid hormones. Patients report a cessation of fatigue, improvements in mood, stamina and strength, normalization of weight, and hair regrowth. Patients whose thyroid levels are normal also experience improvement in energy levels after taking thyroid hormones. However, in similar fashion to CNS stimulants, the improvement is often followed by a crash. The main drawback of taking thyroid hormone is that once hormone replacement has begun, the thyroid ceases making its own hormones. For people taking long-term thyroid hormones, discontinuation may not be possible.
FURTHER READING
Dr. Teitelbaum's recommendations for thyroid supplementation http://www.endfatigue.com/health_articles_d-e/Diet-thyroid_hormone_deficiency.html
Mary Shomon's discussion of low thyroid function in CFS/ME http://thyroid.about.com/cs/fibromyalgiacfs/a/cfsfibrothyroid.htm
Good general information about thyroid testing and CFS/ME: http://blog.nutri-living.com/?p=405
Dr. Myhill's discussion of underactive thyroid in CFS/ME http://www.drmyhill.co.uk/wiki/Hypothyroidism_-_A_Common_Hormonal_Problem_in_CFS
James Burton's article about thyroid hormone deficiencies in CFS/ME patients http://www.prohealth.com/library/showarticle.cfm?libid=10827
PATIENT REVIEWS
CFS/ME patient ratings of Cytomel: http://www.revolutionhealth.com/drugs-treatments/rating/cytomel-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Synthroid: http://www.revolutionhealth.com/drugs-treatments/rating/synthroid-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Armour thyroid: http://www.revolutionhealth.com/drugs-treatments/rating/armour-thyroid-for-chronic-fatigue-syndrome-cfs-cfids-me
HYDROCORTISONE/CORTEF
DESCRIPTION. Hydrocortisone is the pharmaceutical name for cortisol, a glucocorticoid hormone excreted by the adrenal cortex in response to stress, inflammation, and low blood sugar levels.
BACKGROUND. Cortisol is produced in the outer layer of the adrenal gland, known as the adrenal cortex. The release of cortisol is controlled by the hypothalamus, which secretes corticotropin-releasing hormone (CRH) to the pituitary gland, which in turn releases adrenocorticotropic hormone (ACTH). ACTH is carried by the bloodstream to the adrenal glands, where cortisol is then released.
Cortisol has numerous effects on body functions, including reduction of inflammation, maintenance of sodium and potassium balance, and regulation of blood sugar. Cortisol also has profound effects on protein and carbohydrate metabolism. Because cortisol can suppress the immune system (specifically the proliferation on T cells), hydrocortisone is used medically to treat inflammatory conditions such as rheumatoid arthritis, lupus, and allergies.
USES IN CFS/ME. Whether hydrocortisone should be used to treat CFS/ME is a topic of much debate among CFS/ME clinicians. Studies performed by Dr. Mark Demitrack and colleagues showing endocrine system deficiency along the hypothalamic-pituitary-adrenal axis (HPA axis) seem to indicate that there is a chronic adrenal insufficiency in patients with CFS/ME (Journal of Clinical Endocrinology and Metabolism, 1991). The low levels of cortisol found in some CFS/ME patients, combined with increased or new inflammatory responses, such as allergies, irritable bowel syndrome, and rheumatic conditions, also seem to point to the use of cortisol as a potentially effective treatment.
Several studies have confirmed that treatment with low-dose hydrocortisone increases energy levels and stamina in CFS/ME patients. In 1999 Cleare et al found that in a group of 32 CFS/ME patients treated with 5-10 mg of cortisol daily for a month, energy levels were significantly improved. In a subsequent study published in 2001, Cleare also found that low-dose cortisol restored normal adrenal responses to CRH in CFS/ME patients.
A number of prominent CFS/ME doctors include low-dose hydrocortisone as part of their CFS/ME protocols. In a 2008 study of 500 patients, Dr. Holtorf found that 5-15 mg a day of time-release hydrocortisone resulted in an overall improvement in 94% of his patients. Moreover, Dr. Holtorf states that “physiologic [low] doses of cortisol have been shown to improve cellular and hormonal immunity, including natural killer cell activity” both of which are problems with CFS/ME patients.
However, not all clinicians agree that treatment with hydrocortisone is beneficial. Cortisol can be an immune system suppressant and, in cases in which the immune system is already compromised, its effects could be disastrous. Clinicians who are critical of hydrocortisone's usefulness as a CFS/ME treatment point out that glucocorticoids are best used as a short-term treatment for severe allergic reactions. Long-term use may exacerbate the disease process.
PROTOCOL. Hydrocortisone (cortisone, cortisol) may be given as a single injection to treat severe allergic response or in acute cases of CFS/ME when immediate intervention is required. It may also be administered in pill form (Cortef) in low doses (5 to 15 mg) on a daily basis.
PROS. Many patients report a significant increase in energy and stamina from hydrocortisone. For some patients hydrocortisone makes the difference between having to lie in bed all day and being able to get up, which can make all the difference in the world for the severely ill. Single ("pulse") administrations of cortisol can be lifesaving for patients with severe allergic reactions or acute-onset CFS/ME.
CONS. Cortisol is a naturally occurring chemical. However, its use on a long-term basis, carries significant risks. When the body registers the presence of hydrocortisone, the adrenal glands decrease production. Although proponents of low-dose hydrocortisone claim that the risks are minimal, when taken over a long period of time the adrenal glands may fail to produce glucocorticoids altogether, making the patient entirely dependent on a drug source for this essential hormone.
In addition to the risk of dependency, the dosage must not be excessive or Cushing's syndrome may eventually develop, with tendencies for obesity, hypertension, osteoporosis, and mental disturbances. Side effects of even small doses of cortisol include headache, gastrointestinal disturbances, insomnia, and weakness. Hydrocortisone is strongly contraindicated for people with fungal infections.
AVAILABILITY AND COST. Hydrocortisone is available by prescription, in generic and brand-name formulations. The cost of brand (Cortef) or generic is similar, ranging from $15 to $30 a month, depending on the dosage. It is usually covered by insurance.
BOOKS
Jeffries, William. Safe Uses of Cortisol. Charles C Thomas Pub Ltd , 3rd edition. 2004. (Originally published in 1970, this is the “bible” for physicians who prescribe hydrocortisone for CFS/ME and FM.)
FURTHER INFORMATION
Excellent discussion of low-dose hydrocortisone by a CFS/ME patient detailing the dosage and effects: http://www.revolutionhealth.com/groups/me-chronic-fatigue-syndrome-support/discussions/topic/c433312d-35c5-41b1-a2b2-7be3aecc6987
Pro-health's patient thread on low-dose hydrocortisone http://www.prohealth.com/fibromyalgia/blog/boardDetail.cfm?id=1058069&b1=CHWEBO#1058069/
A review of the literature concerning low-dose hydrocortisone treatment in CFS/ME and FM: http://www.endfatigue.com/health_articles_f-n/Hormones-adrenal_problems_in_cfs.html
Discussion of low-dose hydrocortisone in CFS/ME http://enotes.tripod.com/fatigue2.htm
Dr. Teitelbaum's excellent review of HPA axis dysfunction and low-dose hydrocortisone treatment in CFS/ME patients: http://www.endfatigue.com/health_articles_f-n/Hormones-adrenal_problems_in_cfs.html
Dr. Holtorf's review of HPA axis dysfunction and study of 500 patients receiving low-dose hydrocortisone: http://www.holtorfmed.com/dr-pdf/Diagnosis%20Treatment%20CFS%20FM.pdf
Dr. Baschetti discusses the benefits of low-dose cortisol and makes a comparison of 36 shared features between Addison's disease and CFS/ME http://jcem.endojournals.org/content/84/6/2263-a.full
PATIENT REVIEWS
CFS/ME patient reviews of Cortef (hydrocortisone) http://www.revolutionhealth.com/drugs-treatments/rating/cortef-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Cleare AJ, Heap E, Malhi GS, Wessely S, O'Keane V, Miell J. “Low-dose hydrocortisone in chronic fatigue syndrome: a randomised crossover trial.”
Lancet 1999 Feb 6;353(9151):455-8. http://www.ncbi.nlm.nih.gov/pubmed/9989716 (Abstract)
Cleare AJ, Miell J, Heap E, Sookdeo S, Young L, Malhi GS, O'Keane V. “Hypothalamo-pituitary-adrenal axis dysfunction in chronic fatigue syndrome, and the effects of low-dose hydrocortisone therapy.” J Clin Endocrinol Metab. 2001 Aug;86(8):3545-54. http://jcem.endojournals.org/content/86/8/3545.full
Demitrack, Mark A, Dale, Janet K, Straus, Stephen E, Laue, Louisa, Listwak, Sam J, Dreusi, Markus JP, Chrousos, George P, and Gold, Philip W. “Evidence for Impaired Activation of the Hypothalamic-Pituitary-Adrenal Axis in Patients With Chronic Fatigue Syndrome.” Journal of Clinical Endocrinology and Metabolism. 73:1224-1234,1991.
HYPNOTICS
Ambien, Lunesta, Rozerem, Xyrem
Sleep disturbance is found in 100% of people with CFS/ME. This can manifest itself in either too much sleep (hypersomnia) or, more commonly, in poor, unrefreshing sleep. As sleep deprivation tends to worsen all other symptoms, nearly every CFS/ME physician includes an arsenal of insomnia treatments, both pharmaceutical and natural, in their protocols.
AMBIEN (zolpidem)
Ambien (generic: zolpidem) is a hypnotic that potentiates gamma aminobutyric acid (GABA) in the brain. It works very quickly (15 minutes) and has a short half-life. It is most effective for sleep initiation problems, rather than sleep maintenance. Because tolerance is easily developed, a low dose (10 mg) used intermittently for not more than twelve weeks is recommended. Common side effects are sedation, rebound insomnia, GERD, and impaired psychomotor and cognitive function the following day. While some CFS/ME patients report that Ambien gives them a good night's sleep, others report rapid heartbeat, a “trippy” feeling (hallucinations), and a general worsening of CFS/ME symptoms. Because Ambien has been associated with several deaths, (including actor Heath Ledger), it is under review in the U.S. In Australia, Zolpidem (brand: Stilnox) contains a “black box” warning.
PATIENT REVIEWS
CFS/ME patient reviews of Ambien: http://www.revolutionhealth.com/drugs-treatments/rating/ambien-for-chronic-fatigue-syndrome-cfs-cfids-me
LUNESTA (aszopiclone)
Lunesta (aszopiclone) is a short-acting sedative hypnotic used for the treatment of primary insomnia. It acts as a GABA agonist, stimulating GABA action in the brain. It is rapidly absorbed, with levels peaking at one to three hours after ingestion.
There has been considerable controversy surrounding Lunesta. In an article published in the New England Journal of Medicine in 2009, Drs. Lisa Schwartz and Steven Woloshin examined the manufacturer's clinical trials and found that Lunesta only improved sleep onset by 15 minutes as compared to placebo. Sleep duration was increased by 37 minutes. The authors concluded that “FDA approval does not mean that a drug works well; it means only that the agency deemed its benefits to outweigh its harms.”
PROTOCOL. The recommended dose is 2 mg–3 mg for adults (roughly equivalent to 10 mg of Valium). Lunesta is not available in Europe.
FURTHER READING
Schwartz, M Lisa M..D., and Steven Woloshin, M.D. “Lost in Transmission — FDA Drug Information That Never Reaches Clinicians.” N Engl J Med 2009; 361:1717-1720. October 29, 2009. http://www.nejm.org/doi/full/10.1056/NEJMp0907708
ROZEREM
Unlike most other sleep medications, Rozerem (Ramelteon) does not bind to GABA receptors. Instead it binds to melatonin receptors. Like melatonin, it is used to treat delayed sleep onset. There are no published studies indicating whether Rozerem is more effective than melatonin (which has the advantage of being much less expensive and widely available over-the-counter in the U.S. and Canada).
Like Lunesta, Rozerem came under the scrutiny of Drs. Lisa Schwartz and Steven Woloshin, who found that clinical trials revealed no subjective improvements in total sleep time, sleep quality, or the time it took to fall asleep. Outpatient trials confirmed that people didn't notice much benefit from Rozerem. Nor did it improve the ability to fall back asleep after waking, number of awakenings, total sleep time, or sleep quality.
FURTHER READING
CFS/ME patient reviews of Rozerem: http://www.revolutionhealth.com/drugs-treatments/rating/rozerem-for-chronic-fatigue-syndrome-cfs-cfids-me
XYREM
BACKGROUND. Xyrem (sodium oxybate) – also known as the “date rape drug,” or GHB – is a central nervous system depressant. Chemically, Xyrem is the equivalent of gamma hydroxobutyric acid (GHB), a naturally occurring substance found in the central nervous system. While Xyrem is widely (and illegally) available as a street drug, its use for medical purposes is highly restricted. To date, the only approved use of Xyrem is for narcolepsy, a rare condition in which people suddenly fall asleep during the day. In 2010 the makers of Xyrem, Jazz Pharmaceuticals, submitted a New Drug Approval to the FDA for fibromyalgia. Approval was denied. Xyrem is currently listed as an “orphan drug” (a drug used for rare conditions).
USES IN CFS/ME. Xyrem has gained some popularity among CFS/ME physicians for treating the intractable insomnia experienced by many CFS/ME patients. CFS/ME doctors who use Xyrem include Dr. Enlander and Dr. Klimas. Because of its potential for illegal use, physicians and patients who wish to use Xyrem must be registered with Jazz Pharmaceuticals. Registration includes a precise set of instructions for how to take Xyrem. These include not getting up after ingestion and using the bathroom before ingestion. Side effects include nausea, dizziness, headache, vomiting, sleepiness, and bed-wetting (for those who did not use the bathroom first).
PROS AND CONS. Given the popularity of Xyrem as a party drug, there is an unusual amount of data available about dosage and safety. In the general population, it is well-tolerated, safe, and quite definitely effective. Some CFS/ME patients have reported that Xyrem is a “godsend,” providing them with their first deep, refreshing sleep in years. The adverse reactions most commonly reported are nausea and headaches.
SEE: Sleep Disorders
PATIENT REVIEWS
Detailed patient experiences with Xyrem: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=809597
CFS/ME patient reviews of Xyrem: http://www.revolutionhealth.com/drugs-treatments/rating/xyrem-for-chronic-fatigue-syndrome-cfs-cfids-me
MIDODRINE (Amatine, Proamatine)
DESCRIPTION. Midodrine is an anti-hypotensive agent, that is, it causes an increase in blood pressure. It is classed as an alpha-agonist.
BACKGROUND. Midodrine was developed to treat orthostatic hypotension, a form of orthostatic intolerance (OI) in which a person's blood pressure drops upon standing. The most common cause of orthostatic hypotension is diabetes mellitis. The drug works by acting on alpha-adrenergic receptors in arteries and veins, producing an increase in vascular tone. Unlike beta-blockers, midodrine does not affect cardiac beta-adrenergic receptors. Nor does it cross the blood-brain barrier, which means it has little effect on the central nervous system.
Several studies have proven the efficacy of midodrine in patients with orthostatic hypotension. In 1997 Low et al found that in a group of 171 patients there was significant improvement in standing blood pressure, as compared to placebo. Side effects, including urinary retention, goose bumps, itching, and a feeling of "pins and needles," were minimal. In 2011 Chen et al found that midodrine was more effective than conventional therapies in 53 children with Postural Orthostatic Tachycardia Syndrome (POTS). Midodrine has also been recommended as a treatment for vasovagal syndrome (fainting), spinal cord injuries, and dysautonomia caused by Parkinson's disease.
Currently, the status of midodrine in the U.S. is unclear. After being approved and marketed, the FDA withdrew its approval of midodrine because the manufacturer had failed to complete required studies confirming its safety. Later the FDA agreed to keep it on the market as an “orphan drug” provided that the manufacturer (Shire) completed standard testing.
USES IN CFS/ME. Dysautonomia, including OI and POTS, is so common in CFS/ME that many physicians find the conditions to be virtually synonymous. In fact, Naschitz JE et al found that specific responses to a tilt table test can be used to accurately diagnose CFS/ME. A recent study in 2009 by a group of researchers at Newcastle University in England confirmed that people with CFS/ME not only have lower blood pressure but abnormal diurnal blood pressure regulation. They found that the greater the dysregulation in diurnal blood pressure, the greater the fatigue. The researchers recommended midodrine as a possible treatment. A number of CFS/ME physicians have used midodrine to treat OI in their patients, including Dr. Klimas, Dr. Rowe, and Dr. Chia.
PROTOCOL. Dr. Hugh Calkins, a cardiologist at Johns Hopkins University, recommends starting midodrine at 2.5 mg taken three times a day. Dr. Klimas suggests taking midodrine before meals. Regular blood pressure monitoring is advised. Because it lowers blood pressure, midodrine should not be taken before bed.
PROS. People with CFS/ME report an increase in stamina, a decrease in dizziness and light-headedness, and an improvement in their ability to stand for periods of time. Some report an overall improvement in symptoms. Midodrine does not pass through the blood-brain barrier, which is advantageous for patients with drug sensitivities.
CONS. Midodrine is used for patients with consistently low blood pressure. However, patients in a double-blind study also experienced a significant number of adverse effects (Journal of the American Medical Association, 1997). Nausea and headache appear to be the two most common side effects of midodrine. Chills, goose bumps, tingling, and frequent urination have also been reported. Some patients experience a sudden rise in blood pressure that feels “stroke-like.” Paradoxically, some patients experience a “crash” a few hours after taking midodrine, in which their blood pressure falls dramatically. Midodrine cannot be taken by anyone with a heart condition, hypertension or kidney disease.
AVAILABILITY AND COST. Midodrine is available from pharmacies. A bottle of 90 pills at the lowest dosage costs roughly $60.
SEE: Cardiac and Cardiovascular Symptoms
FURTHER READING
Good summary of how midodrine is used in CFS/ME. http://aboutmecfs.org.violet.arvixe.com/Trt/TrtMidodrine.aspx
“Tilt-Test Formula: A Diagnostic Marker for CFS?” CFIDS Chronicle. Spring 2003. http://www.cfids.org/archives/2003rr/2003-rr1-article02.asp
CFS/ME doctors discuss treatments for OI: http://www.co-cure.org/experts.htm
PATIENT REVIEWS
Patient reviews of midodrine: http://www.revolutionhealth.com/drugs-treatments/rating/proamatine-for-chronic-fatigue-syndrome-cfs-cfids-me?rid=13060
RESEARCH
Chen L, Wang L, Sun J, Qin J, Tang C, Jin H, Du J. “Midodrine hydrochloride is effective in the treatment of children with postural orthostatic tachycardia syndrome.” Circ J. 2011 Apr;75(4):927-31. http://www.ncbi.nlm.nih.gov/pubmed/21301135 (Abstract)
Low PA, Gilden JL, Freeman R, Sheng KN, McElligott MA. “Efficacy of midodrine vs placebo in neurogenic orthostatic hypotension. A randomized, double-blind multicenter study. Midodrine Study Group.” JAMA. 1997 Apr 2;277(13):1046-51. http://www.ncbi.nlm.nih.gov/pubmed/9091692 (Abstract)
Newton JL, Sheth A, Shin J, Pairman J, Wilton K, Burt JA, Jones DE. “Lower ambulatory blood pressure in chronic fatigue syndrome.” Psychosom Med. 2009 Apr;71(3):361-5. http://www.ncbi.nlm.nih.gov/pubmed/19297309 (Abstract)
NALTREXONE
DESCRIPTION. Naltrexone (Depade or ReVia) is an opioid antagonist. Naltrexone binds to opioid receptors in the nervous system, blocking the effects of narcotics.
BACKGROUND. Naltrexone was first synthesized in 1963 by a small pharmaceutical company in Long Island. Because of its limited application, there was virtually no interest in the drug until 1971 when the Federal government stepped in and endorsed the use of naltrexone for the treatment of heroin addiction. After ten years of trials with narcotics, the drug was determined to be useful for alcoholism. In 1995 naltrexone (ReVia) was formally approved by the FDA for the treatment of alcoholism. Derivatives of naltrexone have been also been used to treat smoking addiction.
While the Federal government was pursuing the use of naltrexone for narcotics addictions, Dr. Ian S. Zagon, Professor of Neuroscience and Anatomy at Pennsylvania State University, discovered that, in contrast to normal doses of naltrexone (50 mg), low dose naltrexone (LDN) blocked the growth of certain cancer tumors. Dr. Zagon's studies drew considerable attention from the scientific community, and researchers began to investigate other possible medical applications of LDN. In 1985 Dr. Bihari, director of the Division of Alcoholism and Drug Dependence, SUNY/Health Science Center at Brooklyn, New York, began to prescribe LDN to AIDS patients, and in the 1990s he successfully used LDN to treat multiple sclerosis. In the decade following Dr. Bihari's success with LDN, researchers found that LDN was also successful in treating Crohn's disease, rheumatoid arthritis, celiac disease, lupus and other autoimmune disorders.
Theories explaining the mechanism of LDN are still evolving. It is believed that low doses of naltrexone act to stimulate endorphins by temporarily blocking opioid receptor sites. (Endorphins are naturally occurring substances present in high concentrations during various illnesses, including viral and autoimmune disease.) Simply stated, when low dose naltrexone blocks opioid receptors for a few hours, the body produces more endorphins to compensate for the temporary lull. One particular endorphin, Opioid Growth Factor (OGF), is an important immune system regulator. When LDN blocks the receptor site for OGF, the body responds by producing more OGF, which, in turn, acts to regulate the immune system.
LDN also appears to block pain receptors along the spine. In 2009 Drs. Sean Mackey and Jarred Younger of Stanford University completed a successful trial of LDN in ten patients with fibromyalgia. The researchers found that low-dose naltrexone reduced fibromyalgia symptoms in the entire cohort, with a greater than 30% reduction of symptoms over placebo. In addition, laboratory visits showed that mechanical and heat pain thresholds were improved by the drug. Side effects were minor. They concluded that “low-dose naltrexone may be an effective, highly tolerable, and inexpensive treatment for fibromyalgia.”
USES IN CFS/ME. CFS/ME clinicians have expressed interest in naltrexone, especially in light of findings regarding naltrexone's effect on the immune system. Dr. Susan Levine, a well-known CFS/ME expert affiliated with Mt. Sinai Hospital, New York, explains the rationale for the use and success of naltrexone. "Naltrexone can act to counteract some of the negative effects of excess stimulation by endorphins, such as diminished immune function, and may help to improve cognition and listlessness" (CFIDS Chronicle, January/February 1989). One study by Dr. Levine provided encouraging results. Cognitive symptoms improved in six of ten CFS/ME patients treated with 5 mg naltrexone. No clinically significant side effects were observed.
Despite numerous studies on the immunological benefits of naltrexone, relatively few CFS/ME doctors have included LDN as part of their protocols. Dr. Klimas prescribes LDN to boost immune system responses and for pain. Dr. Enlander prescribes LDN, but remains “neutral” as to its benefits.
PROTOCOL. LDN dosage ranges from 3-5 mg. Patients who have taken LDN for several months report that it is better to start with half the lowest recommended dose (1.5 mg) and slowly work up to 3 mg a day. LDN is generally taken before bed, but may be taken during the day if sleep is disturbed.
PROS AND CONS. A number of patients have reported dramatic improvement in flu-like symptoms, energy, sleep and concentration. Some even claim that LDN has cured them of all their symptoms. Side effects are fairly mild and are usually transient: nausea, headaches, weakness, unusually vivid dreams and fatigue. Naltrexone seems to work best with patients who have had a viral onset, or who have significant flu-like symptoms (sore throat, low fever). Because naltrexone is an opioid antagonist, it cannot be taken with any narcotic pain medication, or with corticosteroids.
AVAILABILITY AND COST. LDN is available by prescription through compounding pharmacies. The cost is approximately $40 for a 30-day supply. Irmat Pharmacy in Manhattan supplies 30 capsules of 4.5mg LDN for $38. Insurance coverage may vary, so check with your carrier.
SEE: Pain
FURTHER READING
Very thorough review of the history and current uses of LDN written by Maija Haavisto. Also included are the patient's own experience with LDN http://www.fiikus.net/?ldn
Phoenix Rising discussion of LDN for CFS/ME patients. Includes explanation of how the drug works: http://aboutmecfs.org.violet.arvixe.com/Trt/LDN.aspx
Biography of Dr. Zagon and general information: http://www.ldnscience.org/ldn-researchers/119
Where to find LDN http://www.lowdosenaltrexone.org/index.htm#What_diseases_has_it_been_useful_for
General information about LDN: http://www.lowdosenaltrexone.org/index.htm
Yahoo group for low dose naltrexone http://health.groups.yahoo.com/group/lowdosenaltrexone/
PATIENT REVIEWS
CFS/ME patient reviews of naltrexone: http://www.revolutionhealth.com/drugs-treatments/rating/naltrexone-for-chronic-fatigue-syndrome-cfs-cfids-me
A patient's experience with naltrexone: http://livewithcfs.blogspot.com/2008/04/low-dose-naltrexone-treatment-for-cfs.html
Detailed information on how LDN affected the immune system of a CFS/ME patient over a two-year period. This blog is well worth reading: http://www.users.on.net/~julian.robinson/cfs/naltrexone.htm
RESEARCH
Younger J, Mackey S. “Fibromyalgia symptoms are reduced by low-dose naltrexone: a pilot study.” Pain Med. 2009 May-Jun;10(4):663-72. http://www.ncbi.nlm.nih.gov/pubmed/19453963 (Abstract)
NEXAVIR (formerly Kutapressin)
DESCRIPTION. Nexavir is a peptide and amino acid solution derived from porcine (pig) liver.
BACKGROUND. In the late 1920s, it was discovered that liver helped patients with acne vulgaris. As a result of this observation, attempts were made to isolate the active factor from liver. Not until the 1940s was a specially purified liver fraction isolated. Subsequent refinements in the isolation of the active material led to the development of what was then called Kutapressin, a biological (as opposed to synthetic) medication which had anti-inflammatory properties. Over the following decade, Kutapressin was used to treat a variety of dermatological conditions, including poison ivy, hives, eczema, and severe sunburn. According to Dr. Thomas Steinbach, Kutapressin was used decades ago to treat neurasthenia, a condition that bore a remarkable resemblance to CFS/ME.
USES IN CFS/ME. Kutapressin's value as a CFS/ME treatment did not become generally known until Dr. Thomas Steinbach and Dr. William Hermann used Kutapressin successfully in the early 1980s to treat shingles and what was then referred to as Epstein-Barr virus reactivation (CFIDS Chronicle, Summer 1990). Dr. Steinbach had observed that Kutapressin's antiviral and anti-inflammatory properties made it an effective treatment for infectious mononucleosis. Because of Kutapressin's excellent safety record and the positive results in treating Epstein-Barr virus infection, they conducted an informal unblinded study of some 270 patients with CFS/ME.
The results were impressive. Of the study participants, 75% showed improvement, and in some cases marked improvement, after only 40 injections of Kutapressin. Even more promising was that many of these patients had been ill with CFS/ME for more than five years.
The study riveted the attention of CFS/ME clinicians, because no drug treatment to date had produced such impressive results. A second study published by Dr. Steinbach and Dr. Hermann demonstrated the same impressive results (presented at the International CFIDS Conference, Albany, N.Y., 1992). Of the 130 patients who participated in the second study, 85% reported notable or marked reduction of symptoms while receiving Kutapressin injections. Of 111 patients who reported significant reductions in symptoms, 103 noted results within six months of treatment. As a result of these studies, many CFS/ME clinicians began to incorporate Kutapressin in their treatment plans, particularly when there was evidence of viral activity (high titers of human herpesvirus 6 and high interferon levels).
Some researchers have theorized that Kutapressin must have had both antiviral and immunomodulatory properties to simultaneously curtail viral reactivation and the characteristic immune system upregulation typical in CFS/ME. Kutapressin's role in suppressing viral activity is fairly well documented. A study published by Dr. D.V. Ablashi and colleagues proved that Kutapressin was a potent inhibitor of herpesvirus 6 in vitro without causing cell damage (In Vivo, 1994). A later study conducted in 1996 by Dr. E. Rosenfeld and colleagues found that Kutapressin was also effective against Epstein-Barr virus (In Vivo, 1996). However, its role in immunomodulation remains speculative. Dr. Steinbach and Dr. Hermann postulated that Kutapressin may have acted to mediate the action of lymphokines, the immune system chemicals that are thought responsible for many of the symptoms characteristic of CFS/ME.
On the heels of these promising studies, the ownership of Kutapressin changed hands. The distributor, Schwartz Pharma, sold Kutapressin, along with its client list, to Nexco Pharma, a Texas-based company. The product was renamed Nexavir, and while patients and doctors were assured that it was identical to the original formulation, this turned out not to be the case. Nexavir contains preservatives as well as tyrosine, an amino acid to which many CFS/ME patients are sensitive. This prompted some doctors to switch to Hepapressin, a bovine liver alternative. According to Dr. Steinbach, Hepapressin is not nearly effective as the original formulation of Kutapressin (personal communication).
PROTOCOL. The original protocol developed by Dr. Steinbach and Dr. Hermann consisted of a daily intramuscular injection of 2 ml of Kutapressin for 25 days followed by 2 ml injections every other day for 25 days, followed by 2 ml injections three times a week for several months. This is the protocol currently followed for Nexavir.
When he was still using Kutapressin, Dr. Cheney prescribed lower doses (1 ml) working up to 4 ml daily for six months. A 23-gauge 1-inch-long needle is recommended for deep intramuscular injection.
Many doctors who include Nexavir in their protocols (or its counterpart, Hepapressin), combine it with other medications. Dr. Enlander combines Hepapressin with magnesium, B12, folic acid and minerals. Dr. De Meirleir combines Nexavir with B12. In Dr. De Meirleir's experience with this combination, 50% of patients are pain free within three months, and sleep often normalizes within three days.
PROS. Most patients who have benefited from it note an immediate cessation of sore throats, a reduction in flu-like feelings, pain, and fatigue, and improvement in energy level. Many others have reported decreased duration and severity of episodes of flu, increased energy and stamina, and a feeling of overall improvement with Nexavir. Although Nexavir is considered safe, it does produce a few minor side effects initially, but these usually pass quickly after the first few injections are given. In most patients, side effects subside within the first 20 days of treatment.
CONS. Nexavir, although effective for some patients, is not universally helpful. A small number of patients may even feel worse, particularly those who are sensitive to tyrosine. Nexavir can involve a lot of time and money, with little gain. To that end, patients often do not continue with it for the full six months if they have noted no results after three or four months. People with allergies to pork and women who are pregnant should not take Nexavir.
AVAILABILITY` AND COST. Nexavir is available by prescription only. It costs about $145 per 20 ml vial (10 injections). A full six-month course of treatment can cost upwards of $2,000. Some insurance companies cover the cost. However, many companies consider Nexavir an experimental drug for off-label usage and will not cover the cost.
FURTHER READING
Detailed information about Nexavir http://livingwithchronicfatiguesyndrome.wordpress.com/2010/10/25/nexavir-kutapressin-for-cfs/
Dr. Steinbach's groundbreaking 1996 study of Kutapressin in CFS/ME treatment: http://www.me-cvs.nl/index.php?pageid=3423
Nice run-down of various CFS/ME doctors' Nexavir protocols: http://esme-eu.com/antivirals/nexavir-kutapressin-for-me-cfs-article447-135.html
RESEARCH
Ablashi DV, Berneman ZN, Lawyer C, Kramarsky B, Ferguson DM, Komaroff AL. “Antiviral activity in vitro of Kutapressin against human herpesvirus-6.” In Vivo. 1994 Jul-Aug;8(4):581-6. http://www.ncbi.nlm.nih.gov/pubmed/7893985 (Abstract)
Rosenfeld E, Salimi B, O'Gorman MR, Lawyer C, Katz BZ. “Potential in vitro activity of Kutapressin against Epstein-Barr virus.” In Vivo.1996 May-Jun;10(3):313-8. http://www.ncbi.nlm.nih.gov/pubmed/8797033 (Abstract)
NITROGLYCERIN
DESCRIPTION. Nitroglycerin is a nitrate commonly used to relieve angina.
BACKGROUND. Nitroglycerin is one of the oldest drugs in continual use, having been used for more than 100 years to treat angina pectoris, a condition in which a spasm of the coronary arteries causes oxygen loss (ischemia) to the heart. It is a vasodilator; that is, it causes relaxation of the blood vessels. This in turn increases the supply of blood and oxygen to meet the needs of the heart.
USES IN CFS/ME. Nitroglycerin has been used primarily to treat fibromyalgia-type pain in people with CFS/ME, although it has other uses as well. At the 1992 CFIDS conference in Albany, New York, Dr. Jay Goldstein reported that nitroglycerin not only relieved pain but often helped alleviate many other symptoms associated with low blood flow (hypoperfusion) in the brain. After initiating nitroglycerin treatment, Dr. Goldstein's patients reported a decrease in headaches, sore throat, irritable bowel-type symptoms, anxiety, and depression. They also noted increased energy and improved cognition. A point of great interest regarding nitroglycerin as a CFS/ME treatment is that some patients with concurrent multiple chemical sensitivities report improvement in symptoms.
Aside from Dr. Goldstein, very few doctors have investigated the effects of nitroglycerin on CFS/ME patients. In contrast, a number of doctors and researchers have pursued the possible benefits of nitroglycerin for those who suffer from fibromyalgia. A 2011 study by Cho et al found that in fibromyalgia patients, blood flow was restricted due to endothelial dysfunction (an imbalance between vasodilation and vasoconstriction in the inner lining of blood vessels). Nitroglycerin could potentially correct that problem.
Dr. Mark Reed, a podiatrist, prescribed nitroglycerin patches for use on the ankles of a patient with severe foot pain due to fibromyalgia. The patient reported a cessation of pain, and a return of normal skin color on her feet. The only side effect was headache, which was relieved by cutting the patches into 1/8” segments. It is possible, given its vasodilating properties, that topical nitroglycerin can be used to alleviate localized ischemic pain in other areas of the body as well.
PROTOCOL. Because nitroglycerin affects the heart, it is best to determine a specific dose with your physician (individual requirements vary). Dr. Goldstein prescribed sublingual nitroglycerin, generally 0.04 mg (more information on Dr. Goldstein's protocol can be obtained by reading Dr. Goldstein's book, Chronic Fatigue Syndrome: The Limbic Hypothesis).
PROS AND CONS. In marked contrast to other CFS/ME medications, nitroglycerin acts very quickly. Improvement in symptoms can be noted within minutes, making the drug easy to evaluate. Benefits can be global; energy, pain, cognitive function, and mood may improve significantly. However, side effects are common.
The most frequent problems are reduced blood pressure, fainting, dizziness, and headache. For this reason, nitroglycerin is usually administered while the patient is sitting. Patients with migraine headaches should not take this drug because it will worsen the condition. An additional drawback to nitroglycerin is that it loses its effectiveness over time. Dr. Goldstein states, "The most vexing problem in my use of nitroglycerin has been the development of tolerance, which is sometimes extremely rapid, occurring even after the first dose" (CFIDS Chronicle, Summer 1993).
Concurrent use of any drug that lowers blood pressure or alcohol will exaggerate the hypotensive effect of nitroglycerin. Because it is a vasodilator, patients with syncope or hypotension should avoid nitroglycerin.
AVAILABILITY AND COST. Nitroglycerin is available by prescription, in pill or patch formulation. It can be purchased as a generic drug or any of more than two dozen brand-name drugs. Nitroglycerin is inexpensive; 100 sublingual pills cost less than $30. The price of 10 patches is around $10. Insurance usually covers the cost.
FURTHER READING
Interesting article about the pain-relieving effects of nitroglycerin patches for peripheral neuropathy in a patient with FM: http://www.fmaware.org/News2fa26.html?news_iv_ctrl=-1&page=NewsArticle&id=9359
“Nitroglycerin: A Potential Mediator for Hypoperfusion in CFS.” Jay Goldstein. http://www.me-cvs.nl/index.php?pageid=3022&printlink=true&highlight=cfs
RESEARCH
Cho KI, Lee JH, Kim SM, Lee HG, Kim TI. “Assessment of endothelial function in patients with fibromyalgia--cardiac ultrasound study.” Clin Rheumatol. 2011 May;30(5):647-54. http://www.ncbi.nlm.nih.gov/pubmed/20957400 (Abstract)
OXYTOCIN (Pitocin, Syntocinon)
DESCRIPTION. Oxytocin is a hormone produced in the posterior lobe of the pituitary gland. It acts as a neuromodulator.
BACKGROUND. Oxytocin is a pituitary hormone that stimulates uterine muscle contraction and sensitizes nerves. It also controls microcirculation in the brain. Oxytocin is naturally produced in large quantities during childbirth, lactation, in response to certain stressors (hypoglycemia, exercise, hypothermia), and during sexual intercourse. Its most common medical use has been as an aid in stimulating contractions during labor. Oxytocin is also used to control postpartum uterine bleeding. The neurotransmitter dopamine stimulates oxytocin production.
Oxytocin is sometimes referred to as the “love” hormone. It produces feelings of calmness, trust and bonding while reducing anxiety and fear, all of which are important emotions to feel while caring for an infant. Oxytocin also has myriad other effects on the body. It reduces blood pressure and cortisol levels, improves pancreas and bowel function, and, of primary importance to CFS/ME patients, facilitates microcirculation in the brain. Catecholamines (adrenaline, noradrenaline) inhibit the release of oxytocin.
USES IN CFS/ME. CFS/ME clinician Dr. Jorge Flechas suggested that patients with CFS/ME might well have a deficiency in oxytocin (CFIDS Chronicle, Spring 1995). Dr. Flechas based his theory on the fact that CFS/ME patients have lower levels of two other hormones, corticotropin-releasing hormone (CRH) and arginine vasopressin (AVP), which are coexpressed with oxytocin in the same region of the brain. He pointed out that many of the symptoms of CFS/ME (pain, loss of libido, sleep disturbances, low exercise tolerance, circulatory problems, and metabolic disorders) could be generated by oxytocin deficiency.
Several CFS/ME clinicians, including Dr. Flechas, Dr. Cheney and Dr. Jay Goldstein, have used oxytocin to treat CFS/ME symptoms. They have reported increased stamina, decreased pain, and improved cognitive function in those patients who have used it. In his book, Betrayal by the Brain, Dr. Goldstein also noted a decrease in fibromyalgia pain, anxiety, depression, and perhaps even food allergies.
Dr. Cheney has observed dramatic improvement in fatigue, pain, and short-term memory in his CFS/ME patients, which he attributes oxytocin's effects on microcirculation in the brain and deep tissues. Dr. Lapp also notes that oxytocin increases blood flow to the eyes, brain and muscles in CFS/ME patients:
“You think more clearly and you see more clearly. It can be remarkable. I can give the patient a shot of oxytocin in the hip and five minutes later they will say, "I haven’t seen this clearly, I haven’t felt this well in months." It doesn’t work for everybody, but when it does, it is quite miraculous and can be a long-term therapy.”
Interestingly, several CFS/ME doctors have observed that when their patients become pregnant, their CFS/ME symptoms abate. Many attribute this improvement to an increase in oxytocin.
PROTOCOL. Oxytocin may be administered orally, sublingually, or as an intramuscular injection (IM). Dr. Cheney has used sublingual oxytocin at 10 units up to three times a day. Dr. Teitelbaum recommends 10 units IM for patients in whom a deficiency is suspected (those with pallor and cold extremities). According to Dr. Teitelbaum, effects will begin within 45 minutes to an hour. He prescribes injections daily or on an “as needed” basis. Some specialists note the benefits of oxytocin after a single injection, while others believe it takes several injections to determine if oxytocin will have a positive effect.
Dr. Cheney has used a sublingual form of oxytocin at 10 to 20 units up to three times per day. Sublingual oxytocin has the advantage of being able to spit it out if a negative reaction occurs.
PROS AND CONS. Oxytocin has so many functions in regulating primary systems in the body that it may provide, as Dr. Lapp says, nearly “miraculous” results. But, it doesn't work for everybody. Because oxytocin is a hormone which can influence nearly every system in the body, side effects can be serious: nausea, irregular heartbeat, changes in blood pressure, convulsions, headache, weight gain, dizziness, difficulty breathing, and mental disturbances. Any side effects should be reported to your physician. Pregnant women should not take oxytocin.
AVAILABILITY AND COST. Oral oxytocin (Pitocin, Syntocinon) is available by prescription only. Injectable oxytocin can be expensive, $50 for 10 ml. Nasal spray is less expensive. Belmar Pharmacy has also made available both a sublingual and oral form of oxytocin which may reduce the risk of side effects.
SUPPLIER
Belmar Pharmacy
Website: http://www.belmarpharmacy.com/oxytocin.htm
FURTHER READING
Dr. Lapp's 1997 presentation on treatments, including oxytocin http://www.prohealth.com/library/showarticle.cfm?id=2926&t=CFS/ME_FM
Detailed discussion of oxytocin, primarily as it relates to FM http://findarticles.com/p/articles/mi_m0FDL/is_3_14/ai_n27448236/
Very thorough explanation of the various functions of oxytocin by Dr. Jorge Flechas http://cypress.he.net/~bigmacnc/drflechas/abstract1.html
How oxytocin is used for fibromyalgia and chronic pain http://sacfs.asn.au/news/2011/01/01_25_oxytocin_may_offer_benefits_in_treatment_of_chronic_pain.htm
PATIENT REVIEWS
Blog of one patient's unsuccessful treatment with oxytocin http://livingwithchronicfatiguesyndrome.wordpress.com/2010/07/05/oxytocin-for-cfs/
PAIN RELIEVERS (ANALGESICS)
Aspirin, NSAIDs, Tylenol, Aleve, Ultram, Narcotics
NOTE: Most analgesics are available over the counter, but it is still important to discuss dosage and side effects with your physician, especially if any of these medications are taken regularly.
DESCRIPTION. Analgesics are agents that diminish pain.
BACKGROUND. Analgesics, or pain killers, work by blocking the body's production of hormones that send pain messages to the brain (prostaglandins) or by occupying the sites that receive those messages. The two general types of analgesics are non-narcotics, which block chemical production, and narcotics, which block reception in the brain. Non-narcotic pain killers include aspirin and other salicylates, acetaminophen (Tylenol), naproxen (Aleve) and nonsteroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen (Advil, Motrin). Narcotic pain killers include the opiates and opioids, such as codeine, Darvon or Wygesic (propoxyphene), Demerol (meperidine), and morphine. Because narcotics are habit-forming, they are used on a short-term basis only. A number of prescription analgesics contain a combination of non-narcotic and narcotic pain killers. The most common combinations contain codeine and acetaminophen or aspirin. These drugs are used when pain persists or is not relieved by other non-narcotic or narcotic drugs.
ASPIRIN
DESCRIPTION. Aspirin is a salicylate, a group of drugs with many medicinal uses, including reduction of fever and inflammation, as well as exhibiting mild antibiotic properties. Aspirin blocks pain by inhibiting the enzyme cyclooxygenase (COX-1), which helps the body produce inflammation-causing prostaglandins. The main active ingredient in aspirin is acetylsalicylic acid, a chemical that was first derived from willow bark.
Aside from blocking pain, aspirin has a number of physiological mechanisms. It has been shown to prevent glutamate toxicity in the brain. Glutamate is a neuroexcitatory neurotransmitter which is frequently high in CFS/ME patients. Aspirin also reduces ATP storage pools, which increases bleeding time; increases extracellular adenosine, which is associated with short-term energy increase; and lowers inducible nitric oxide synthase activity (NO mediates vasodilation in blood vessels).
USES IN CFS/ME. Aspirin is recommended for those CFS/ME patients with continual or severe joint and muscle pain. In his book, The Doctor's Guide to Chronic Fatigue Syndrome, Dr. David Bell notes that aspirin is beneficial for CFS/ME patients with "prominent joint and muscle pain, headache, lymph node pain and general aching, and is less effective in patients with prominent fatigue, nausea, and neurologic symptoms."
PROTOCOL. Aspirin can be taken as needed to prevent or treat pain. Dr. Bell suggests that some patients with intractable pain may benefit from daily use of aspirin. To avoid stomach upset, aspirin should be taken with food. As with other drugs, it is best to begin with a small dose to assess tolerance.
PROS. For many patients, aspirin is an inexpensive, reliable analgesic. Some patients report an increase of energy after taking aspirin, probably due to the temporary increase of adenosine.
CONS. Although aspirin is generally regarded as safe, frequent use can lead to a number of side effects, including tinnitus (ringing in the ears), nausea, and heartburn. If aspirin is taken on a regular basis, an anti-ulcer medication (such as Cytotec, Zantac or Tagamet) may also be recommended to protect the lining of the stomach. Patients with a history of ulcers, gastroesophageal reflux, or other gastrointestinal problems should avoid aspirin. Some nutritionists recommend that patients with food sensitivities avoid salicylates. Aspirin should not be given to children because it can cause Reye's syndrome.
AVAILABILITY AND COST. Aspirin is available over the counter at any pharmacy and most supermarkets. It is quite inexpensive, often less than $5 for a bottle of 300 tablets. Check the label carefully because some aspirin brands contain other potentially irritating ingredients, such as caffeine.
RESEARCH
Crisanti P, Leon A, Lim DM, Omri B. “Aspirin prevention of NMDA-induced neuronal death by direct protein kinase Czeta inhibition.” J Neurochem. 2005 Jun;93(6):1587-93. http://www.ncbi.nlm.nih.gov/pubmed/15935075?dopt=Abstract (Abstract)
Czyz M, Watala C. [Aspirin--the prodigious panacea? Molecular mechanisms of the action of acetylsalicylic acid in the organism]. Postepy Hig Med Dosw (Online). 2005 Mar 23;59:105-15. http://www.ncbi.nlm.nih.gov/pubmed/15928593 (Abstract)
PATIENT REVIEWS
A CFS/ME patient's review of Bayer aspirin http://www.revolutionhealth.com/drugs-treatments/rating/bayer-aspirin-for-chronic-fatigue-syndrome-cfs-cfids-me
NSAIDs
Ibuprofen (Advil, Motrin), Naproxen (Aleve), Nabumetone (Relafen), Celecoxib (Celebrex), Meloxicam (Mobic), diclofenac (Arthrotec)
DESCRIPTION. Nonsteroidal anti-inflammatory drugs (NSAIDs) act by inhibiting prostaglandin production by blocking both COX-1 and COX-2. Like aspirin, they reduce inflammation, pain, and fever. Unlike aspirin, which is cleared from the body quickly, NSAIDs have a long half-life and thus require less frequent administration. Their lower dosage leads to fewer side effects. There is also a class of strictly COX-2 inhibitors, of which Celebrex is the most common. These produce greater risks of side effects and should not be taken with other NSAIDs.
USES IN CFS/ME. NSAIDs are recommended to treat recurring pain in muscles and joints. Many patients with CFS/ME who have chronic acute pain prefer ibuprofen (Advil, Motrin) over other pain medications.
PROTOCOL. NSAIDs are generally taken as needed. Patients should start with a small dose to assess tolerance.
PROS. Some CFS/ME patients report that taking ibuprofen gives them an extra “boost.” Because NSAIDs actively work to reduce inflammation, they may work better on joint pain and stiffness than other analgesics.
CONS. Because all NSAIDs can produce gastrointestinal problems, caution must be exercised. Buffered or enteric-coated drugs help protect the stomach lining. The medication should always be taken with food. Finally, patients should be alert for signs of gastrointestinal distress (heartburn, reflux, pain). NSAIDs raise blood pressure, so patients with a history of hypertension should avoid taking them. NSAIDs are also contraindicated for patients with a history of kidney problems.
AVAILABILITY AND COST. NSAIDs are available over the counter. The most common is ibuprofen (Advil, Motrin). A bottle of 50 tablets of Advil (200 mg) costs around $5.00. Prescription NSAIDs include Clinoril, Feldene, and Tolectin. Intramuscular Toradol may be prescribed for severe pain. NSAIDs are generally more expensive than aspirin or acetaminophen.
PATIENT REVIEWS
CFS/ME patient reviews of Advil: http://www.revolutionhealth.com/drugs-treatments/rating/advil-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Aleve: http://www.revolutionhealth.com/drugs-treatments/rating/aleve-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Arthrotec: http://www.revolutionhealth.com/drugs-treatments/rating/arthrotec-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Celebrex: http://www.revolutionhealth.com/drugs-treatments/rating/celebrex-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Mobic: http://www.revolutionhealth.com/drugs-treatments/rating/mobic-for-chronic-fatigue-syndrome-cfs-cfids-me
CFS/ME patient reviews of Naproxen: http://www.revolutionhealth.com/drugs-treatments/rating/naprosyn-for-chronic-fatigue-syndrome-cfs-cfids-me
ACETAMINOPHEN (Tylenol)
CAUTION: In January 2011, the FDA limited the use of acetaminophen-opioid combinations due to the risk of liver failure. These include hydrocodone with acetaminophen (Vicodin, Lortab), and oxycodone with acetaminophen (Tylox, Percocet).
USES IN CFS/ME. In contrast to NSAIDs, which work by inhibiting signals to the nervous system, acetaminophen (Tylenol) acts in the brain, where it blocks the perception of pain. As a consequence, acetaminophen is not of particular benefit in treating joint or muscle pain due to inflammation. Its primary uses in CFS/ME are to relieve headache and generalized achiness, and to reduce fevers.
PROS. Acetaminophen does not cause stomach irritation, as do aspirin and other NSAIDs. However, a number of patients with CFS/ME find they can tolerate only low or infrequent doses.
CONS. A serious problem associated with acetaminophen is that high doses can lead to liver damage—as can any dose of this drug taken with alcohol. Acetaminophen also interacts in a similar fashion with opioids (narcotics). If signs of liver malfunction develop (jaundice or pain under the right side of the rib cage), acetaminophen should be discontinued immediately.
AVAILABILITY AND COST. Acetaminophen is available over the counter in brand-name and generic formulations. It is inexpensive. A bottle of 24 capsules costs less than $6.00.
FURTHER READING
Study linking acetaminophen to liver failure: http://www.masscfids.org/resource-library/3-research/61-increasing-number-of-fatal-acute-liver-failure-cases-linked-to-the-popular-painkiller-acetaminophen-tylenol
PATIENT REVIEWS
CFS/ME patient reviews of Tylenol: http://www.revolutionhealth.com/drugs-treatments/rating/tylenol-for-chronic-fatigue-syndrome-cfs-cfids-me
ULTRAM
DESCRIPTION. Ultram (tramadol) is a centrally acting synthetic opioid analgesic used for severe pain.
BACKGROUND. Tramadol was developed in the 1970s by the German company Grunenthal GmbH. Somewhat like narcotics, it is an opioid agonist, releasing serotonin and inhibiting the uptake of norepinephrine. Because tramadol is structurally similar to Effexor, it has been proposed as a treatment for mood disorders, phobias and anxiety, although physicians have not endorsed it for these uses.
USES IN CFS/ME. Ultram has been prescribed to treat muscle and fibromyalgia-type pain that has been resistant to other medications.
PROS. Some patients report that Ultram is the most effective medication for pain and that it also helps relieve insomnia and fatigue. Ultram acts quickly and does not seem to produce as many side effects as other pain medications.
CONS. Ultram is addictive. Withdrawal symptoms from extended use are more severe than for other opioids, and last for a longer period of time. This drug is contraindicated in patients with seizure disorders and those taking monoamine oxidase inhibitors (MAOIs) or other antidepressants.
AVAILABILITY AND COST. Tramadol is available by prescription. The generic is relatively inexpensive. Thirty tablets costs around $20.
PATIENT REVIEWS
CFS/ME patient reviews of Ultram: http://www.revolutionhealth.com/drugs-treatments/rating/ultram-for-chronic-fatigue-syndrome-cfs-cfids-me
NARCOTICS
USES IN CFS/ME. The subset of CFS/ME patients with severe, burning, intractable pain that does not respond to other treatments may need stronger medications. In these cases, narcotics may be recommended. Although effective, narcotics are addictive and therefore should be used only when other pain treatments have failed to alleviate pain.
PROS. Narcotics offer immediate and sometimes total relief from certain types of pain. Some CFS/ME patients with fibromyalgia report that a single injection of Demerol may relieve pain for up to 6 months. The reasons for this are not clear, but for some patients breaking the cycle of pain reception in the brain seems to have long-term benefits.
CONS. Narcotics can be used only infrequently and in small doses because the risk of addiction is high. The most common side effects are drowsiness, mood changes, and constipation. Codeine also causes stomach upset. The higher the dose, the more serious the side effects. High doses, for example, may cause breathing problems; therefore, patients with a history of respiratory problems should exercise caution or avoid narcotics entirely.
FURTHER READING
CFIDS Association of America's list of commonly used analgesics and side effects http://www.cfids.org/resources/analgesic.asp
FDA limits use of acetaminophen-opioid combinations: http://www.fightingfatigue.org/?p=8933
PENTOXIFYLLINE (Trental)
DESCRIPTION. Pentoxifylline (Trental) is a hemorrheologic agent derived from xanthine. A number of stimulants, including caffeine, are derived from xanthine.
BACKGROUND. Pentoxifylline improves capillary blood flow by increasing the flexibility of red blood cells and lowering blood viscosity. This double action enables blood cells to squeeze through tiny capillaries with greater ease. Traditionally, pentoxifylline is used to treat vascular diseases, especially those that inhibit blood flow. Pentoxifylline is also used to treat the nausea and headaches associated with altitude sickness.
USES IN CFS/ME. Some clinicians have recommended pentoxifylline in CFS/ME to increase blood flow to the brain. Single-photon emission computed tomography (SPECT) scans consistently reveal lowered blood flow in patients with CFS/ME. In theory, pentoxifylline should resolve that problem.
Pentoxifylline may also address another blood problem common to CFS/ME. Dr. L.O. Simpson, a pathologist from the University of Otago Medical School in
Dunedin, New Zealand, discovered that patients with CFS/ME have irregularly shaped red blood cells, which makes it more difficult for blood cells to pass through capillaries. Dr. Simpson believes the decreased cerebral blood flow in CFS/ME is the consequence of abnormally shaped blood cells. Many of the symptoms of inadequate blood supply such as light-headedness, vertigo, and cognitive problems might be alleviated if blood flow is increased.
Apart from pentoxifylline's well-known effects on blood flow, it also has broad antiviral activity. A study conducted in 1993 by a team of Russian scientists found that trental [pentoxifylline] was an “effective broad spectrum virus inhibitor.” Pentoxifylline also has the ability to inhibit proinflammatory cytokines, which have been shown to be upregulated in CFS/ME patients.
PROTOCOL. The usual recommended dose for vascular problems is 400 mg three times a day, with meals. Patients with CFS/ME should begin with a lower dose (400 mg once a day) to assess sensitivity.
PROS AND CONS. CFS/ME patients who have benefited from pentoxifylline report dramatic improvement in cognitive function as well as a reduction in flu-like symptoms (sore throats, swollen glands, and malaise). Pentoxifylline should not be used by those who cannot tolerate stimulants. (Xanthine, from which pentoxifylline is derived, is closely related to caffeine.) Pentoxifylline is contraindicated in patients with peptic ulcers and those at risk for hemorrhage. The most commonly reported side effects are nausea, headache and flushing.
AVAILABILITY AND COST. Pentoxifylline is available by prescription. It is not expensive. Ninety tablets can cost as little as $20.
FURTHER READING
A very thorough discussion of one patient's experiences with pentoxifylline. http://livingwithchronicfatiguesyndrome.wordpress.com/2011/09/05/pentoxifylline-for-me/
An excellent CFS Report on Les Simpson, blood flow and fatigue in CFS. http://www.cfidsreport.com/Articles/researchers/lessimpson.htm
RESEARCH
Amvros'eva TV, Votiakov VI, Andreeva OT, Vladyko GV, Nikolaeva SN, Orlova SV, Azarova IA, Zgirovskaia AA. “New properties of trental as an inhibitor of viral activity with a wide range of activity.” Vopr Virusol. 1993 Sep-Dec;38(5):230-3. http://www.ncbi.nlm.nih.gov/pubmed/8284924 (Abstract)
PLAQUENIL
DESCRIPTION. Plaquenil (hydroxychloroquine) is an antimalarial drug. Chemically, it is classed as a 4-aminoquinoline compound.
BACKGROUND. Hydroxychloroquine is one of a number of drugs that have been used for many years in the treatment of malaria. It has also been used to treat a number of autoimmune and inflammatory disorders, including systemic lupus, rheumatoid arthritis, and Sjögren's Syndrome. Hydroxychloroquine reduces the activation of dendritic cells, thus mitigating the inflammatory process.
USES IN CFS/ME. Hydroxychloroquine (Plaquenil) is prescribed to CFS and FMS patients if they have a high ANA level plus symptoms of Sjögren's syndrome, lupus, or other autoimmune diseases. Patients starting hydroxychloroquine therapy should have an ophthalmology exam every six months to monitor for retina toxicity.
PROTOCOL. As very few doctors use Plaquenil for CFS/ME, there is no protocol.
PROS AND CONS. Some patients report a decrease in pain and insomnia. The drawbacks, however, do not justify the benefits, which may be obtained through other less risky medications. As with all chloroquine medications, there are numerous serious side effects. People of African descent can develop severe anemia. In children, Plaquenil can be fatal.
Plaquenil diffuses rapidly into adipose (fatty) tissues, which are found abundantly in the nervous system and eyes. Permanent eye damage (retinal and corneal), including blindness, has been reported. Some patients experience psychosis (hearing voices, delusions, hallucinations, disorientation). The 4-aminoquinoline compounds are very rapidly and completely absorbed after ingestion, which means accidental overdoses, even at low doses, can occur. Toxic symptoms can occur within 30 minutes. These consist of headache, drowsiness, visual disturbances, cardiovascular collapse, and convulsions, followed by sudden and early respiratory and cardiac arrest (death).
AVAILABILITY AND COST. Plaquenil is available by prescription only.
FURTHER READING
Patient thread on Plaquenil: http://forums.phoenixrising.me/showthread.php?3171-Plaquenil-hydroxychloroquine
PATIENT REVIEWS
One patient's review of Plaquenil: http://www.revolutionhealth.com/drugs-treatments/rating/hydroxychloroquine-for-chronic-fatigue-syndrome-cfs-cfids-me
PYRIDOSTIGMINE (Mestinon)
DESCRIPTION. Pyridostigmine (brand: Mestinon) is an acetylcholinesterase inhibitor. Pyridostigmine is poorly absorbed in the gut and does not cross the blood-brain barrier.
BACKGROUND. Pyridostigmine works by preventing the breakdown of acetylcholine (ACh) in nervous system synapses. This leads to an increase in acetylcholine, a neurotransmitter widely found in both the peripheral and central nervous systems. Acting as both an excitatory and inhibitory neurotransmitter, acetylcholine performs a variety of functions. Within the skeletal muscular system it contracts muscle, allowing for movement. It slows the heart, and promotes REM sleep. In the central nervous system, ACh is closely associated with learning, attention, and short-term memory.
Pyridostigmine is mainly prescribed for myasthenia gravis, an autoimmune condition in which acetylcholine is blocked, leading to profound muscle weakness. In spite of the fact that it does not cross the blood-brain barrier, pyridostigmine is also used to enhance memory in people with Alzheimer's disease. Pyridostigmine has been administered as a treatment for the paralysis caused by organophosphate pesticide poisoning. In a similar vein, the military administered pyridostigmine as a prophylactic to soldiers during the Gulf War to block potential exposure to Soman, a nerve gas which acts on acetylcholine in much the same manner as organophosphate pesticides. Recently, pyridostigmine has been used to treat orthostatic intolerance.
USES IN CFS/ME. In his book, Betrayal by the Brain, Dr. Jay Goldstein proposed that pyridostigmine can be used in CFS/ME with much the same results as in patients with myasthenia gravis: the alleviation of muscle weakness. Surprisingly, Dr. Goldstein found that even though pyridostigmine does not cross the blood-brain barrier it increased mental clarity in his CFS/ME patients. He noted that because pyridostigmine helps increase the secretion of growth hormone (GH), it might be of benefit to CFS/ME patients, who tend to have low levels of GH.
In 2003 a group of Japanese researchers published a study in which low-dose pyridostigmine was administered to three CFS/ME patients with dysautonomia and positive Epstein-Barr virus (EBV) titers. In all three cases, a one-month course of pyridostigmine relieved fatigue and muscle weakness. The authors speculated that EBV infection induces antibodies, which, through an inhibition of calcium influx at motor terminals, reduces acetylcholine release and causes muscle weakness and cholinergic autonomic dysfunction. The authors concluded that their case studies “strongly suggest therapy using a small dose (10 mg per day) of oral pyridostigmine in patients with CFS who have had more than a 40% amplitude increase in response to the RNS [repetitive nerve stimulation] test, positive anti-VCA IgG of EBV and mild impairment of autonomic functions.”
Based on findings that pyridostigmine increases growth hormone, a 2008 study of fibromyalgia patients in Portland, Oregon was conducted comparing exercise, diet and treatment with pyridostigmine. While the researchers did not find that either pyridostigmine alone or pyridostigmine plus exercise produced an improvement in most FM symptoms, they did find that pyridostigmine improved anxiety and sleep. The authors speculated that pyridostigmine may have improved vagal tone, thus alleviating sleep and anxiety symptoms.
PROS AND CONS. CFS/ME patients report a decrease in fatigue and post-exertional malaise. However, there are many side effects if taken at normal recommended doses. Common side effects include increased saliva, increased sweating, increased urination, watery eyes, stomach upset, stomach pain, nausea, warmth, tingling, and diarrhea.
AVAILABILITY AND COST. Pyridostigmine is available at most pharmacies with a prescription. A 30-day supply of generic 60 mg tablets costs about $20. Insurance usually covers the cost.
PATIENT REVIEWS
FM patient reviews of Mestinon (pyridostigmine): http://www.revolutionhealth.com/drugs-treatments/rating/mestinon-for-fibromyalgia-syndrome-fms
RESEARCH
Arvat E, Cappa M, Casanueva FF, Dieguez C, Ghigo E, Nicolosi M, Valcavi R, Zini M. “Pyridostigmine potentiates growth hormone (GH)-releasing hormone-induced GH release in both men and women.” J Clin Endocrinol Metab. 1993 Feb;76(2):374-7. http://www.ncbi.nlm.nih.gov/pubmed/8432781 (Abstract)
Jones KD, Burckhardt CS, Deodhar AA, Perrin NA, Hanson GC, Bennett RM. “A six-month randomized controlled trial of exercise and pyridostigmine in the treatment of fibromyalgia.” Arthritis Rheum. 2008 Feb;58(2):612-22. http://www.ncbi.nlm.nih.gov/pubmed/18240245 (Abstract)
Kawamura, Yasuo, Mikihiro Kihara, Kazuhiro Nishimoto, Mayumi Taki. “Efficacy of a half dose of oral pyridostigmine in the treatment of chronic fatigue syndrome: three case reports.” Pathophysiology 9 (2003) 189-194. http://www.cfids-cab.org/cfs-inform/Coicfs/kawamura.etal03.pdf
QUESTRAN (cholestyramine)
DESCRIPTION. Questran (cholestyramine) is a bile sequestrant; it attaches to bile in the intestines and removes it.
BACKGROUND. Bile is produced in the liver. When it is released via the gall bladder into the small intestine, it serves to break down fats. Bile is then reabsorbed by the ileum (the portion of the small intestine where it joins the large intestine). In some situations, such as GI surgery or Crohn's disease, the bile is not properly reabsorbed, resulting in a watery green diarrhea. Questran helps bind bile acids, reducing diarrhea. Questran's binding action is useful for the pruritus (itching) experienced by people with liver failure, and for reducing high levels of cholesterol in the bloodstream. Questran also binds to mold toxins, and is used by some alternative doctors to treat “sick building syndrome.”
USES IN CFS/ME. The idea that CFS/ME patients suffer from neurotoxicity and oxidative stress is not a new one. Normally, CFS/ME physicians treat their patients with a combination of antioxidants (for oxidative stress) and nervous system down regulators, such as Klonopin (for neurotoxicity). However, it was Dr. Shoemaker's treatment of oxidative stress in mold toxicity, chronic Lyme and other bacterial infections with Questran that led to its use in CFS/ME.
PROTOCOL. The normal recommended dose of Questran is one packet (4 oz) of powder mixed into a beverage and drunk slowly. Dr. Cheney recommends that CFS/ME patients start with as little as ¼ teaspoon at bedtime. Be sure to drink plenty of water during the day as Questran is very constipating. Because Questran absorbs everything in your intestinal tract, you should not take Questran within an hour of taking other medications.
PROS AND CONS. Nothing will stop diarrhea faster than Questran, which is a boon to people who experience diarrhea often. Questran is a medication with a good safety record and with few side effects. However, it is a stomach irritant. Because it binds to bile and fats, it not only can cause constipation, but can lead to deficiencies in fat-soluble vitamins. Questran contains sugar, which is not recommended for CFS/ME patients. Questran “Light” contains aspartame, which is also not recommended. Notwithstanding these drawbacks, some CFS/ME patients swear by it.
AVAILABILITY AND COST. Questran is quite expensive, but if you buy generic cholestyramine powder the price drops considerably. (A single dose of brand costs about $2, whereas generic costs roughly 40 cents.) Insurance usually covers.
FURTHER READING
Basic drug information about Questran: http://www.drugs.com/pro/questran.html
Summary of Dr. Cheney's protocol: http://www.dfwcfids.org/medical/cheney.html
Dr. Teitelbaum's recommendations for how best to take Questran: http://www.endfatigue.com/tools-support/Neurotoxins-Information-Sheet.html
CFS/ME patient reviews of Questran: http://www.revolutionhealth.com/drugs-treatments/rating/questran-for-chronic-fatigue-syndrome-cfs-cfids-me
RITUXIMAB
DESCRIPTION. Rituximab (trade names: Rituxan, MabThera) is a monoclonal antibody which acts against the protein CD20. Rituximab was first approved by the FDA in 1997 for the treatment of non-Hodgkin's lymphoma.
BACKGROUND. All cells have receptors on their surfaces which allow molecules to attach themselves and cause metabolic changes within the cell. One of these receptors, primarily found on the surface of B cells, is called CD20. Molecules that attach to CD20 can affect the growth and development of tumor cells, and, sometimes, cause the production of new tumor cells. Tests confirming the expression of CD20 antigens are important in diagnosing B-cell lymphomas and leukemia.
Rituximab was developed using cloning and recombinant DNA technology from human and murine (mice or rat) genes. It is believed that rituximab destroys tumors by attaching to the CD20 receptor on B cells, causing the tumor cells to disintegrate. In some non-Hodgkin's B-cell lymphomas, rituximab prevents the production of more tumor cells.
Rituximab is also used in the treatment of autoimmune disorders, such as rheumatoid arthritis and Wegener's granulomatosis. In these cases, rituximab works by temporarily depleting the total number of B cells, which are important in promoting inflammation. Rich Van Konynenburg has proposed that this is the reason rituximab may work for CFS/ME patients – by reducing B cells, rituximab reduces inflammation.
USES IN CFS/ME. The effect of rituximab on CFS/ME patients was discovered by accident. Two Norwegian doctors, Øystein Fluge and Olav Mella of Haukeland University Hospital, noticed that after treating a CFS/ME patient for Hodgkin's lymphoma with rituximab, she recovered from CFS/ME. This led the doctors to initiate a small study of rituximab on CFS/ME patients.
Three CFS/ME patients were given rituximab in an open-label trial (that is, the patients knew they were receiving the drug). All three patients experienced significant improvement; two of them responded within six weeks and the third had a delayed response, occurring six months after treatment. The positive effects lasted for between 16 and 44 weeks. After relapse, the patients were administered another dose of rituximab, with the same positive results. The investigators hypothesized that B cells of the immune system might play a significant role in CFS, at least for a subset of patients, and that “CFS may be amenable to therapeutic interventions aimed at modifying B-cell number and function.”
The positive results of this, as well as a second open-label trial, led Drs. Fluge and Mella to conduct a larger study with a more rigorous design to test the effects of the drug. In 2009 they initiated a double-blind, placebo-controlled phase trial with 30 CFS/ME patients. As in the earlier open-label studies, the responses to rituximab were significant. Sustained overall improvements were noted in 67% of the patients (as opposed to 13% of the control group). Four of the rituximab patients showed improvement past the study period. The authors concluded that the delayed responses starting from 2–7 months after rituximab treatment, in spite of rapid B-cell depletion, “suggests that CFS is an autoimmune disease and may be consistent with the gradual elimination of autoantibodies preceding clinical responses.”
The result of this study not only generated headlines all over the world, but prompted an unprecedented apology from the Norwegian Directorate of Health. In a televised announcement, Deputy Director Bjørn Guldvog stated: "I think that we have not cared for people with ME to a great enough extent. I think it is correct to say that we have not established proper health care services for these people, and I regret that."
FURTHER READING
“Rituximab Trial Shows Promise.” Kimberly McCleary. CFIDS Association of America. http://www.research1st.com/2011/10/19/rituximab-trial/
ABC article on rituximab study: http://abcnews.go.com/Health/Wellness/chronic-fatigue-syndrome-study-supports-autoimmune-disease-theory/story?id=14801908
“Norwegian research breakthrough can solve CFS mystery.” English translation of first Norwegian news article on Rituximab: http://www.tv2.no/nyheter/innenriks/english-version-norwegian-research-breakthrough-can-solve-cfsmystery-3615631.html
“Will rituximab be a viable treatment option for ME/CFS.” A thoughtful, clear analysis of the possible role of rituximab as a treatment for CFS/ME. http://www.masscfids.org/resource-library/9/351
Cort Johnson's review of rituximab, including an interview with Dr. Olav Mella: http://esme-eu.com/treatment/a-drug-for-me-cfs-the-rituximab-story-article468-110.html
Apology from the Norwegian Directorate of Health. http://www.euro-me.org/news-Q42011-003.htm
List of rituximab clinical trials. http://www.clinicaltrials.gov/ct2/results?term=rituximab
Dr. Jamie-Deckhoff-Jones' fascinating blog. Scroll down for her explanation of how rituximab works in CFS/ME, as well as her personal critique. Both are quite good. http://treatingxmrv.blogspot.com/2011/10/rituximab-big-guns-for-mecfs.html
RESEARCH
Fluge, Øystein, Olav Mella. “Clinical impact of B-cell depletion with the anti-CD20 antibody rituximab in chronic fatigue syndrome: a preliminary case series.” BMC Neurol. 2009 Jul 1;9:28 http://www.ncbi.nlm.nih.gov/pubmed/19566965 (Abstract)
Fluge, Øystein, Ove Brulan, Kristin Risa, Anette Storstein, Einar K. Kristoffersen, Dipak Sapkota, Halvor Næss, Olav Dahl, Harald Nyland, Olav Mella. “Benefit from B-Lymphocyte Depletion Using the Anti-CD20 Antibody Rituximab in Chronic Fatigue Syndrome. A Double-Blind and Placebo-Controlled Study.” http://www.plosone.org/article/info%3Adoi%2F10.1371%2Fjournal.pone.0026358
Vandermeer's critique of Fluge et al double-blind study.
http://www.plosone.org/annotation/listThread.action?inReplyTo=info%3Adoi%2F10.1371%2Fannotation%2F43f3e6a8-cf7d-4438-8b97-b21b9c31bf5c&root=info%3Adoi%2F10.1371%2Fannotation%2F43f3e6a8-cf7d-4438-8b97-b21b9c31bf5c
Fluge and Mella's response to Vandermeer's critique. (This is well worth reading, as it lays the foundation for CFS/ME as an autoimmune disease.) http://niceguidelines.blogspot.com/2011/10/dr-oystein-fluge-and-professor-olav.html
TRANSFER FACTOR
DESCRIPTION. Transfer factor, an extract from peripheral blood lymphocytes (white blood cells) of a healthy donor, facilitates the transfer of T cell-mediated immunity from one person to another.
BACKGROUND. Transfer factor has been used for more than 40 years to transfer immunity from a presumably healthy donor to a recipient. It has been used to treat viral, parasitic, and bacterial infections. Distinctive types of transfer factor may be used, depending on the condition being treated. Nonspecific transfer factor from a pool of healthy donors may be used for immune system modulation. Disease-specific transfer factor is used to treat a specific virus or infection, such as herpesviruses or human immunodeficiency virus (HIV). In addition, donor-specific or dedicated donor transfer factor can be obtained from a relative or other household member.
USES IN CFS/ME. Transfer factor, at least in theory, would appear to be valuable as a primary therapy in CFS/ME. Because the cause of CFS/ME is still unknown, it has been difficult to find a universally effective treatment. Transfer factor is considered adaptogenic; that is, it can boost a deficient immune system or, conversely, can down regulate the immune system in certain autoimmune conditions. This makes it an ideal immunomodulator in CFS/ME. However, as the following data reveal, reports of the efficacy of transfer factor have been inconclusive.
At the May 1994 CFIDS conference in Dublin, Ireland, information was presented regarding a study of 20 patients with CFS treated with oral transfer factor by Dr. Giancarlo Pizza and colleagues from Bologna, Italy. Of the 20 patients, improvement was noted in 12 and remission was observed in two. There were no significant side effects. This oral form of transfer factor was specific for Epstein-Barr virus, cytomegalovirus, human herpesvirus 6, and herpes simplex virus.
Dr. Perry Orens of Great Neck, New York, reported a positive experience with transfer factor (CFIDS Chronicle, Fall 1993). With Dr. Hugh Fudenberg, a leading international expert on transfer factor, Dr. Orens used injectable, donor-specific transfer factor to treat symptoms of CFS in nine patients. The results were complete remission in two patients, marked improvement in two, partial improvement in two, and no improvement in three.
In 1991 Dr. Denis Wakefield of Australia reported the results of an extensive double-blind study of transfer factor. Of 90 patients with CFS, 46 received the transfer factor and 44 received a placebo. Twenty-five patients received specific transfer factor donated by a family member and 21 received transfer factor from an unrelated donor (a healthy control). Follow-up three months later showed no difference in quality of life, immunological assessment, or activity levels. It was concluded that neither specific nor nonspecific transfer factor were of benefit. It is important to note that the treatment consisted of only eight injections, given over the course of a month. It is possible that the short duration of treatment affected the outcome.
At the 2003 AACFS Conference held in Chantilly, Virginia, Dr. Brewer presented the results of a study in which 28 CFS patients were given a transfer factor (TF) preparation derived from bovine colostrum that has activity against HHV-6. Ten CFS patients (controls) received a similar TF preparation derived from bovine colostrum, except that it was devoid of any specific activity for HHV-6. Following the administration of the HHV-6 transfer factor preparation, improvements were noted in symptom scores in 68% and NK function in 75% of patients studied, as compared to 0% for both symptom score and NK function in the control group taking the TF preparation without HHV-6.
PROTOCOL. Transfer factor may be given in oral or injectable form. It may take at least six months before improvement is noted.
PROS AND CONS. Because transfer factor has not been widely tested as a treatment for CFS/ME, it is difficult to assess its efficacy. It is worth noting that when transfer factor is effective, the results are global, with significant improvement of symptoms.
In his book, The Type I/Type 2 Allergy Relief Program, Dr. Alan Levin wrote of his extensive experience with transfer factor. After using it to treat severe allergic conditions in more than 300 patients, he reported a 68% success rate, with miraculous results in some patients. However, he pointed out some serious side effects, including heart or muscle malfunction, temporary or permanent brain damage, and aggravated vasculitis, and recommended that transfer factor should probably be used only in patients with incapacitating symptoms.
Other physicians have not shared Dr. Levin's success rate and a number of CFS/ME patients have reported not only lack of improvement but even a worsening of allergic-type symptoms, even after lengthy treatments with transfer factor. In fact, treatment surveys conducted by De Paul University and independent researchers have shown that about a third of those who try transfer factor consider it "harmful." Side effects of treatment may vary. Dr. Pizza notes that fatigue, sore throat, fever, and headache may occur within the first few days of treatment, but these resolve quickly. These side effects might be the result of immune system activation in response to transfer factor.
Few CFS/ME doctors currently use transfer factor, so it is difficult to assess its usefulness as a treatment. Dr. Cheney has used transfer factor, but to our knowledge, there are no other CFS/ME protocols that include transfer factor.
AVAILABILITY AND COST. Oral transfer factor is available through a number of online sources. ProHealth sells Transfer Factor Essentials for $40 a bottle. Chisolm Biological Laboratory's ImmunFactor formulations cost $140 for a bottle of 30 gel caps.
FURTHER READING
Sloan Kettering's excellent review of transfer factor: http://www.mskcc.org/cancer-care/herb/transfer-factor
Patient thread discussing transfer factor: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=1374195
MORE INFORMATION
Ordering information for transfer factor multi-immune: http://www.forresthealth.com/_search.php?page=1&q=transfer+factor&x=0&y=0
Ordering information for Chisolm Labs transfer factor: http://www.forresthealth.com/chisolm-biological-laboratories/
RESEARCH
Brewer, Joseph. “Administration of Transfer Factor for Human Herpesvirus 6 (HHV-6) in Patients with Chronic Fatigue Syndrome and HHV-6 Viremia.” HHV6 News. http://hhv6.blogspot.com/2005/07/joseph-brewer-on-hhv-6-transfer-factor.html
De Vinci, C, Levine, PH, Pizza, G, Fudenberg, HH, Orens, P, Pearson, G, Viza, D. “Lessons from a pilot study of transfer factor in chronic fatigue syndrome.” Biotherapy. 1996;9(1-3):87-90. http://www.ncbi.nlm.nih.gov/pubmed/8993764 (Abstract)
CHAPTER 5: NUTRITIONAL SUPPLEMENTS AND BOTANICALS
INTRODUCTION
This section encompasses nutritional supplements, botanicals (herbs), and compounds that are naturally found in the body. Although some of these are also classed as pharmaceuticals, nearly everything in this section can be purchased without a prescription. (The exception is injectables.) We have not included each and every supplement that is available on the market, but have limited our selection to those for which there is relevant medical research, or which are in common use either by CFS/ME clinicians or by CFS/ME patients themselves.
Nutritional supplements are an essential component of any CFS/ME treatment protocol. Research has shown that people with CFS/ME are routinely deficient in many important nutrients (notably zinc, magnesium, and carnitine). These deficiencies, in and of themselves, can decrease the degree to which the body can absorb and make use of other nutrients. Even when there are no clinical nutritional deficiencies, the physiological demands of a chronic illness make it necessary to provide additional nutritional support – especially in light of the numerous GI problems prevalent in the CFS/ME population, which may lead to malabsorption. For these reasons, and because most CFS/ME doctors recommend supplements, this section attempts to be as inclusive as possible.
There is a method to taking nutritional supplements. As with pharmaceuticals, supplements should initially be taken in very small doses to test for sensitivity. Even if a supplement consists of something “natural” there is nothing natural about taking it in concentrated doses. Your body reacts to these as it would to any chemical. For that reason, it is wise to take supplements with food, unless instructed otherwise.
“Take with food” means eat a little first, then take the supplement, then eat some more. By sandwiching the supplement within a meal, you lower the risk of reactions, as the supplement is processed along with food. Sandwiching supplements also reduces the risk of heartburn. When a supplement is taken with water only it floats to the top of the stomach, where it can easily flow back into the esophagus, causing irritation.
New supplements should be taken one at a time. That is, don't start several supplements at once, even if they act synergistically. Take the new supplement for three or four days before introducing another. This allows you to evaluate the supplements for possible negative reactions or sensitivities.
Supplements can be quite expensive and are not usually covered by health insurance. But purchasing the cheapest brand is not always the wisest course to take. There is a wide range in quality when it comes to nutritional supplements. Some of the cheapest brands may not even contain the ingredients on the label. It is best to stick to well-known brands and to purchase from reputable suppliers. (See Appendix D: Mail Order Suppliers.) Purchasing online, rather than from retail outlets can cut the cost of expensive supplements in half. Whenever possible, we have included recommendations in each entry.
Most online suppliers include product label information on their websites, but for those who wish to compare the product labels of a supplement made by different manufacturers, or check into recalls or FDA notices for specific supplements, there are several helpful websites that will provide this information:
The Dietary Supplements Labels Database. This is a very useful website that allows searches for product labels by manufacturer and by product. From the website: “The Dietary Supplements Labels Database offers information about label ingredients in more than 6,000 selected brands of dietary supplements. It enables users to compare label ingredients in different brands. Information is also provided on the "structure/function" claims made by manufacturers.” http://dietarysupplements.nlm.nih.gov/dietary/index.jsp
Natural Products Foundation. The NPF keeps an excellent database of supplements, as well as the medical conditions they are used for. From the website: “The Dietary Supplement Information Bureau™ (DSIB™) was founded in 2001 to promote the responsible use of vitamins, minerals, herbs and specialty supplements. In June 2008 DSIB became part of the Natural Products Foundation, a not-for-profit organization whose mission is to promote and facilitate research and education related to natural products for the benefit of consumers and industry.” http://www.naturalproductsinfo.org/
Consumer Healthcare Products Association. The CHPA website provides a search for government warnings and decisions regarding most OTC medications and supplements. From the website: “The Consumer Healthcare Products Association (CHPA), founded in 1881, is a member-based association representing the leading manufacturers and distributors of nonprescription, over-the-counter (OTC) medicines and dietary supplements.” http://www.chpa-info.org/
FURTHER READING
Dowson, David, MD. “Nutrition Toxicity and ME/CFS.” http://www.annhilltrust.org/nutrition-toxicity-and-me.html
5-HTP
DESCRIPTION. 5-Hydroxytryphophan (5-HTP) is a naturally occurring amino acid which serves as a precursor to the neurotransmitter serotonin.
BACKGROUND. 5-HTP is a precursor as well as a metabolic intermediate in the synthesis of serotonin and melatonin from tryptophan. Through the action of vitamin B6, 5-HTP is converted in the liver and nervous system to 5-HP (serotonin). Most commercially marketed 5-HTP is derived from the seeds of the Griffonia simplicifolia. a woody climbing shrub native to West Africa.
Serotonin is the most abundant neurotransmitter in the human body. In the brain it plays a crucial role in sleep, mood, learning, memory and appetite. However, the vast majority of serotonin, 90%, is produced in the lining of the intestines, which has led Dr. Michael Gershon, chairman of the department of anatomy and cell biology at Columbia University, to refer to the gut as the “second brain.” This eponym is apt, for today gastroenterologists routinely prescribe serotonin enhancers for treating GI motility problems.
USES IN CFS/ME. Several studies have shown that 5-HTP is an effective overall treatment for fibromyalgia. For people with CFS/ME, 5-HTP is most often used as a sleep aid.
PROTOCOL. Dr. Rodger Murphree, a chiropractor and nutritionist who has been treating CFS/ME for over 15 years, recommends taking 5-HTP 30 minutes before bed, on an empty stomach, with four ounces of juice. Start with 100 mg, then go to 150 and then to 200. Don’t go above 300 mg. It may take several nights to take effect. If it doesn’t work in two weeks, Dr. Murphree suggests stopping and switching to melatonin. According to Dr. Murphree, patients who stay on 5-HTP for more than three months should take a broad-based amino acid supplement to balance out the other neurotransmitters.
PROS AND CONS. 5-HTP, like many antidepressants, can cause strange, vivid dreams. These dreams usually diminish over time. Excessively high serotonin levels can cause insomnia, hyperactivity, headache, and increased heart rate. CFS/ME patients who have a negative reaction to 5-HTP should either lower the dose or stop.
AVAILABILITY AND COST. 5 HTP is sold in most health food stores and by online distributors. A bottle of 60 tablets can cost as little as $8.00.
CAUTION: High doses of 5-HTP can cause serotonin syndrome, a condition in which serotonin is raised to dangerous levels. Taking 5-HTP with serotonin-enhancing pharmaceuticals such as triptans (for migraines), antidepressants, Demerol, Robitussin, and Ultram can also lead to serotonin syndrome.
FURTHER READING
Good summary of 5-HTP as a CFS/ME treatment: http://www.immunesupport.com/98wtr002.htm
Discussion of 5-HTP as a CFS/ME treatment: http://aboutmecfs.org.violet.arvixe.com/Trt/5-HTP.aspx
Dr. Teitelbaum on 5-HTP and other natural sleep aids: http://www.healthy.net/scr/Column.aspx?Id=647
General information on 5-HTP: http://www.herbwisdom.com/herb-5-htp.html
PATIENT REVIEWS
CFS/ME patient reviews of 5-HTP: http://www.revolutionhealth.com/drugs-treatments/rating/5-htp-5-hydroxytryptophan-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Caruso I, Sarzi Puttini P, Cazzola M, Azzolini V. “Double-blind study of 5-hydroxytryptophan versus placebo in the treatment of primary fibromyalgia syndrome.” J Int Med Res. 1990 May-Jun;18(3):201-9. http://www.ncbi.nlm.nih.gov/pubmed/2193835 (Abstract)
Sarzi Puttini P, Caruso I, “Primary fibromyalgia syndrome and 5-hydroxy-L-tryptophan: a 90-day open study.” J Int Med Res.1992 Apr;20(2):182-9. http://www.ncbi.nlm.nih.gov/pubmed/1521674 (Abstract)
ALPHA KETOGLUTARATE
DESCRIPTION. Alpha ketoglutarate (AKG) is an ionic form of alpha ketoglutarate acid, an intermediate in the tricarboxylic cycle (Krebs cycle, or citric acid cycle).
BACKGROUND. Alpha ketoglutarate (AKG) fulfills a vital role in the metabolism and utilization of carbohydrates, proteins, and long-chain fatty acids. Its best known function is as a component of a number of energy-producing cycles at the cellular level. The first of these, the Krebs cycle, breaks down and transforms citric acid through a series of enzyme-controlled reactions to produce adenosine triphosphate (ATP), a crucial energy source for many cell processes. AKG, as an early intermediate in the Krebs cycle, forms the basis for all further transformations. It is also required for catabolism of many amino acids, another process that generates energy.
Another important function of AKG involves the formation of nonessential amino acids (amino acids that are biosynthesized in the body), notably glutamate and, through its action, proline, alanine, aspartic acid, and asparagine. AKG is also one of the most important transporters of cellular nitrogen, combining with nitrogen in the cell to prevent an overload of ammonia in the body.
USES IN CFS/ME. AKG is used as a short-term energy enhancer and for Krebs cycle support in patients with CFS/ME. Because of its essential role in energy production and carbohydrate metabolism, it may be useful as a general CFS/ME treatment as well. AKG is also beneficial for the intestines. Many people with CFS/ME suffer from digestive problems, including food sensitivities, dysbiosis, slow transit time, small intestine bacterial overgrowth (SIBO) and a host of other disorders. AKG is converted in the intestines into glutamate, which regulates gastric emptying and provides an environment for healthy gut flora. AKG also prevents damage to the mucosal lining of the intestines by inhibiting oxidative stress.
PROTOCOL. The suggested dosage of AKG is one or two 300 mg capsules per day, which can be taken with meals. Because of its location in the Krebs cycle, alpha ketoglutarate is generally more effective if taken with other Krebs cycle supports such as vitamin C, B vitamins, essential fatty acids (evening primrose oil, borage oil, or fish oil), magnesium, nutritional supplements, and NAC (N-acetyl-L-cysteine).
PROS. Because alpha ketoglutarate is not a stimulant but works through natural metabolic pathways, it is a relatively risk-free source of energy. People who take alpha ketoglutarate usually do not "crash" afterward. It has no reported side effects at recommended doses. Patients with low levels of AKG (as confirmed by an Organic Acids Test) have noted significant improvement in energy levels with alpha ketoglutarate supplementation.
CONS. Results tend to be less dramatic than those obtained with CoQ10, which may make this product less attractive to those who want a greater boost. Among its many function, AKG leads to production of nitric oxide (NO), which Dr. Pall has implicated in many CFS/ME symptoms. He has recommended that NO should be down regulated in people with CFS/ME. Because AKG is normally combined with excitatory amino acids, it can cause insomnia.
AVAILABILITY AND COST. Pure AKG is difficult to find. Most suppliers combine AKG with an amino acid, such as arginine or glutamine. Douglas Labs sells a 90-tablet bottle of AKG (300 mg) combined with vitamin B6, calcium and phosphorus for $18.
FURTHER READING
Benefits of AKG and its functions in the Krebs cycle: http://www.ei-resource.org/articles/general-environmental-health-articles/influencing-your-krebs-cycle/
A detailed description of Krebs cycle intermediaries, including AKG. Very technical. http://www.nutritionreview.org/library/krebs.php
RESEARCH
Hou Y, Wang L, Ding B, Liu Y, Zhu H, Liu J, Li Y, Kang P, Yin Y, Wu G. “Alpha-Ketoglutarate and intestinal function.” Front Biosci. 2011 Jan 1;16:1186-96. http://www.ncbi.nlm.nih.gov/pubmed/21196226 (Abstract)
ALPHA LIPOIC ACID
DESCRIPTION. Alpha lipoic acid, or lipoic acid, is a an organic compound derived from caprylic acid. It is both fat and water soluble.
BACKGROUND. Alpha lipoic acid (ALA) has been referred to as the “mother” of all antioxidants. This well-deserved epithet is due to the fact that not only does it act as a potent free radical scavenger, it can transform an oxidant into an antioxidant. Notably, when glutathione is oxidized, ALA can transform it back into its reduced form, thus increasing the pool of glutathione.
ALA is produced throughout the body through the biosynthesis of fatty acids. Although it is found in many foods (especially organ meats, yeast extract and leafy green vegetables), alpha lipoic acid is not readily available through dietary sources. As a consequence, all alpha lipoic acid supplements must be synthesized.
Alpha lipoic acid has been studied for its effects on many disease states, including treatment for cardiovascular disease, prevention of migraines, preventing organ dysfunction, slowing the progression of Alzheimer's disease, reducing inflammation, and the treatment of chronic diseases involving oxidative stress. A study conducted in 1999 by Kishi et al found that the reduced glucose uptake in diabetes was completely reversed with alpha lipoic acid, which not only corrected the deficit, but improved the peripheral neuropathy found in diabetics.
A detailed proposal submitted to the National Cancer Institute by the Chemical Selection Working Group (see below) indicates that ALA may work best when combined with acetyl L-carnitine. Acetyl-L-carnitine facilitates the movement of fatty acids into the mitochondria for energy and is also used to generate acetyl coenzyme A, while ALA is involved in mitochondrial ATP production and can recycle other antioxidants. The authors propose that the combination of acetyl L-carnitine and ALA may have significant synergistic effects – increasing energy and reducing oxidative stress.
USES IN CFS/ME. A number of CFS/ME clinicians and researchers, notably Martin Pall and Dr. Myhill, have pointed out that oxidative stress is a primary component in the cascade of CFS/ME symptoms. Oxidative stress can affect every system in the body, and has particularly deleterious effects on oxygen transport systems (blood). ALA has been shown to improve the integrity of red blood cells (which are often abnormal in CFS/ME patients) leading to elevated glutathione levels. Glutathione, one of the body's most potent antioxidants, is often diminished in CFS/ME patients.
PROTOCOL. The “R” form is the most bioavailable and stable form of alpha lipoic acid. (The “S” form deteriorates rapidly.) There is no set protocol for ALA. CFS/ME patients who have tried ALA recommend beginning at the lowest dose (100 mg) to avoid detox symptoms (headache, “hungover” feeling).
PROS. ALA has no documented side effects at low doses. Many people have noted an increase in energy, muscle strength, and mental alertness, particularly when taken with acetyl-L carnitine.
CONS. Too high a dose can cause insomnia and stomach upset. ALA lowers blood sugar, which may pose a problem for people with hypoglycemia. There is one study that suggests that ALA competes with biotin (vitamin B7) in rats, but the results have not been confirmed in humans. Those who take large quantities of lipoic acid may wish to independently supplement with biotin.
AVAILABILITY AND COST. ALA is widely available in health food stores and through online distributors. It is not expensive. A 60-capsule bottle of R-ALA (100 mg) can cost less than $10.
FURTHER READING
This article questions the necessity of supplementing lipoic acid with biotin. http://www.geronova.com/content/lipoic-acid-biotin
RESEARCH
Kishi, Yutaka, James D. Schmelzer, Jeffrey K. Yao, Paula J. Zollman, Kim K. Nickander, Hans J. Tritschler, and Phillip A. Low. “ a-Lipoic Acid: Effect on Glucose Uptake, Sorbitol P a t h w a y, and Energy Metabolism in Experimental Diabetic Neuropathy.” Diabetes, VOL. 48, October 1999 http://diabetes.diabetesjournals.org/content/48/10/2045.full.pdf
Mirjana M, Jelena A, Aleksandra U, Svetlana D, Nevena G, Jelena M, Goran P, Melita V. “Alpha-lipoic acid preserves the structural and functional integrity of
red blood cells by adjusting the redox disturbance and decreasing O-GlcNAc modifications of antioxidant enzymes and heat shock proteins in diabetic rats.” Eur J Nutr. 2011 Nov 18. http://www.ncbi.nlm.nih.gov/pubmed/22094580 (Abstract)
“Acetyl-L-Carnitine/a-Lipoic Acid Supplements.” This is a proposal prepared for the National Cancer Institute by the Chemical Selection Working Group (CSWG) on behalf of Technical Resources International, Inc. It contains a thorough and exhaustive account of the mechanisms of alpha lipoic acid. http://ntp.niehs.nih.gov/ntp/htdocs/chem_background/exsumpdf/carnliposupp.pdf
AMINO ACIDS
Carnitine, Glutamine, Lysine, Taurine
DESCRIPTION. Amino acids are nitrogen-containing chemical units (amines) that, bound together, make up protein.
BACKGROUND. The amino acids, in various combinations, form the hundreds of types of proteins present in every living organism. These proteins are essential for nearly all processes that induce cell growth and repair, as well as for continued maintenance of every body tissue, organ, and structure within the body. Amino acids link together to form tens of thousands of proteins and enzymes, each of which has a specific function. They can also perform as individual units. Single amino acids can act as neurotransmitters or as precursors to neurotransmitters in the central nervous system. Therefore, not only are they responsible for providing and maintaining the very substances of which we are made, but also for the communications system that enables us to plan, dream, think, feel, and direct our every action.
There are 20 primary amino acids. About 80% are produced in the liver and the remaining 20% must be obtained from food. Whether an amino acid can be produced within the body is what distinguishes the essential from nonessential amino acids. The essential amino acids (those which must be obtained from food sources) are arginine, histidine, isoleucine, leucine, lysine, methionine, phenylalanine, threonine, tryptophan, and valine. Nonessential amino acids (those which can be produced within the body) include alanine, glutamine, asparagine, glycine, proline, and serine. Given the countless functions that amino acids perform, a protein shortage or congenital defect in amino acid synthesis can lead to problems that involve every system in the body.
Amino acids occur in two isomers: L and D. The L isomer is the form most commonly found in nutritional supplements.
USES IN CFS/ME. Specific amino acids, both essential and nonessential, have been recommended as treatments by a number of CFS/ME clinicians. Their applications include mediation of hyperactive nervous system responses, repair of leaky gut and other intestinal disturbances, and regulation of the fundamental CFS/ME metabolic dysfunction that results in loss of cellular energy.
A number of researchers have documented imbalances in amino acid ratios among people with CFS/ME. In an article published in 1994, Dr. Alexander Bralley and Dr. Richard Lord noted that people with CFS/ME commonly have deficiencies in tryptophan, phenylalanine, taurine, isoleucine, and leucine. They also found lower than normal amounts of arginine, methionine, lysine, threonine, and valine in a smaller number of CFS/ME patients. It is significant that the most common deficiencies found by Drs. Bralley and Lord are of phenylalanine and tryptophan because these two amino acids are precursors to the catecholamines and serotonin, neurotransmitters that are closely involved with sleep function, stress responses, and regulation of pain and mood.
Dr. Scott Rigden has also noted that many of his patients with metabolic abnormalities have an imbalance in amino acid ratios. The implication is that, for these patients, amino acids may be either synthesized or utilized at a slower rate or appear in such disequilibrium that they no longer function together with full efficiency – perhaps giving a clue to the origins of the collagen formation problems and enzyme disturbances common in many patients with CFS/ME.
An extensive study published in 2005 by Jones et al compared organic acids in people with CFS/ME, major depression, and rheumatoid arthritis. The researchers found lower levels of taurine, GABA, histidine and tyrosine in the group with CFS/ME. The researchers also found low levels of histidine in plasma from rheumatoid arthritis patients, leading the team to speculate that a similar etiology might be involved for the two illnesses (i.e. inflammation).
A more recent study by Niblett et al confirms specific deficiencies in CFS/ME patients of asparagine, phenylalanine, leucine, isoleucine, valine, and the organic acid, succinic acid, as well as increases in 3-methylhistidine (an amino acid associated with protein loss) and tyrosine. The authors concluded that “urinary excretion and blood parameters data supported the hypothesis that alterations in physiologic homeostasis exist in CFS patients.”
In 2012 a team of Australian researchers identified low levels of glutamine and ornithine, along with other metabolites that participate in the urea cycle, in a group of CFS/ME patients. (CFS/ME patients are consistently low in uric acid.) The researchers suggested that a specific disturbance of amino acid and nitrogen metabolism was implicated in CFS/ME which might potentially serve as a biomarker.
Amino acid supplementation has received particular attention as a treatment for CFS/ME from nutritionists. Using an amino acid analyzer to measure specific imbalances, Drs. Bralley and Lord tailored a supplement to correct amino acid deficiencies. In a study of 25 CFS/ME patients, they found that correcting specific amino acid imbalances resulted in 50% to 100% improvement in symptoms (Journal of Applied Nutrition, 1994). The greatest effect was noted in energy levels. Two patients who had had CFS/ME symptoms for 15 years experienced dramatic improvement. Patients also reported improvement in cognitive function and elimination of "brain fog."
It should be noted that single amino acids taken as dietary supplements may not be well tolerated by patients with serious metabolic disturbances. Also note that tyrosine, an amino acid often found to be deficient in CFS/ME patients, is seldom recommended. Tyrosine is a dopamine precursor which triggers symptoms in patients with inflammatory disorders such as migraine, interstitial cystitis, and rosacea. Dr. Bell has observed that in CFS/ME patients, dopamine precursors make the majority of CFS/ME patients feel much worse.
FURTHER READING
Bralley J., Alexander and Richard S. Lord. “Treatment of Chronic Fatigue Syndrome with Specific Amino Acid Supplementation.” Journal of Applied Nutrition, Vol 46, No 3, 1994. http://www.metametrix.com/files/learning-center/articles/Chronic-Fatigue-Amino-Acids.pdf
Dr. Michael Rosenberg's amino acid protocols for treating CFS/ME. http://www.prohealth.com/library/showarticle.cfm?id=4337&t=CFS/ME_FM
RESEARCH
Armstrong, Christopher W., Neil R. McGregor, John R. Sheedy, Ian Buttfield, Henry L. Butt, Paul R. Gooley. “NMR metabolic profiling of serum identifies amino acid disturbances in Chronic Fatigue Syndrome.” Clinica Chimica Acta. Available online 21 June 2012. http://www.sciencedirect.com/science/article/pii/S0009898112003270
Jones, Mark G., Elizabeth Cooper, Saira Amjad, Stewart C. Goodwin, Jeffrey L. Barron, Ronald A. Chalmers. “Urinary and plasma organic acids and amino acids in chronic fatigue syndrome.” Clin Chim Acta. 2005 Nov;361(1-2):150-8. http://www.cfids-cab.org/cfs-inform/Hypotheses/jones.etal.05.pdf
Niblett SH, King KE, Dunstan RH, Clifton-Bligh P, Hoskin LA, Roberts TK, Fulcher GR, McGregor NR, Dunsmore JC, Butt HL, Klineberg I, Rothkirch TB. “Hematologic and urinary excretion anomalies in patients with chronic fatigue syndrome.” Exp Biol Med (Maywood). 2007 Sep;232(8):1041-9. http://www.ncbi.nlm.nih.gov/pubmed/17720950 (Abstract)
CARNITINE
DESCRIPTION. Carnitine (L-carnitine) is one of the methyl group donors. It is crucial for the transport of long-chain fatty acids into the mitochondria of cells, providing energy to skeletal and heart muscle. Carnitine also aids in reducing toxic buildup of organic acids which are a natural byproduct of cell metabolism. Carnitine deficiency produces fatigue, muscle weakness, malaise, exercise intolerance, heartbeat abnormalities, and tissue acidosis. Carnitine deficiency can result from congenital metabolic defects as well as the administration of antibiotics containing pivalic acid (e.g., Pondocillin).
USES IN CFS/ME. Japanese researchers have shown that CFS/ME patients have a deficiency in intracellular levels of acylcarnitine. They found no deficiency in serum levels of free carnitine, however, indicating the deficiency is not the result of lack of carnitine in the system but of its derivative, acylcarnitine. Acylcarnitine deficiency can be expected to produce not only the fatigue and weakness characteristic of interruption in mitochondrial processes but also the malaise typical of autointoxication. Dr. Hiroko Kuratsune and colleagues discovered that in their sample group of 38 CFS/ME patients, low levels of acylcarnitine covaried with the severity of the illness (Clinical Infectious Diseases, 1994). As symptoms improved, so did acylcarnitine levels. In a study comparing amantadine and carnitine, Dr. Audrius Plioplys and Dr. Sigita Plioplys found "statistically significant clinical improvement" after eight weeks of treatment with L-carnitine (Neuropsychobiology, 1997).
A subsequent study in 2004 by Okada et al, found secondary proof for acetyl-carnitine deficiency in CFS/ME patients. Using MRI imaging, they found that there was a reduction in gray matter in the prefrontal cortex of CFS/ME patients as compared to controls. The researchers concluded that their results were “consistent with previous reports of an abnormal distribution of acetyl-L-carnitine uptake, which is one of the biochemical markers of chronic fatigue syndrome, in the prefrontal cortex. Thus, the prefrontal cortex might be an important element of the neural system that regulates sensations of fatigue.”
In a recent study conducted in 2011, researchers from the University of South Australia compared L-carnitine levels of 44 CFS/ME patients to 49 controls. They found that levels of acylcarnitine was 30-40% lower in CFS/ME patients. The authors hypothesized that the administration of omega-3 fatty acids in combination with L-carnitine would improve chronic fatigue syndrome symptomology.
PROTOCOL. Carnitine can be taken in liquid or pill form as an over-the-counter nutritional supplement. As a food supplement, the general recommended dosage is 1000 mg/day taken with a meal. The liquid is often better tolerated than the pill form although patients with chemical sensitivities should note that the liquid may also contain artificial flavors, colors, preservatives (methylparaben), and sucrose.
Dr. Teitelbaum has observed that in his experience acetyl-L-carnitine is much more effective that L-carnitine. This is due to the fact that acetyl-L-carnitine crosses the blood-brain barrier, as opposed to L-carnitine, which is too rapidly excreted by the kidneys to be adequately utilized by the brain. Dr. Teitelbaum recommends taking 500 mg of pure acetyl-L-carnitine 2-3 times a day. In low doses, acetyl-L-carnitine can mimic the effects of pyridostigmine and galantamine, increasing the availability of acetylcholine in both the peripheral and central nervous systems.
Because carnitine interferes with thyroid hormone production, thyroid levels (free T3 and T4, as well as TSH) should be taken before beginning supplementation. Even if thyroid hormone levels fall within the normal range, carnitine should not be taken for more than a month. Signs of thyroid suppression are dry skin, low energy level, weight gain, excessive sleep, and hormonal disturbances.
PROS. L-Carnitine as a food supplement is widely available. Patients have reported increased muscle function, decreased weakness, and overall improved stamina and well-being after a few weeks of carnitine supplementation. In some cases, the benefits remain even after finishing the course of treatment.
CONS. Carnitine is not recommended for patients with low thyroid function, as it interferes with thyroid hormones. Excess amounts of carnitine can cause diarrhea and stomach upset, so start with low doses.
AVAILABILITY AND COST. A 12 oz bottle of the liquid nutritional supplement Mega L -Carnitine (Twin Labs) can be purchased online at Vitacost for $10. At the recommended dosage of 1 tablespoon a day, the bottle will last for 1 month. A 30-capsule bottle of acetyl-L-carnitine costs around $18. (There are many brands. Check Vitacost for a cost comparison.)
FURTHER READING
Dr. Teitelbaum's carnitine protocol: http://www.endfatigue.com/health_articles_c/CFS_FM-acetyl-l-carnitine_for_cfs.html
RESEARCH
Benvenga S, Amato A, Calvani M, Trimarchi F. “Effects of carnitine on thyroid hormone action.” Ann NY Acad Sci. 2004 Nov;1033:158-67. http://www.ncbi.nlm.nih.gov/pubmed/15591013 (Abstract)
Colucci S, Mori G, Vaira S, Brunetti G, Greco G, Mancini L, Simone GM, Sardelli F, Koverech A, Zallone A, Grano M. “L-carnitine and isovaleryl L-carnitine fumarate positively affect human osteoblast proliferation and differentiation in vitro.” Calcif Tissue Int. 2005 Jun;76(6):458-65. http://www.ncbi.nlm.nih.gov/pubmed/15906015 (Abstract)
Eder K, Felgner J, Becker K, Kluge H. “Free and total carnitine concentrations in pig plasma after oral ingestion of various L-carnitine compounds.” Int J Vitam Nutr Res. 2005 Jan;75(1):3-9. http://www.ncbi.nlm.nih.gov/pubmed/15830915 (Abstract)
Ho JY, Kraemer WJ, Volek JS, Fragala MS, Thomas GA, Dunn-Lewis C, Coday M. Häkkinen K, Maresh CM. “L-Carnitine l-tartrate supplementation favorably affects biochemical markers of recovery from physical exertion in middle-aged men and women.” Metabolism. 2010 Aug;59(8):1190-9. http://www.ncbi.nlm.nih.gov/pubmed/20045157 (Abstract)
Holme, Elisabeth, Carl-Eric Jacobson, Ingalill Nordin, Joachim Greter, Sven Lindstedt, Bengt Kristiansson, Ulf Jodal. “Carnitine Deficiency Induced by Pivampicilin and Pivmecillinam Therapy.” The Lancet. Volume 334, Issue 8661, Pages 469 - 473, 26 August 1989. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(89)92086-2/abstract (Abstract)
Kuratsune H, Yamaguti K, Takahashi M, Misaki H, Tagawa S, Kitani T. “Acylcarnitine deficiency in chronic fatigue syndrome.” Clin Infect Dis. 1994 Jan;18 Suppl 1:S62-7. http://www.ncbi.nlm.nih.gov/pubmed/8148455 (Abstract)
Okada T, Tanaka M, Kuratsune H, Watanabe Y, Sadato N. “Mechanisms underlying fatigue: a voxel-based morphometric study of chronic fatigue syndrome.” BMC Neurol. 2004 Oct 4;4(1):14. http://www.ncbi.nlm.nih.gov/pubmed/15461817 (Abstract)
Patano N, Mancini L, Settanni MP, Strippoli M, Brunetti G, Greco G, Tamma R, Vergari R, Sardelli F, Koverech A, Colucci S, Zallone A, Grano M. “L-carnitine fumarate and isovaleryl-L: -carnitine fumarate accelerate the recovery of bone volume/total volume ratio after experimentally induced osteoporosis in pregnant mice.” Calcif Tissue Int. 2008 Mar;82(3):221-8. http://www.ncbi.nlm.nih.gov/pubmed/18265928 (Abstract)
Plioplys AV, Plioplys S. “Amantadine and L-carnitine treatment of Chronic Fatigue Syndrome.” Neuropsychobiology. 1997;35(1):16-23. http://www.ncbi.nlm.nih.gov/pubmed/9018019 (Abstract)
Reuter SE, Evans AM. “Long-chain acylcarnitine deficiency in patients with chronic fatigue syndrome. Potential involvement of altered carnitinepalmitoyltransferase-I activity.” J Intern Med. 2011 Jul;270(1):76-84. http://www.ncbi.nlm.nih.gov/pubmed/21205027 (Abstract)
Spiering BA, Kraemer WJ, Vingren JL, Hatfield DL, Fragala MS, Ho JY, Maresh CM, Anderson JM, Volek JS. “Responses of criterion variables to different supplemental doses of L-carnitine L-tartrate.” Journal of Strength and Conditioning Research. 2007 Feb;21(1):259-64. http://www.ncbi.nlm.nih.gov/pubmed/17313301 (Abstract)
Vermeulen RC, Scholte HR. “Exploratory open label, randomized study of acetyl- and propionylcarnitine in chronic fatigue syndrome.” Psychosom Med. 2004 Mar-Apr;66(2):276-82. http://www.ncbi.nlm.nih.gov/pubmed/15039515 (Abstract)
GLUTAMINE
DESCRIPTION. Glutamine is the most abundant nonessential amino acid in the body. It is a precursor to glutathione.
BACKGROUND. Glutamine plays an important role in many biological functions, including protein synthesis, providing cellular energy, and as a non-toxic transporter of ammonia in the bloodstream. When converted to glutamic acid, it acts as an excitatory neurotransmitter in the brain.
In the intestinal tract, glutamine strengthens the gut's function as an immune barrier by supporting the production of secretory immunoglobulin A (sIgA), which helps maintain the structure, metabolism, and function of the mucosal lining of the intestines. Glutamine can help heal injured gut mucosa after surgery and, in a high percentage (92%) of patients, completely heals ulcer damage. Glutamine is an important detoxifying agent for ammonia, a neurotoxin and one of the toxic by-products of protein metabolism. It is used to treat sugar craving, fatigue, ADHD, peptic ulcers, and personality disorders. Dietary sources of glutamine include beef, chicken, fish, eggs, milk, dairy products, wheat, cabbage, beets, beans, and spinach.
USES IN CFS/ME. Because it is so important in gastrointestinal growth and function, glutamine is primarily used to treat leaky gut. Clinicians recommend taking 1000 mg of glutamine daily on an empty stomach, divided into equal doses (Patients with many sensitivities may want to test a very small amount of this amino acid before taking the full dose.)
PROS. A number of CFS/ME patients have noted improvement in gut function and increased food tolerance with this treatment as well as a decrease in “brain fog.” Side effects from this amino acid are relatively rare (but see below).
CONS. L-glutamine can cause gastrointestinal symptoms such as nausea and diarrhea. In patients with small intestinal bacterial overgrowth (SIBO) glutamine may actually worsen symptoms. Because glutamine is an excitatory neurotransmitter it may cause insomnia in individuals who do not tolerate stimulants. People who are sensitive to MSG should not take glutamine.
AVAILABILITY AND COST. Glutamine is available at health food stores and online in both powder and pill form. It is inexpensive. A 100-tablet bottle can cost as little as $6. Glutamine is also available from some compounding pharmacies as enteric coated tablets which are formulated to bypass the stomach and increase bioavailability.
RESEARCH
Blachier, François, Claire Boutry, Cécile Bos, Daniel Tomé. “Metabolism and functions of L-glutamate in the epithelial cells of the small and large intestines.” Am J Clin Nutr September 2009 vol. 90 no. 3 814S-821S. http://www.ajcn.org/content/90/3/814S.abstract
LYSINE
DESCRIPTION. Lysine is an essential amino acid. (It cannot be synthesized in the body.)
BACKGROUND. Lysine is needed for bone growth in children and to maintain nitrogen balance in adults. It also aids in the production of antibodies, hormones, and enzymes as well as helping in collagen formation, muscle building, and tissue repair. Lysine deficiency can result in hair loss, anemia, bloodshot eyes, loss of energy, and irritability. Food sources of lysine include meat, eggs, legumes and milk.
USES IN CFS/ME. Lysine is recommended chiefly because of its ability to inhibit reproduction of herpesviruses (herpes simplex virus, varicella zoster virus, human herpesvirus 6, and Epstein-Barr virus), which require arginine in order to reproduce. Lysine's structure is similar enough to arginine, however, that herpesviruses can be fooled into using lysine instead. Since the virus cannot use lysine for replication, the virus loses its ability to reproduce, effectively halting the spread of the infection. Some CFS/ME doctors recommend lysine to treat frequent outbreaks of cold sores (herpes simplex) or shingles (herpes zoster).
PROTOCOL. Dr. Charles Lapp recommends 1000 to 2000 mg of lysine, taken daily with meals. Foods high in arginine, such as chocolate, nuts, raisins, whole wheat, cereal, and brown rice, should be avoided.
PROS. Lysine appears to be a safe, effective treatment for cold sores.
CONS. Side effects of lysine can include dizziness, sweating, nausea, appetite loss, and difficulty swallowing. Lysine should be discontinued if these symptoms develop.
AVAILABILITY AND COST. Lysine is available in most health food stores and can be purchased inexpensively. Most brands retail for less than $10 for a 100-capsule bottle (500 mg).
RESEARCH
Griffith RS, Walsh DE, Myrmel KH, Thompson RW, Behforooz A. “Success of L-lysine therapy in frequently recurrent herpes simplex infection. Treatment and prophylaxis.” Dermatologica 1987;175(4):183-90. http://www.ncbi.nlm.nih.gov/pubmed/3115841 (Abstract)
TAURINE
DESCRIPTION. Although taurine is usually classified as an amino acid, it is actually an organic acid, which is an organic compound with acidic properties but without a carboxyl group.
BACKGROUND. Taurine acts as a building block for all other amino acids and consequently is present in every cell in the body. It is a prime component of bile (thus aiding in fat digestion and vitamin absorption) and is found in high concentrations in heart muscle, skeletal muscle, white blood cells, and the central nervous system (CNS). Anxiety, hyperactivity, and poor brain function are related to taurine deficiency. Taurine can be synthesized in the body from cysteine, with the aid of vitamin B6.
Taurine is unusual in that it not only functions as a neurotransmitter, but as a potent antioxidant. When taurine interacts with the oxidant hypochlorous acid it forms taurine monochloramine, which inhibits the transcription iNOS gene as well as the expression of COX-2 protein, both of which are primary sources of inflammation. Taurine lowers NF-kappaB activity, which helps inhibit another important inflammatory pathway. It also acts to reduce intracellular calcium levels, thus lowering the production of nitric oxide. In its role as a neuromodulator, taurine stimulates the synthesis of GABA, the primary inhibitory neurotransmitter. It also stimulates glycine receptors, leading to a down regulation of excitatory NMDA receptors. (Glycine is also used in the biosynthesis of hemoglobin, which is very important in the maintenance of red blood cell integrity and oxygen transport.)
USES IN CFS/ME. Dr. Majid Ali, author of The Canary and Chronic Fatigue, makes extensive use of taurine as an antioxidant and has reported excellent results in treating fatigue and chronic constipation. Dr. Cheney has observed that taurine may also be of benefit in treating hyperactive nervous system responses. CFS/ME patients have been shown to have high amounts of glutamate in the brain, which increases neuroexcitatory responses. Because taurine slows CNS impulses, it may help relieve symptoms such as insomnia, anxiety, and restlessness, especially when taken in conjunction with magnesium. Taurine is transported easily across the blood-brain barrier, allowing taurine supplements to work in the brain.
PROTOCOL. Dr. Ali recommends a dosage of 250 mg/day, along with magnesium and potassium. Dr. Cheney recommends ½ cc of injectable magnesium (250 mg) accompanied by ½ cc injectable taurine.
PROS AND CONS. Taurine has very few side effects, however, excess doses can cause GI upset (yellow diarrhea, gas, pale stools).
AVAILABILITY AND COST. Taurine can be purchased in most health food and vitamin stores and costs less than $10 a bottle. Powdered forms can be purchased, for those who prefer to titrate dosage.
FURTHER READING
Very thorough discussion of the role of taurine: http://me-cfsmethylation.com/viewtopic.php?f=3&t=149
RESEARCH
El Idrissi A , Trenkner E. “Taurine as a modulator of excitatory and inhibitory neurotransmission.” Neurochem Res. 2004 Jan;29(1):189-97. http://www.ncbi.nlm.nih.gov/pubmed/14992278 (Abstract)
Liu, Y, Tonna-DeMasi, M, Park, E, Schuller-Levis, G, Quinn, MR. "Taurine chloramine inhibits production of nitric oxide and prostaglandin E2 in activated C6 glioma cells by suppressing inducible nitric oxide synthase and cyclooxygenase-2 expression. "Brain Res. Mol. Brain Res. 59,189-195. http://www.sciencedirect.com/science/article/pii/S0169328X98001454
Nakagawa K, Kuriyama K. “Effect of taurine on alteration in adrenal functions induced by stress.” Jap. J. Pharmacol. 1975 Dec;25(6):737-46. http://www.ncbi.nlm.nih.gov/pubmed/6814 (Abstract)
Park E, Jia J, Quinn MR, Schuller- Levis G. “Taurine chloramine inhibits lymphocyte proliferation and decreases cytokine production in activated human leukocytes.” Clin Immunol. 2002 Feb;102(2):179-84. http://www.ncbi.nlm.nih.gov/pubmed/11846460 (Abstract)
ANTIOXIDANTS
DESCRIPTION. Antioxidants are a group of vitamins, minerals, and enzymes that help protect cells from free radical damage.
BACKGROUND. Antioxidants have long been used as preservatives because of their ability to retard the oxidation that causes oils to become rancid. However, they have garnered increased attention over the past few years for their medical value. The same process that allows them to prevent oils from becoming rancid also protects the body from damage caused by free radicals. Free radicals are atoms or groups of atoms that have lost an electron. These molecules containing unpaired electrons are highly unstable and can easily pick up other elements, causing volatile reactions. When large numbers of free radicals are formed, whether from exposure to radiation, toxic chemicals or rancid oils, or because of prolonged illness and immune activation, significant damage can result. When dangerously high levels of free radicals are present, they can cause changes in protein structure. The body may identify the altered proteins as foreign elements and launch an immune system attack.
The body has its own defenses against excess free radical formation. The three most potent antioxidants produced in the body are superoxide dismutase (SOD), CoQ10, and glutathione peroxidase. However, the group of biochemicals known as antioxidants are also found abundantly in nature in the form of vitamins, minerals, and enzymes. Among the most widely used antioxidants are vitamins A, C, and E, alpha lipoic acid (ALA), gamma-linoleic acid (GLA), the amino acid cysteine, glutathione, taurine, the mineral selenium, CoQ10, and the bioflavonoids in pycnogenol, milk thistle, and gingko.
Antioxidants operate in concert to prevent free radical damage. A single antioxidant, once it has neutralized the free radical, can itself cause cell damage. The action of other antioxidants is necessary to return antioxidants to their reduced state, in which they can continue to scavenge free radicals. Therefore, antioxidants should be taken in combination rather than single forms. An article in the New England Journal of Medicine reports that heavy smokers in Finland who took very high doses of the antioxidant beta carotene had a higher rate of lung cancer than those taking a placebo (CFIDS Chronicle, Spring 1995). However, when beta carotene was combined with vitamin E, this was not the case.
Due to the potential of antioxidants to mitigate the more damaging effects of chronic illnesses (including cancer and diabetes) research on antioxidants is rapidly evolving. In 2004 Rezk et al proposed a new class of antioxidants based on the mechanism of vitamin E. In a study comparing the activities of different forms of vitamin E, the researchers discovered that vitamin E phosphate prevented the transfer of free radicals by forming a detergent barrier.
USES IN CFS/ME. Several studies have confirmed oxidative damage in CFS/ME patients. In 2000 a team of Italian researchers investigating the source of muscle pain found oxidative damage to DNA and lipids (fats) in the muscle tissue of CFS/ME patients. They also found significant differences in the composition of muscle membranes as compared to controls and patients with FM. The researchers concluded that their data “support an organic origin of CFS, in which muscle suffers oxidative damage.”
Patients with CFS/ME who experience depression also show evidence of free radical formation. In a 2001 study conducted by Maes et al, glutathione peroxidase levels were found to correlate with depressed mood and autonomic symptoms. The lower the glutathione levels, the greater the depression. The researchers recommended supplementation with glutathione, NAC and selenium.
Two studies conducted independently in 2000 and 2005 found that oxidative stress in CFS/ME patients could be measured through blood samples. In Australia, Richards et al measured methemoglobin in CFS/ME patients and controls.
Methemoglobin (pronounced “met-hemoglobin”) is an altered form of hemoglobin that does not bind well to oxygen, limiting the blood's ability to carry oxygen to tissues and organs. The formation of methemoglobin can be caused by various health problems and is a sign of oxidative stress. The study found that in CFS/ME patients, symptoms such as sleep disturbance, pain, and fatigue correlated with methemoglobin levels. They concluded that their data suggested that “oxidative stress due to excess free radical formation is a contributor to the pathology of CFS and was associated with symptom presentation.”
A second study by Kennedy et al. investigated free radical damage in CFS/ME symptoms using the “gold standard” of oxidative stress: isoprostanes. Isoprostanes are prostaglandin-like compounds which are formed after free radicals catalyze essential fatty acids. They have long been recognized as an accurate predictor of oxidative stress. Kennedy et al found that in CFS/ME patients, raised levels of isoprostanes correlated with post-exertional malaise. They postulated that in CFS/ME the excessive free radical formation could be due to persistent viral infection, to inflammation, or to metabolic abnormalities in mitochondria and lipids.
Antioxidants fall into many classes. The most commonly recommended antioxidants for CFS/ME patients are:
Vitamins: A, C, E
Vitamin co-factors: CoQ10
Minerals: Manganese, selenium, zinc
Hormones: Melatonin
Flavonoids: Quercetin, pycnogenol, grape seed extract, Ecklonia cava
Phenols: Silymarin
Plant sources: Capsaicin, bilberry
Enzymes: SOD
Various Others: N-acetyl cysteine, alpha lipoic acid, essential fatty acids, glutathione, taurine
PROTOCOL. Most, if not all, CFS/ME doctors have included some form of antioxidant therapy into their protocols. Usually they recommend a broad-spectrum approach, as opposed to single-supplement therapy, accompanied in many cases by bioflavonoids such as pycnogenol (which is a potent antioxidant), grape seed extract, or “super foods” such as blue-green algae. Vitamin E, because it is the only fat-soluble antioxidant, is particularly good in combination with other antioxidants.
Martin Pall, one of the leading researchers of oxidative stress in CFS/ME, recommends vitamin C, flavonoids, Ecklonia cava extract, B12, CoQ10, vitamin E, lipoic acid, as well as a host of other antioxidants to combat free radical damage.
Dr. Cheney recommends daily doses of 2000-4000 mg vitamin C, 400-800 IU of Vitamin E, 200 mg of CoQ10, 100-300 mg of lipoic acid, omega-6 and omega-3 essential fatty acids and flavonoids. He stresses that because high doses of antioxidants can increase oxidative stress, flavonoids should be taken to mitigate potential free radical damage stemming from excessive antioxidant activity.
455
Dr. Myhill recommends 300 mg of CoQ10 daily for three months, then reduced to 100 mg daily, 250 mg of glutathione daily together with 20 mcg of selenium as well as minerals to help produce the powerful free radical scavenger, superoxide dismutase. (Please see below for her discussion of antioxidants.)
FURTHER READING
Dr. Myhill's excellent discussion of antioxidants: http://drmyhill.co.uk/wiki/Antioxidants
Logan, Alan C. and Cathy Wong. “Chronic Fatigue Syndrome: Oxidative Stress and Dietary Modifications.” Altern Med Rev 2001;6 (5): 450-459. http://www.altmedrev.com/publications/6/5/450.pdf
This article contains an excellent summary of research concerning oxidative stress in CFS/ME as well as a proposed list of antioxidant treatments.
Martin Pall's supplement list: http://esme-eu.com/supplements/supplements-in-me-cfs-by-prof-martin-pall-article276-139.html
Dr. Cheney's talk on CFS/ME treatments, including antioxidants: http://www.me-cfs.info/cheneyII3.pdf
RESEARCH
Fulle S, Mecocci P, Fan G, Vecchiet I, Vecchini A, Racciotti D, Cherubini A, Pizzigallo E, Vecchiet L, Senin U, Beal MF. “Specific oxidative alterations in vastus lateralis muscle of patients with the diagnosis of chronic fatigue syndrome.” Free Radic Biol Med. 2000 Dec 15;29(12):1252-9. http://www.ncbi.nlm.nih.gov/pubmed/11118815 (Abstract)
Kennedy, Gwen, Vance A. Spence, Margaret McLaren, Alexander Hill, Christine Underwood, Jill J.F. Belch. “Blood parameters indicative of oxidative stress are associated with symptom expression in chronic fatigue syndrome.” Free Radical Biology & Medicine 39 (2005) 584 – 58. http://www.cfids-cab.org/rc/Kennedy.pdf
Maes M, Mihaylova I, Kubera M, Uytterhoeven M, Vrydags N, Bosmans E. “Lower whole blood glutathione peroxidase (GPX) activity in depression, but not in myalgic encephalomyelitis /chronic fatigue syndrome: another pathway that may be associated with coronary artery disease and neuroprogression in depression.” Neuro Endocrinology letters. 2011;32(2):133-40. http://www.ncbi.nlm.nih.gov/pubmed/21552194 (Abstract)
Miwa K, Fujita M. “Fluctuation of serum vitamin E (alpha-tocopherol) concentrations during exacerbation and remission phases in patients with chronic fatigue syndrome.” Heart Vessels. 2010 Jul;25(4):319-23. http://www.ncbi.nlm.nih.gov/pubmed/20676841 (Abstract)
Rezk BM, Haenen GR, Van Der Vijgh WJ, Bast A. “The extraordinary antioxidant activity of vitamin E phosphate.” Biochim Biophys Acta. 2004 Jul 5;1683(1-3):16-21. http://www.ncbi.nlm.nih.gov/pubmed/15238215 (Abstract)
Richards RS, Roberts TK, McGregor NR, Dunstan RH, Butt HL. “Blood parameters indicative of oxidative stress are associated with symptom expression in chronic
456
fatigue syndrome.” Redox Rep. 2000;5(1):35-41. http://www.ncbi.nlm.nih.gov/pubmed/10905542 (Abstract)
Saransaari, P, Oja S. “Nitric oxide is involved in taurine release in the mouse brainstem under normal and ischemic conditions.” Amino Acids. 2008 Apr;34(3):429-36 http://www.ncbi.nlm.nih.gov/pubmed/17665274 (Abstract)
BETAINE HCl
DESCRIPTION. Betaine HCl is a synthesized chemical compound consisting of betaine, a methyl group donor, and hydrochloride, a salt.
BACKGROUND. Betaine is a vitamin-like substance that was originally derived from beets. For many years Betaine HCl was added to over-the-counter digestive aids, until in 1993 the FDA determined that it has not been proven “generally safe and effective.” At that point Betaine HCl began to be sold as a separate supplement.
Betaine HCl is still marketed as a digestive aid, particularly for the treatment of hypochloridia, a condition in which the stomach does not produce enough acid. Hypochloridia can occur after taking stomach acid suppressors (antacids, proton pump inhibitors), through H. Pylori infections (which interfere with stomach acid production), as well as any disease process that causes inflammation in the stomach lining. Stomach acid is often low in the elderly.
Lack of stomach acid can lead to the phenomenon known as “dumping,” in which the stomach's contents (chyme) are released into the small intestines before having been adequately broken down. The ability of the small intestines to further break down the chyme can result in poor absorption of nutrients, leading to deficiency states, particularly of minerals, which require acid to be absorbed. One of the most common symptoms of hypochloridia is reflux, which is frequently misdiagnosed as excess acid.
The most reliable test to determine hypochloridia is the Heidelberg Capsule test. The capsule contains a high frequency transmitter attached to a string. When the capsule is swallowed and drawn back up the esophagus, it gives an instant pH reading.
USES IN CFS/ME. A number of clinicians have proposed that low levels of stomach acid are responsible for many of the GI symptoms found in CFS/ME patients. Dr. Cheney routinely recommends Betaine HCl as a supplement to correct hypochloridia and prevent dumping. Dr. Myhill also maintains that people with CFS/ME chronically suffer from low levels of stomach acid.
PROTOCOL. Dr. Cheney recommends starting with a capsule (or ½ capsule) with meals. Paradoxically, too low a dose may actually increase reflux, as there still isn't enough stomach acid to trigger the opening of the sphincter that releases chyme into the intestines. The food that then returns through the esophagus contains not only normally occurring stomach acid, but the additional Betaine HCl as well. According to Dr. Cheney, increasing the dose will actually reduce reflux.
PROS AND CONS. Although Betaine HCl does not contain hydrochloric acid (the HCl, in this case, is a salt), some people report improved digestion. The
457
supplement does have mild acidifying properties, which is perhaps why people report having to take so many capsules with their meals (up to seven). It is quite possible that many of its benefits may actually come from the betaine, which acts as a liver support.
AVAILABILITY AND COST. Betaine HCl is easily available from health food stores and from online suppliers. It is inexpensive. Vitacost markets a 100-capsule bottle of Twinlab's Betaine HCl for about $7.
FURTHER READING
Dr. Sara Myhill's excellent discussion of hypochloridia: http://www.drmyhill.co.uk/wiki/Hypochlorhydria_-_lack_of_stomach_acid_-_can_cause_lots_of_problems
Basic information about Betaine HCl: http://www.encyclopedia.com/doc/1G2-3435100086.html
A good explanation of the Heidelberg capsule test and hypochloridia. http://www.antiagingwellnesscenter.com/phcapsule.shtml
Dr. Paul Cheney on dumping, hypochloridia, and Betaine HCl supplementation. http://www.prohealth.com/library/showarticle.cfm?libid=8037
BIOFLAVONOIDS
Grape seed extract, Pycnogenol, Quercetin
DESCRIPTION. Bioflavonoids are glycosides (sugars) derived from citrus, paprika, and other plants, which serve to protect capillaries. Although formerly known as "vitamin P," bioflavonoids are not vitamins.
BACKGROUND. Bioflavonoids were first extracted from paprika in 1936 by a scientist who claimed that the substance had a greater effect than vitamin C in reducing capillary bleeding. It was later shown that the substance, or rather substances, helped maintain capillary strength by inhibiting permeability of the walls (rather than maintaining the actual structure, as does vitamin C). This may be because bioflavonoids inhibit oxidation of epinephrine (adrenaline), the hormone directly responsible for capillary wall integrity. Bioflavonoids enhance absorption of vitamin C and, when taken together, can help protect and preserve capillaries, increase circulation, prevent cataracts, and produce a mild antibacterial effect. Flavonoids have anti-allergic, anti-inflammatory and anti-microbial effects.
Dietary sources include buckwheat, black currants, peppers, and the white part of citrus peel. There are many bioflavonoids available for purchase through health food stores and online vitamin suppliers.
Bioflavonoids are rapidly absorbed in the system, and almost as rapidly excreted through the kidneys. Peak blood levels occur roughly two hours after ingestion, which means that to be effective, they should be taken throughout the day.
458
USES IN CFS/ME. Bioflavonoids are poorly absorbed, so for better utilization its best to take several. The most active intracellular free radical scavengers are lycopene, a carotenoid found in red fruits (except strawberries) and lutein, found in green leafy vegetables. Dr. Pall recommends FlaviNOx, which is a combination of standardized bioflavonoids derived from herbs (gingko, bilberry, milk thistle, grape seed extract, decaffeinated green tea extract, cranberry and hawthorn). The combination of antioxidants in FlaviNOx is designed to scavenge peroxynitrite and superoxide, two highly damaging free radicals.
AVAILABILITY AND COST. A 90-capsule bottle of FlaviNOx (Allergy Research Group) costs roughly $35.
GRAPE SEED EXTRACT
DESCRIPTION. Grape seed extract is a polyphenolic compound derived from grape seeds.
BACKGROUND. Grape seeds contain polyphenols, procyanidins, and proanthocyanidins, which are antioxidants many times more powerful than vitamin C or E. Grape seed extract is reported to be a potent peroxynitrite scavenger, and therefore can protect the cells from intracellular damage. The effects of polyphenols are far-reaching, including the inhibition of skin cancer, reduction of inflammation, neuroprotective action, improvement of cerebral circulation, acceleration of wound healing, modulation of intestinal flora, repairing leaky gut, and immune system regulation.
USES IN CFS/ME. Grape seed extract is often used as a less expensive alternative to pycnogenol. Patients report that it helps with pain.
PROTOCOL. One 100 mg tablet taken with food.
AVAILABILITY AND COST. Grape seed extract is widely available in health food stores and through online distributors. A bottle of 120 capsules can cost as little as $13. Grape seed extract is frequently combined with other bioflavonoids, such as green tea and resveratrol (found in grape skin) to increase its antioxidant effects.
FURTHER READING
Sloan Kettering's review of the mechanisms of grape seed extract. Includes a list of studies. http://www.mskcc.org/cancer-care/herb/grape-seed
RESEARCH
Afaq F, Katiyar SK. “Polyphenols: Skin Photoprotection and Inhibition of Photocarcinogenesis.” Mini Rev Med Chem. 2011 Oct 28. http://www.ncbi.nlm.nih.gov/pubmed/22070679 (Abstract)
Lin, B. “Polyphenols and Neuroprotection against Ischemia and Neurodegeneration.” Mini Rev Med Chem. 2011 Oct 28 http://www.ncbi.nlm.nih.gov/pubmed/22070681 (Abstract)
Vendrame S, Guglielmetti S, Riso P, Arioli S, Klimis-Zacas D, Porrini M. “Six-week consumption of a wild blueberry powder drink increases bifidobacteria in the
459
human gut.” J Agric Food Chem. 2011 Nov 7. http://www.ncbi.nlm.nih.gov/pubmed/22060186 (Abstract)
PYCNOGENOL
DESCRIPTION. Pycnogenol (proanthocyanadin) is a bioflavonoid antioxidant derived from the bark of the French maritime pine tree.
BACKGROUND. Pycnogenol is a potent free radical scavenger. Studies have shown that, as an antioxidant, pycnogenol is up to 50 times more effective than other antioxidants to clear free radicals created from chemical sources (air pollution and food additives). It is 20 times more effective than vitamin C in scavenging superoxide, hydroxyl, and peroxide radicals. Pycnogenol is reported to enhance immune system function, increase energy, promote healing, and reduce allergic reactions. It is particularly effective in the brain.
USES IN CFS/ME. Pycnogenol has not been widely investigated for use in CFS/ME patients although it has been researched for other virally induced diseases. Some patients who have used pycnogenol report small increases in mental and physical energy and better resistance to bacterial and viral infections as well as stress.
PROTOCOL. The recommended dosage is 50 mg a day, taken with food. Some CFS/ME patients report that pycnogenol is more effective on an empty stomach.
AVAILABILITY AND COST. Pycnogenol can be purchased from health food stores and vitamin catalogs. Twinlab markets a 60-capsule bottle of pycnogenol (50 mg) for $25 through Vitacost.
FURTHER READING
Sloan Kettering's excellent summary of the mechanisms of pycnogenol. Contains a list of research studies: http://www.mskcc.org/cancer-care/herb/pine-bark-extract
Iravani S., and B. Zolfaghari. “Pharmaceutical and nutraceutical effects of Pinus pinaster bark extract.” PhD. Res Pharm Sci. 2011 Jan-Jun;6(1): 1–11. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3203267/
A thorough review of all research articles investigating pycnogenol.
RESEARCH
Feng WY, Tanaka R, Inagaki Y, Saitoh Y, Chang MO, Amet T, Yamamoto N, Yamaoka S, Yoshinaka Y. “Pycnogenol, a procyanidin-rich extract from French maritime pine, inhibits intracellular replication of HIV-1 as well as its binding to host cells.” Jpn J Infect Dis. 2008 Jul;61(4):279-85. http://www.ncbi.nlm.nih.gov/pubmed/18653969 (Abstract)
QUERCETIN
BACKGROUND. Quercetin, a flavonol, is chiefly used to treat asthma and allergies. Quercetin has properties similar to that of the antihistamine disodium cromoglycate (found in Gastrocrom and Nasalcrom). It can inhibit mast cell
460
production and block histamine release, two functions that together can curb many allergic responses. In its antioxidant function, quercetin decreases the synthesis of pro-inflammatory leukotrienes, and inhibits free radical production and lipid peroxidation.
Quercetin is reported to help relieve muscle pain, particularly along the upper back and shoulders. It is commonly found in many food sources: green tea, apples, red onions, red grapes, citrus fruits, tomato, broccoli, leafy green vegetables, cranberries and raspberries, among others.
USES IN CFS/ME: An interesting study conducted in 2009 by Davis et al found that quercetin increased the genesis of mitochondria in mice, significantly improving exercise tolerance. The reason this study is important is that it was done in vivo. (Most studies on antioxidants are performed in test tubes.) As exercise intolerance is the hallmark symptom of CFS/ME, quercetin may play an important role in improving physical stamina among people with CFS/ME.
PROTOCOL. Because it is so poorly absorbed, quercetin needs to be taken with bromelain, an enzyme found in pineapple. Dr. James Balch, author of Prescription for Nutritional Healing, recommends 1000 to 2000 mg one to three times a day to prevent or lessen the severity of asthma attacks and allergies. CFS/ME patients are advised to start with much smaller doses, 200-1200 mg a day.
PROS AND CONS. Quercetin is the most widely used bioflavonoid among patients with CFS/ME. A number of allergy-prone patients with CFS/ME have noted that allergy symptoms subside with quercetin. For patients with many allergies, this may provide overall improvement because allergy symptoms can cause systemic problems. Some patients with interstitial cystitis have noted an improvement in symptoms after taking quercetin. The primary side effect is that high doses may cause diarrhea.
AVAILABILITY AND COST. Quercetin (with bromelain) is available from health food stores and online vitamin catalogs. A three-month supply may cost as little as $8. ProHealth markets a 100-tablet bottle of a quercetin-bromelain combination (also containing vitamin C and magnesium) for about $15.
FURTHER READING
Davis JM, Murphy EA, Carmichael MD, Davis B. “Quercetin increases brain and muscle mitochondrial biogenesis and exercise tolerance.” Am J Physiol Regul Integr Comp Physiol. 2009 Apr;296(4):R1071-7. http://www.ncbi.nlm.nih.gov/pubmed/19211721 (Abstract)
Park HH, Lee S, Son HY, Park SB, Kim MS, Choi EJ, Singh TS, Ha JH, Lee MG, Kim JE, Hyun MC, Kwon TK, Kim YH, Kim SH. “Flavonoids inhibit histamine release and expression of proinflammatory cytokines in mast cells.” Arch Pharm Res. 2008 Oct;31(10):1303-11. http://www.ncbi.nlm.nih.gov/pubmed/18958421 (Abstract)
Pearce FL, Befus AD, Bienenstock J. “Mucosal mast cells. III. Effect of quercetin and other flavonoids on antigen-induced histamine secretion from rat intestinal
461
mast cells.” J Allergy Clin Immunol. 1984 Jun;73(6):819-23. http://www.ncbi.nlm.nih.gov/pubmed/6202731 (Abstract)
Shaik YB, Castellani ML, Perrella A, Conti F, Salini V, Tete S, Madhappan B, Vecchiet J, De Lutiis MA,Caraffa A, Cerulli G. “Role of quercetin (a natural herbal compound) in allergy and inflammation.” J Biol Regul Homeost Agents. 2006 Jul-Dec;20(3-4):47-52. http://www.ncbi.nlm.nih.gov/pubmed/18187018 (Abstract)
BUTYRIC ACID (BUTYRATE)
DESCRIPTION. Butyrates (butanoic, or butyric acid) are short-chain saturated fatty acids found naturally in the human intestine and in butter fat.
BACKGROUND. Short-chain fatty acids (volatile fatty acids) are produced in the colon as natural by-products of the bacterial fermentation of fiber. These fatty acids provide an energy source for the mucosal cells of the lining of the colon, enabling them to check the proliferation and establishment of pathogens (such as salmonella and Candida) and allowing greater absorption of magnesium and vitamin K. Deficiency of these fatty acids results in malabsorption, diarrhea, and, over the long term, colitis.
Of the three fatty acids found in all mammals – butyrate, acetate, and propionate – butyrate is the preferred energy substrate. It stimulates the normal proliferation of mucous cells, enabling greater efficiency of all colonic functions. Butyrates have been used successfully to treat Candida overgrowth (yeast infection), cancer, ulcerative colitis, and nonspecific inflammatory conditions of the colon. It is one of the treatments recommended for leaky gut and for alleviating food sensitivities.
USES IN CFS/ME. A significant number of people with CFS/ME suffer from gastrointestinal problems. According to Dr. Cheney, 90% of his CFS/ME patients have small intestinal bacterial overgrowth (SIBO), a condition in which bacteria from the large intestine migrate into the small intestines, interfering with fat and carbohydrate metabolism and causing a spate of GI symptoms. Rao et al found that 50% of CFS/ME patients meet the criteria for irritable bowel syndrome (IBS), a gut motility disorder. Butyrates, because they provide a substrate for beneficial intestinal flora, can be used in conjunction with probiotics to help restore gut mucosa damaged by SIBO as well as maintaining gut motility.
Although butyrates are primarily recommended for treating digestive disorders, it may also have a positive effect on some neurological problems associated with CFS/ME. Dr. Cheney proposes that an imbalance in the actions of the neuroexcitatory chemical NMDA (N-methyl-D-aspartate) and the neuroinhibitor GABA (gamma amino butyric acid) may lead to many of the troubling neurological symptoms experienced by patients with CFS/ME (insomnia, intolerance of sensory stimuli, seizure-like activity, pain) (CFIDS Chronicle, Spring 1995).
For many patients, down regulation of the NMDA receptors, accomplished with small doses of Klonopin (clonazepam), magnesium, Nimotop (nimodipine), melatonin, or calcium channel blockers, leads to general improvement of all
462
symptoms. Butyrate, because it forms a component of GABA, may also rectify some of this neurochemical imbalance by increasing the amount of neuroinhibitory action in the brain.
PROTOCOL. Butyrate is usually taken orally. The suggested dose is one or two capsules with each meal. It smells awful, so you may want to store it in the refrigerator.
PROS AND CONS. Butyrate is inexpensive, safe, and does not require a prescription.
AVAILABILITY AND COST. ButyrEn tablets, marketed by Allergy Research Group, are hypoallergenic, containing no yeast, wheat, corn, soy, dairy products, or artificial colors or resins. The tablets are buffered with calcium and magnesium. ButyrEn is available from online distributors and some specialized vitamin stores. One bottle of 100 capsules costs as little $9 on amazon. PureFormulas markets a 90-capsule bottle of Cal-Mag Butyrate made by Ecological Formulas for $10.50. Shipping is free.
FURTHER READING
Life Extension is a bit pricier than other suppliers, but their website contains a very thorough description of the mechanisms of butyric acid. http://www.lifeextensionvitamins.com/bualregr.html
RESEARCH
Rao, A Venket, Alison C Bested, Tracey M Beaulne, Martin A Katzman, Christina Iorio, John M Berardi and Alan C Logan. “A randomized, double-blind, placebo-controlled pilot study of a probiotic in emotional symptoms of chronic fatigue syndrome.” Gut Pathogens 2009, 1:6. http://www.gutpathogens.com/content/1/1/6
CHOLINE
DEFINITION. Choline is an amine (a nitrogen-containing compound) similar in function to B vitamins.
BACKGROUND. Choline is an essential nutrient, which means it cannot be synthesized by the body and must be obtained through food sources. Foods high in choline include egg yolk, liver, fatty meats, nuts and brown rice.
Choline performs three vital biological functions: 1) It is an important component of phosphatidylcholine, which forms cell walls and supports cellular function; 2) Choline serves as a precursor to acetylcholine, the neurotransmitter responsible for memory formation and muscle movement; 3) Choline is an important methyl donor, supporting the methylation cycle through its metabolite, trimethylglycine (betaine).
A deficiency in choline can lead to liver damage (“fatty liver”) and a reduction in kidney function. Lack of choline in the diet can also cause infertility, growth impairment, bone abnormalities, and hypertension. Because choline plays such an important role in nervous system development, a deficiency in early life can lead to
463
neurological deficits. Vegans and athletes are particularly prone to choline deficiency.
USES IN CFS/ME. Because choline serves as a marker for certain types of brain damage, it is one of the compounds that is measured in magnetic resonance (MR) spectroscopy. For example, high amounts of choline accompanied by low amounts of creatine and N-acetyl aspartate (NAA) are indicative of stroke (cerebral ischemia and hypoxia). MR spectroscopy can also be used to monitor changes in tumors, stroke, epilepsy, metabolic disorders, infections, and neurodegenerative diseases.
In 2004 Chaudhuri and Behan used MR spectroscopy to assess brain chemistry in CFS/ME patients. They found that in CFS/ME patients, choline levels in the occipital cortex and basal ganglia were raised, but NAA and creatine were normal. The researchers concluded that in the absence of NAA and with no structural abnormalities, the increase in choline was probably due to increased phospholipase activity (the enzyme that breaks down the phospholipids that make up cell walls) rather than to inflammation. They theorized that viral activity could possibly contribute to the increased choline, as many viruses increase the activity of phospholipase.
While Chaudhuri and Behan concluded that inflammation in the brain was not indicated by their test results, further research indicates otherwise. Martin Pall has suggested that activation of NMDA receptors (due to oxidative stress) provides the missing inflammatory pathway that Chaudhuri and Behan were unable to identify. In fact, an increase in choline can be an early signal of an inflammatory process, even in the absence of NAA. The mechanism which induces release of choline was identified by Gasull et al as an inhibition of phosphatidylcholine synthesis rather than phospholipase degradation. The researchers found that the increase in extracellular choline was induced by NMDA receptor activation, which ties in with Martin Pall's theory. In addition, Gasull's group found that early choline release was directly related to excitotoxic cell death caused by glutamine.
PROTOCOL. Given the important role of choline in neuronal protection from oxidative stress, as well as the fact that it is a component of acetylcholine, choline comprises a valuable addition to any CFS/ME treatment plan. Dr. Cheney recommends taking 50 mg of choline bitartrate a day. Dr. Teitelbaum recommends the same dose, accompanied by vitamin C.
High doses (10 to 16 grams/day) of choline are not recommended. Side effects from excessive intake of choline have been associated with a fishy body odor, vomiting, salivation, and increased sweating. (The fishy body odor results from excretion of trimethylamine, a metabolite of choline.) Taking large doses of choline in the form of phosphatidylcholine (lecithin) does not generally result in fishy body odor. However, lecithin is not usually well-tolerated by CFS/ME patients.
AVAILABILITY AND COST. Choline bitartrate supplements are not widely available, so most people decide to purchase lecithin powder, which is inexpensive and easy to find. PureFormulas.com markets a bottle of 100 choline bitartrate capsules (235 mg) for roughly $10. Purebulk.com sells a 100-gram container of
464
choline bitartrate powder for $4.25. The powder may be a more viable option for most people as it allows for titration. Many B vitamin formulations contain choline, so check labels. It may be worthwhile to purchase a good-quality B-complex supplement that includes choline, as this will give you the proper balance of B vitamins as well.
FURTHER READING
This Oregon University site provides excellent information about choline. http://lpi.oregonstate.edu/infocenter/othernuts/choline/
“What are Choline and Inositol?” (Good overview): http://www.livestrong.com/article/326852-what-are-choline-inositol/
“Choline on the Brain? A Guide to Choline in Chronic Fatigue Syndrome.” Cort Johnson. Aug, 2005. http://aboutmecfs.org.violet.arvixe.com/Rsrch/CholineBrain.aspx
Ray Sahelian's sensible advise on choline: http://www.raysahelian.com/cdp.html
“Fundamentals of MR Spectroscopy.” John R. Hesselink. (A nice summary of MR spectroscopy.) http://spinwarp.ucsd.edu/neuroweb/Text/mrs-TXT.htm
RESEARCH
Chaudhuri, A., P.O. Behan. “In vivo magnetic resonance spectroscopy in chronic fatigue syndrome.” Prostaglandins, Leukotrienes and Essential Fatty Acids 71 (2004) 181–183. http://www.cfids-cab.org/cfs-inform/MitochondrialATP/chaudhuri.behan04.pdf
Chaudhuri A, Condon BR, Gow JW, Brennan D, Hadley DM. “Proton magnetic resonance spectroscopy of basal ganglia in chronic fatigue syndrome.” Neuroreport. 2003 Feb 10;14(2):225-8. http://www.cfids-cab.org/cfs-inform/Brainscans/chaudhuri.etal03.pdf
Cohen BM, Renshaw PF, Stoll AL, Wurtman RJ, Yurgelun-Todd D, Babb SM. “Decreased brain choline uptake in older adults. An in vivo proton magnetic resonance spectroscopy study.” JAMA. 1995 Sep 20;274(11):902-7. http://www.nutrasal.com/library/pdfs/21.pdf
Doležal, Vladimír, Stanislav Tuček. “Activation of muscarinic receptors stimulates the release of choline from brain slices.” Biochem Biophys Res Commun. 1984 May 16;120(3):1002-7. http://www.ncbi.nlm.nih.gov/pubmed/6732780 (Abstract)
Gasull, Teresa, Nuria DeGregorio-Rocasolano, Agustin Zapata and Ramon Trullas. “Choline Release and Inhibition of Phosphatidylcholine Synthesis Precede Excitotoxic Neuronal Death but Not Neurotoxicity Induced by Serum Deprivation.” First Published on March 28, 2000. The Journal of Biological Chemistry, 275,18350-18357. http://www.jbc.org/content/275/24/18350.full
COQ10 (UBIQUINONE, UBIQUINOL)
DESCRIPTION. CoQ10 (ubiquinone) is a fat-soluble coenzyme found in the mitochondria of most mammal cells.
465
BACKGROUND. CoQ10 was first discovered by R.A. Morton, a biochemist who gave it the name ubiquinone after its ubiquitous presence in nearly all living things. "Co" stands for coenzyme (a vitamin-like substance), "Q" for quinone (the group of organic chemicals to which CoQ belongs), and "10" for the number of isoprene units that characterize the particular coenzyme found in animal cells.
CoQ10 is vital for electron transport, the intracellular function that ultimately provides the energy necessary to sustain life. CoQ10 is also a powerful antioxidant and is important in immune system function. The Japanese have successfully used CoQ10 to treat gum disease, heart disease, and high blood pressure, and to enhance the effectiveness of the immune system. Research performed in Japan and elsewhere indicates that CoQ10 can be of benefit in treating allergies (owing to its ability to block the effects of histamine), asthma, candidiasis, obesity, diabetes, mental function diseases such as Alzheimer's disease, and can slow the aging process (CoQ10 levels decline with age).
High amounts of CoQ10 occur naturally in fatty saltwater fish, especially mackerel, salmon, and sardines.
USES IN CFS/ME. CoQ10 is one of the most frequently used supplements for the treatment of CFS/ME-related fatigue because of its importance in the production of adenosine triphosphate (ATP), the cellular source of energy. In addition to reducing fatigue, CoQ10 may alleviate muscle weakness and pain. It is also one of the few supplements that seems to reduce cognitive dysfunction. Its role as a free radical scavenger may lead to improvement in immune responses in patients with CFS/ME. Although its effects as a natural antihistamine have not yet been specifically explored in CFS/ME, patients with allergies may benefit from CoQ10.
There is also evidence that CoQ10 is deficient in CFS/ME patients. In 2009 Maes et al measured plasma CoQ10 in 58 CFS/ME patients. Compared to normal controls, the CFS/ME group had values significantly below the lowest recorded levels of the control group. Patients with very low levels of CoQ10 suffered significantly more from concentration and memory disturbances. The researchers concluded that lowered levels of CoQ10 play a role in the pathophysiology of ME/CFS and that “symptoms, such as fatigue, and autonomic and neurocognitive symptoms may be caused by CoQ10 depletion.” Their results suggested that patients with CFS/ME would benefit from CoQ10 supplementation in order to normalize the low CoQ10 syndrome.
PROTOCOL. Nearly all CFS/ME physicians recommend supplementation with CoQ10. CoQ10 can be taken in a single dose or divided into two doses taken at different times during the day. There is evidence that dividing the dose is more effective than taking it all at once. The normal recommended dose is between 30 and 200 mg/day. Dr. Lapp and Dr. Klimas recommend 120 mg a day. Sublingual CoQ10, reputedly more effective against cognitive dysfunction, may be taken at higher doses. Oral CoQ10, although primarily absorbed by the digestive tract and liver, is also effective for some patients. The oral dosage varies, but is usually 25 to 50 mg/day. It may take up to eight weeks to see effects from oral CoQ10. Because
466
CoQ10 is fat-soluble, it should be taken with a meal that contains some kind of fat or oil.
PROS. Taken at lower doses, CoQ10 is a supplement with very few side effects. Patients report improvements in energy, stamina, light-headedness, and syncope (fainting). Dr. Lapp reports that half of his patients see improvement after taking CoQ10. A significant number of patients, particularly those with fibromyalgia, find that CoQ10 increases their energy over the course of the day.
CONS. Some patients report that CoQ10, while giving them an initial energy boost, also increases insomnia and causes jitters. Some people report, paradoxically, that CoQ10 produces exhaustion, although this effect may be more common in the acutely ill than in those with stable symptoms. CoQ10 lowers blood sugar levels, which may be problematic for patients with hypoglycemia. High doses can cause flu-like symptoms.
AVAILABILITY AND COST. CoQ10 can be purchased at most health food stores and from online distributors. There is a mind-boggling array of CoQ10 products. High-grade brands are preferred. (CoQ10 deteriorates rapidly when exposed to heat and light.) Because CoQ10 is fat-soluble, it should be purchased as a softgel (not capsule), preferably with a natural preservative (such as vitamin E).
Sublingual CoQ10 can be purchased from online sources without a prescription. Intensive Nutrition, Inc. markets a sustained-release sublingual CoQ10 for $25 (80 mg, 30 count). Source Naturals sells sublingual CoQ10 for $14 (30 mg, 120 count).
CoQ10 is also available by prescription as a gel. Unlike other forms of CoQ10, the gel is water soluble, and bypasses the GI tract completely. The gel is more easily absorbed that oral forms, so less CoQ10 needs to be taken. CoQ10 gel has been given orphan status by the FDA for treating mitochondrial dysfunction. (Orphan status means that a drug has been approved for the treatment of rare disorders.)
A more easily absorbed form of CoQ10, ubiquinol, is currently being marketed in the U.S. CoQ10 is converted in the body to ubiquinol, which is the active form of the enzyme, and therefore, more potent. Not only is ubiquinol more easily absorbed, it is longer acting than ubiquinone. Ubiquinol can be purchased from health food stores and online distributors. Vitacost sells a wide variety of ubiquinol products, ranging in cost from $8 to $74. (Read the labels carefully to confirm that the product contains pure ubiquinol.) Olympian Labs sells a bottle of 60 ubiquinol softgels (50 mg) with relatively few additives for $27.62.
Oral CoQ10 is not usually covered by insurance, as it is classed as a supplement.
FURTHER READING
Excellent summary of CoQ10 in CFS/ME: http://phoenixrising.me/?page_id=4759
An interesting and useful site containing a discussion of ubiquinol, a comparison of ubiquinol to CoQ10, links and research: http://ubiquinol.org/what-is-ubiquinol
Website of the International CoQ10 Association: http://www.icqa.org/ICQA/home.html
467
Ray Sahelian's informative site. Effects of CoQ10, studies and FAQs. http://www.raysahelian.com/coq10.html
Compounding pharmacies that make CoQ10 troches: http://www.mitoaction.org/blog/coq-10-update
Information on CoQ10 gel: http://www.epic4health.com/noname.html
PATIENT REVIEWS
Patient reviews of CoQ10: http://www.revolutionhealth.com/drugs-treatments/rating/coenzyme-q10-coq10-for-chronic-fatigue-syndrome-cfs-cfids-me?sort=recent
RESEARCH
Maes M, Mihaylova I, Kubera M, Uytterhoeven M, Vrydags N, Bosmans E. “Coenzyme Q10 deficiency in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is related to fatigue, autonomic and neurocognitive symptoms and is another risk factor explaining the early mortality in ME/CFS due to cardiovascular disorder.” Neuro Endocrinol Lett. 2009;30(4):470-6. http://www.ncbi.nlm.nih.gov/pubmed/20010505 (Abstract)
D-RIBOSE
DESCRIPTION. D-Ribose is a water-soluble simple sugar that is an important component of nucleic acids, vitamin B2, and various coenzymes.
BACKGROUND. Ribose was first identified in 1891 by Emil Fischer, a German chemist and recipient of the Nobel Prize in Chemistry. Fischer's primary work concerned sugars and the identification of their various functions. Ribose is an extremely important sugar in that it comprises the backbone of RNA, one of the three major macromolecules essential to all forms of life. Ribose is also a component of ATP, NADH and several other compounds that control the metabolism of carbohydrates, proteins, and fat.
USES IN CFS/ME. Mitochondrial defects that lead to low production of ATP, the principal source of cellular energy, have been thoroughly documented in people with CFS/ME. Low levels of ATP are responsible for the hallmark symptoms of CFS/ME, exercise intolerance and fatigue. However, direct supplementation with ATP seems to have no effect on either fatigue or stamina. This is due to the fact that ATP has a molecular weight of more than 500, which means that it is nearly impossible to absorb. Therefore, the mitochondrial defects leading to low ATP production must be addressed at a lower level in the metabolic chain.
The body makes ATP through the Krebs cycle, in which various enzymes convert citric acid into ATP. These enzymes are often deficient in people with CFS/ME, resulting in a lower production of ATP. The body can also make ATP from glucose, but the process involves first converting glucose into lactic acid, which then accumulates in the muscles, causing the familiar “burn” of over-exertion. This is also a longer and less efficient process than the Krebs cycle. D-Ribose cuts the time
468
required to produce ATP because the body can quickly convert D-Ribose into ATP without converting it first into lactic acid.
In a 2006 pilot study, Teitelbaum et al found that in 36 CFS/FM patients, 66% experienced improvement in energy, pain, sleep, mental clarity and overall well-being after treatment with D-Ribose. The average improvement in energy was 45%, while the global improvement was 30%. The researchers concluded that D-Ribose “significantly reduced symptoms in patients suffering from fibromyalgia and chronic fatigue syndrome.”
Apart from its uses in CFS/ME, D-Ribose is among the most popular nutritional supplements to have been recently patented. In 2010, Bioenergy Inc, the company which markets Corvalen (the brand recommended by Dr. Teitelbaum), achieved its highest revenue earnings in the history of the company.
PROTOCOL. The serving size recommended by Jarrow is 2 grams (½ tsp/one scoop) up to three times a day. Dr. Teitelbaum recommends 5000 mg (5 grams) of D-Ribose three times a day for two to three weeks, then twice a day. Dr. Myhill also recommends 15 grams a day. Interestingly, she notes that the effects of D-Ribose can be enhanced by caffeine. She notes that D-Ribose has a short half-life, which is why it must be taken in small doses throughout the day. D-Ribose should be taken with food.
While initial doses of 15 grams are recommended by Drs. Teitelbaum and Myhill, it should be remembered that many CFS/ME patients are sensitive to supplements. Dr. Cheney has observed that fully one-third of his patients cannot tolerate D-Ribose. To test for sensitivities, an initial small dose (1 to 2 grams a day) is recommended.
PROS. D-Ribose appears to be generally well tolerated by people with CFS/ME. Patients usually notice improvement in energy levels within two or three days, although one patient commented that “within an hour, it was like a super thick fog bank had dissipated.” D-Ribose works particularly well with brain fog, daytime sleepiness and hypersomnia.
CONS. Some patients report that D-Ribose makes them sleepy, and that it saps them of energy. Those who take high doses (15 grams a day) have reported diarrhea, nausea, and headache. Because D-Ribose is derived from corn, those with corn allergies may not be able to tolerate this supplement. Although D-Ribose does not have the same properties as table sugar, it can be converted back to glucose, which may have an adverse effect on patients with Candida, as well as those with blood sugar problems. D-Ribose supplementation is not advised for diabetics. Nor is it recommended for those with gout, as it causes an increase in uric acid levels (which are usually low in people with CFS/ME).
AVAILABILITY AND COST. D-Ribose is widely available in health food stores and from online suppliers. Costs range from $10 to $75, depending on the brand. Corvalen, the brand Dr. Teitelbaum prefers, sells for roughly $30 for a 280-gram container (56 servings, or roughly an 18-day supply at three scoops a day). Vitacost markets a 100-gram bottle made by Jarrow for about $10 (45 scoops).
469
FURTHER READING
Dr. Teitelbaum addresses questions about D-Ribose: http://www.endfatigue.com/web-newsletters/Newsletter_3_questions_d-ribose.html
Dr. Teitelbaum explains the functions and benefits of D-Ribose. http://www.endfatigue.com/health_articles_d-e/D-ribose-powerful_body_energizer.html
Teitelbaum JE, JA St. Cyr, C Johnson. “The Use of D-Ribose in Chronic Fatigue Syndrome and Fibromyalgia: A Pilot Study” J Alternative and Complementary Medicine2006;12(9):857-862. http://www.fibroandfatigue.com/files/d-ribose.pdf
Dr. Lapp's list of supplements, including D-Ribose: http://www.prohealth.com/library/showarticle.cfm?libid=16109
Myhill, Sarah, Norman E. Booth, and John McLaren-Howard. “Chronic fatigue syndrome and mitochondrial dysfunction.” Int J Clin Exp Med.2009;2(1): 1–16. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2680051/
(This is a very long paper. You may want to jump to the following site.)
A summary of the information in the previous paper: http://www.drmyhill.co.uk/wiki/CFS_-_The_Central_Cause:_Mitochondrial_Failure
Creatine and D-Ribose studies: http://www.vrp.com/energizers/mitochondrial-restoration-part-iii-d-ribose-and-creatine-increase-mitochondrial-energy-production
A patient's encouraging report of her experiences with D-Ribose. http://www.healingwell.com/community/default.aspx?f=15&m=1253136
DIGESTIVE ENZYMES
DESCRIPTION. Gastrointestinal enzymes are secreted in the GI tract for the purpose of breaking down large food molecules into smaller molecules that are more easily absorbed.
BACKGROUND. Digestive enzymes are secreted in the mouth by salivary glands, in the stomach, in the pancreas and throughout the small intestine. Enzymes are classed into groups according to their function: proteases split proteins into amino acids, lipases split fat into fatty acids and glycerol, carbohydrases split sugars and carbohydrates into glucose, and nucleases split nucleic acids into nucleotides, which form RNA and DNA. Nucleotides also potentiate the production of ATP.
The mouth is where the digestive process is initiated. Enzymes which are released by salivary glands include lingual lipase, to start the digestion of fats; and amylase, which starts the conversion of carbohydrates into glucose; as well as immune system chemicals such as IgA to battle bacterial toxins, and R-factor which helps with the absorption of B12.
The main enzyme produced in the stomach is pepsin, which breaks down proteins. There are a number of other gastric secretions in the stomach which aid the process of breaking down food, the most important of which are hydrochloric
470
acid (HCl ), which activates pepsin and destroys bacteria; intrinsic factor, which aids in the absorption of B12 by protecting it from HCl ; and gastrin, the hormone which stimulates the stomach lining to produce HCl and intrinsic factor.
The pancreas produces trypsin, which further breaks down proteins into amino acids; pancreatic lipase, which breaks down fats; pancreatic amylase, which further breaks down carbohydrates into glucose; protease, for breaking down proteins; and several nucleases.
The small intestines, among many other chemicals, produce sucrase, to break down sugars; lactase, to break down lactose in milk; and maltase, which breaks maltose down into glucose.
USES IN CFS/ME. Given the broad range of GI disturbances in CFS/ME patients, as well as the importance of the GI tract in maintaining both nutritional health and immune system functioning, digestive enzymes can play a critical role in treatment. Dr. Cheney believes enzyme supplementation is essential for all CFS/ME patients.
PROTOCOL. Dr. Cheney recommends one or two tablets of Ultrazyme (made by Douglas Labs). Ultrazyme provides a broad spectrum of enzymes, including lipase, amylase, protease, ox bile extract, cellulase, pepsin and L-lysine. Dr. Myhill recommends Polyzyme Forte, a broad-spectrum enzyme supplement made by BioCare (available the U.K.). Enzymes are sensitive to temperature extremes. They should be taken with warm water or food. Enzymes are activated by moisture, so make sure you keep the tablets dry.
PROS. Many patients swear by enzymes, claiming that they help eradicate digestion problems as well as many food sensitivities.
CONS. Enzymes can be hard on the stomach. For those who are prone to reflux, or heartburn, enzymes may exacerbate these problems. Stomach problems can be mitigated by taking enzymes with food (rather than on an empty stomach).
AVAILABILITY AND COST. Enzymatic supplements are readily available at any health food store and from online suppliers. A 60-tablet bottle of Ultrazyme (Douglas Labs) sells for around $15 on amazon.com. Enzymatic supplements can also be purchased in powder form. Plant-based enzymes, which are not degraded by stomach acid, should always be purchased.
FURTHER READING
Dr. Cheney discusses gut dysbiosis and CFS/ME symptoms: http://www.cheneyclinic.com/gut-dysbiosis-modulates-significant-cfs-symptoms/247
Dr. Cheney discusses Betaine HCl and the function of enzymes. (Written by Carol Sieverling) http://www.prohealth.com/library/showarticle.cfm?libid=8037
Lots of articles about enzymes: http://www.enzymestuff.com/
DHEA
471
NOTE: Not all CFS/ME patients have low levels of DHEA. Before embarking on a course of DHEA, make sure to have your DHEA level tested.
DEFINITION. DHEA (dehydroepiandrosterone) is a naturally occurring adrenal hormone.
BACKGROUND. DHEA, a hormone produced in the adrenal cortex, generates the sex hormones estrogen and testosterone. It is the most common hormone in the blood and is found in greatest concentrations in the brain. Perhaps because DHEA levels decrease with age, it has been called "the fountain of youth." A substantial body of research has provided evidence that DHEA may help the elderly by strengthening bones and muscles, decreasing joint pain, and improving sleep and mood. In addition to influencing hormone production, DHEA has several effects on immune system function, not the least of which is the regulation of lymphokine production.
A study conducted in 1993 by researchers at the University of Tennessee showed that DHEA decreases the amount of circulating interleukin-6 (a potent bone resorber and pro-inflammatory cytokine) and enhances the function of natural killer cells. Another study conducted in 1998 confirmed an inverse correlation between DHEA levels and IL-6 (as DHEA drops, IL-6 increases). DHEA has also been used to treat osteoporosis. A twelve-month study conducted in Canada confirmed that in post-menopausal women the application of DHEA in the form of 10% cream stimulated bone formation.
USES IN CFS/ME. Inspired by mounting evidence of adrenal cortical hypofunction in CFS/ME, clinicians have tested for blood levels of DHEA in CFS/ME patients. Some have discovered lower than normal levels. Based on these results, low doses of DHEA have been administered in hopes of raising immune function and normalizing the metabolic and endocrine disturbances that commonly accompany CFS/ME. It is believed that DHEA could also act as an antiviral agent because testosterone, a DHEA derivative, has demonstrable antiviral effects.
PROTOCOL. The usual dosage of DHEA is 25 to 100 mg/day, although a number of clinicians report good results with smaller doses. Dr. Majid Ali states that he frequently prescribes DHEA in doses of 50 mg taken on alternating days for up to several months. In contrast, Dr. James McCoy found that smaller doses (10 mg or less) are equally, if not more, effective than larger doses (CFIDS Chronicle, Fall 1993). He recommended starting at one tenth the normal dose to minimize the chance of negative reactions. Many patients with CFS/ME confirm that smaller doses (10 mg) work well for them.
PROS. Patients with CFS/ME have reported weight loss, increased energy, improved cognitive function, and better immune system responses with DHEA.
CONS. A number of patients have reported heart palpitations, jitters, and altered mental and emotional states. Female patients have experienced hair loss and acne. Dr. Paul Cheney points out that DHEA is often most beneficial in mild CFS/ME. He notes that even in cases where DHEA deficiency can be documented, administration of this hormone has caused severe relapse in some of his more profoundly ill patients (CFIDS Chronicle, Spring 1995).
472
Researchers have noted side effects in older women given standard doses of DHEA (25-200 mg a day), including acne and hirsutism (facial hair growth). DHEA also lowers cortisol, an anti-inflammatory adrenal hormone responsible for raising blood sugar levels. It is important to remember that even though DHEA is a natural substance, it is still a powerful hormone. Hormones, because they are released directly into the bloodstream, produce profound metabolic effects, not all of which are intended. Like other steroid or hormone treatments, DHEA is not without some risk and must be approached with caution.
AVAILABILITY AND COST. DHEA can be purchased online and at most health food stores. It is inexpensive. Vitacost sells many brands for less than $10. Mexican wild yam products containing diosgenin should be avoided, as the body cannot convert diosgenin to DHEA.
Although DHEA is sold as a supplement in the U.S., it cannot be purchased in the U.K. and Canada without a prescription. South Dakota and Missouri prohibit the sale of DHEA. Those under the age of 18 cannot purchase DHEA without a prescription. Most bottles of DHEA contain the warning: “Not for women under the age of 35.”
One of the natural precursors to DHEA, pregnenolone, may be less risky than DHEA. Patients report increased energy, enhanced mental clarity, and general improvement after taking pregnenolone. The dosage is 10 mg every other day in patients younger than 50 years, and 20 mg every other day in patients over 50 years old. Pregnenolone can be purchased from online suppliers at roughly the same cost as DHEA. Pregnenolone carries the same warnings as DHEA.
FURTHER READING
Very thorough overview of DHEA. Many studies are cited. http://www.tidesoflife.com/dhea__basic_information.htm
Dr. Cheney on DHEA and other supplements (1995). http://www.immunesupport.com/news/95sum003.htm
Good article on the effects of DHEA on aging: http://www.anti-agingmd.com/dhea.html
PATIENT REVIEWS
CFS/ME patient reviews of DHEA: http://www.revolutionhealth.com/drugs-treatments/rating/dehydroepiandrosterone-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Casson PR, Andersen RN, Herrod HG, Stentz FB, Straughn AB, Abraham GE, Buster JE. “Oral dehydroepiandrosterone in physiologic doses modulate immune function in postmenopausal women.” Am J Obstet Gynecol. 1993 Dec;169(6):1536-9. http://www.ncbi.nlm.nih.gov/pubmed/8267058 (Abstract)
Labrie F, Diamond P, Cusan L, Gomez JL, Bélanger A, Candas B. "Effect of 12-Month Dehydroepiandrosterone Replacement Therapy on Bone, Vagina, and
473
Endometrium in Postmenopausal Women." J Clin Endocrinol Metab. 1997 Oct;82(10):3498-505. http://jcem.endojournals.org/content/82/10/3498.short (Abstract)
ESSENTIAL FATTY ACIDS
Fish Oil, Flaxseed Oil, Evening Primrose Oil, Borage Seed Oil
DESCRIPTION. Essential fatty acids are fats (lipids) that are important in a number of physiological processes. They cannot be produced by the body and therefore must be obtained through dietary sources.
BACKGROUND. The two most important types of essential fatty acids are omega-3 and omega-6. Omega-3 fatty acids – alpha linolenic acid (ALA), docosahexanoic acid (DHA), and eicosapentaenoic (EPA) – are found in fish oil (especially cold water fish) and flaxseed oil. Omega-6 fatty acids (linoleic acid, LA) are found in many plant oils, including evening primrose oil, borage oil, and black currant oil.
Essential fatty acids are vital to a number of physiological processes, such as regulating cholesterol levels, keeping the skin moist and supple, and producing prostaglandins (hormone-like substances that affect a variety of body functions). Essential fatty acids are also indispensable in maintaining the structure and function of cell membranes. Most important, essential fatty acids, particularly those found in fish oil, can act as immune system modulators, enhancing immune system activity where needed, and inhibiting it when there is an upregulated immune response.
Several factors can affect fatty acid metabolism. Poor diet, stress, diabetes, excessive alcohol intake, radiation, and viral infections can disrupt the metabolism of essential fatty acids, making it difficult for the body to produce fatty acid metabolites in sufficient quantities. In such cases, supplementation may be necessary to prevent deficiency states. Supplementation with essential fatty acids has improved such diverse conditions as premenstrual syndrome (PMS), heart disease, rheumatoid arthritis, multiple sclerosis, hyperactivity in children, depression and mononucleosis.
USES IN CFS/ME. In 1987 Dr. Peter Behan, a professor of Clinical Neurology in Glasgow, Scotland, found that patients with CFS/ME have a disorder in fatty acid metabolism. Dr. Behan surmised that the disorder was the result of chronic viral infection much like mononucleosis, a prolonged illness that also produces abnormal serum fatty acid concentration. He conducted a double-blind trial using a fatty acid supplement (Efamol) containing both omega-3 and omega-6 fatty acids (Acta Neurologica Scandinavica, 1990). After 16 weeks of treatment, an astounding 85% of patients showed marked improvement, primarily in the areas of fatigue, dizziness, headaches, depression, and muscle pain.
In 1994, Gray and Martinovic hypothesized that the chronic immune system activation found in CFS/ME patients results in hyporesponsiveness of essential
474
fatty acid metabolites, which produces a state in which even minor stressors can disturb homeostasis. They tested their hypothesis by administering dietary essential fatty acids to a group of CFS/ME patients. After three months, 90% of the patients treated showed signs of improvement.
While the results of Behan's and Gray's studies were encouraging, not all studies have confirmed that the administration of EFAs significantly improves CFS/ME symptoms. It wasn't until specific EFAs were tested that some light was shed on the effects of EFA supplementation in CFS/ME.
In 2003 Liu et al measured specific EFAs in the red blood cells of CFS/ME patients. The researchers found that both DHA and ARA (arachidonic acid) levels were low, indicating a state of oxidative stress. The authors concluded that because ratios of EFAs are essential in maintaining signal transduction, the disruption in EFA ratios might induce an impairment in both circulation and immune system function. The authors stated that recurrent sore throat, tender lymph nodes, muscle aches, arthralgia, and headaches might be due to disruption in EFA signaling.
Puri's 2004 study of eicosapentaenoic acid (EPA) showed that it was the omega-3 fatty acids that produced the greatest improvement in CFS/ME symptoms. Four patients with chronic, intractable CFS/ME were treated with high doses (approx 1500 mg a day) of an over-the-counter high eicosapentaenoic acid fatty acid supplement (Equazen, Ltd., London). All four patients showed improvement in symptoms within 12 weeks of treatment. They reported a lessening of “brain fog,” and an overall sense of well-being. The same patients when treated with a placebo did not note a similar improvement. While the cohort was small, the findings of this study were significant.
On the heels of this study, in 2005 Maes et al studied the ratios of fatty acids in CFS/ME patients. The researchers measured omega-6 and omega-3 fatty acid ratios in 22 CFS/ME patients and 12 controls. They found that CFS/ME patients, regardless of age or gender, had significantly higher levels of linoleic acid and arachidonic acid (omega-6) than controls. Both linoleic acid and arachidonic acid are implicated in the production of pro-inflammatory cytokines. They speculated that the low levels of circulating zinc found in CFS/ME patients (indicating an inflammatory response) might be due to the depletion of omega-3 fatty acids. The authors further hypothesized that the defects in T cell activation found in CFS/ME might also be attributed to a deficit in omega-3 fatty acids.
AVAILABILITY AND COST. EFAs are available at any health food store and through online suppliers. Many companies sell combinations of different EFAs for maximum effect. Because these are oils which are highly prone to rancidity, it is worth the price to buy a high quality product.
FURTHER READING
“The ABCs of EFAs.” CFIDS Chronicle, Summer 2008. http://www.cfids.org/cfidslink/2009/040107.pdf
Good summary of essential fatty acids, their function, and their role as a treatment for CFS/ME.
475
RESEARCH
Gray JB, AM Martinovic. “Eicosanoids and essential fatty acid modulation in chronic disease and the chronic fatigue syndrome.” Medical Hypotheses; Vol 43, Issue 1, July 1994, Pages 31-42 http://www.ncbi.nlm.nih.gov/pubmed/7968718 (Abstract)
Liu, Zhandong, Dexin Wang, Qiming Xue, Jun Chen, Yongjie Li, Xiaoli Bai, and Liwen Chang. “Determination of Fatty Acid Levels in Erythrocyte Membranes of Patients with Chronic Fatigue Syndrome.” Nutritional Neuroscience, Volume 6 Number 6 (December 2003), pp. 389–392. http://www.cfids-cab.org/cfs-inform/Hypotheses/liu.etal03.pdf
Maes, Michael, Ivana Mihaylova and Jean-Claude Leunis. “In chronic fatigue syndrome, the decreased levels of omega-3 poly-unsaturated fatty acids are related to lowered serum zinc defects and defects in T cell activation.” Neuroendocrinology Letters; No 6, December, Vol 26, 2005. http://www.nel.edu/26-2005_6_pdf/NEL260605A22_Maes.pdf
Ninjs, Jo, and Kenny De Meirleir. “Letter to the Editor: Oxidative Stress Might Reduce Essential Fatty Acids in Erythrocyte Membranes of Chronic Fatigue Syndrome Patients.” Nutritional Neuroscience, Volume 7 Number 4 (August 2004), pp. 251–253 http://cfids-cab.org/cfs-inform/Hypotheses/nijs.demeirleir04.pdf
Puri BK. “The use of eicosapentaenoic acid in the treatment of chronic fatigue syndrome.” Prostaglandins Leukot Essent Fatty Acids. 2004 Apr;70(4):399-401. http://www.cfids-cab.org/cfs-inform/CFStreatment/puri04.pdf
FISH OILS
DESCRIPTION. The oil derived from deep-sea fish (sardines, mackerel, salmon, and herring) is the richest source of omega-3 fatty acids (DHA and EPA). Four ounces of salmon can contain as much as 3600 mg of omega-3 fatty acids. Fish oil capsules have been particularly helpful in treating fibromyalgia, often providing immediate relief from pain. Fish oil is so effective that some physicians suggest it in place of Advil (ibuprofen) for pain from inflammation. Because of its anti-inflammatory properties, fish oil can also be used to treat arthritis and colitis.
AVAILABILITY AND COST. High-quality brands of fish oils are available from Kyolic and Cardiovascular Research Ltd. Plain cod liver oil is not recommended because the amount needed to provide sufficient fatty acids might lead to an overdose of vitamin A. Fish oils can range in price from $5 to $15 for a month's supply, depending on the brand, and can be purchased in health food stores or through online vitamin catalogs. The usual dose is one to four capsules a day.
For those who experience stomach upset with fish oil, the enteric-coated version, Fisol (made by Nature's Way), may be preferred. The enteric coating allows the capsules to pass through the stomach, dissolving only once they reach the intestines. One capsule of Fisol provides 500 mg of omega-3 fatty acids. Vitacost sells a 180-capsule bottle of Fisol for $16.
476
PATIENT REVIEWS
CFS/ME patient reviews of fish oil: http://www.revolutionhealth.com/drugs-treatments/rating/fish-oil-omega-3-epa-dha-fatty-acids-for-chronic-fatigue-syndrome-cfs-cfids-me
FLAXSEED OIL
DESCRIPTION. Flaxseed (linseed) is a good plant source of omega-3 fatty acids. It is also high in magnesium and zinc, two important factors in fatty acid metabolism, as well as B complex vitamins, protein, and potassium. Flaxseed oil is low in saturated fat and calories and contains no cholesterol. It has a delicious nutty flavor and can be added to salad dressings or sprinkled over vegetables.
Flaxseed is high in alpha-linoleic acid (ALA), which the body converts to eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), the two fatty acids found in fish oils. Some clinicians prefer flaxseed oil to fish oil because it is lower on the food chain and thus contains fewer fat-soluble contaminants. Fish oils, as opposed to vegetable oils, also contain large quantitites of vitamin A, which can be toxic in excessive amounts.
AVAILABILITY AND COST. Flaxseed oil can be purchased in health food stores and is inexpensive. NOW markets a 24-ounce bottle of organic flaxseed oil for $9. Flaxseed oil must be stored in the refrigerator to avoid rancidity. It should not be used for cooking. Gelcaps are also available.
PATIENT REVIEWS
CFS/ME patient ratings for flaxseed oil: http://www.revolutionhealth.com/drugs-treatments/rating/flax-seed-oil-omega-3-alpha-linolenic-acid-for-chronic-fatigue-syndrome-cfs-cfids-me
EVENING PRIMROSE OIL
DESCRIPTION. Evening primrose oil is one of the most popular and perhaps most effective of the omega-6 essential fatty acids. It comes from the evening primrose (Oenothera), a lovely yellow flower that grows wild along roadsides. The seeds contain large amounts of GLA (gamma-linoleic acid), a linoleic acid metabolite. Unlike other omega-6 fatty acids, GLA does not lead to increased production of pro-inflammatory cytokines, but has an anti-inflammatory effect. Evening primrose oil has been used to help alleviate the symptoms of premenstrual syndrome (PMS), menstrual cramps, and arthritis, often with dramatic results. It may even lessen the symptoms of endometriosis.
PROS AND CONS. Patients with CFS/ME have reported increased energy, improvements in skin disorders (eczema, acne, dry skin), and decreased mood swings. Side effects, although uncommon, include headache, nausea, mild intestinal discomfort, and, rarely, weight gain.
477
AVAILABILITY AND COST. Evening primrose oil capsules are relatively inexpensive. A bottle of 60 softgels can be purchased for under $10 from online distributors.
PATIENT REVIEWS
CFS/ME patient ratings of evening primrose oil: http://www.revolutionhealth.com/drugs-treatments/rating/vitamin-c-ascorbic-acid-for-chronic-fatigue-syndrome-cfs-cfids-me
BORAGE SEED OIL
DESCRIPTION. Borage seed oil, made from the borage plant, contains the highest GLA content of any currently available seed oil, up to four times more than the GLA content of evening primrose oil. Patients who have gained little benefit from or cannot tolerate evening primrose oil because of food sensitivities often take borage oil with good results. The recommended dose is lower than for evening primrose oil, only one to three capsules a day. As with all EFAs, it is best to purchase products that are high quality. Pureformulas.com markets a bottle of 30 softgels made by Allergy Research Group for $14.
FOS (Fructooligosaccharides)
DESCRIPTION. FOS (Fructooligosaccharides) are natural sugars derived from fruits and vegetables.
BACKGROUND. FOS is produced from the degradation of inulin, or polyfructose. It is roughly half as sweet as sugar. FOS has achieved popularity as a “prebiotic,” something that provides a necessary substrate for lower intestinal flora, particularly bifidobacteria. FOS also helps increase the absorption of calcium and magnesium.
USES IN CFS/ME. FOS is primarily used in conjunction with probiotics to aid in the promotion of friendly gut bacteria.
Opinions about FOS are mixed in the CFS/ME community. Dr. Cheney, for example, is not a fan of FOS. In a 1999 talk about CFS/ME patients with leaky gut, he likened FOS to “throwing fertilizer on a patch of weeds.” By this, he is referring to the fact that FOS, like other prebiotics, will nourish harmful bacteria as well as friendly bacteria. In the presence of a bacterial infection in the gut or SIBO (small intestine bacterial overgrowth), prebiotics such as FOS will only make the condition worse. Dr. Myhill, on the other hand, recommends supplementation for FOS to help replenish friendly flora.
PROTOCOL. The normal dose is ¼ to 1 teaspoon of powder, taken 2 -3 times daily, in divided doses, with or between meals. FOS is sweet, so it can be used in place of sugar.
PROS AND CONS. There is not much patient feedback on FOS. In small amounts it does not cause side effects. If too much is taken, it can cause gas. Because FOS provides a substrate for all bacteria, it should not be taken in the presence of intestinal bacterial infections (such as C diff or SIBO).
478
AVAILABILITY AND COST. FOS is available at health food stores and from online distributors. It can be purchased in capsules, tablets, or in a powder. Most health care practitioners recommend the powder, as it can be more easily titrated. PureFormulas.com markets a 100-gram container of FOS made by Pure Encapsulations for about $14. (At 1 teaspoon a day, a 100-gram container will last a month.) There are many probiotic/FOS combinations on the market.
GABA
DESCRIPTION. GABA (gamma aminobutyric acid) is the chief neuroinhibitory neurotransmitter in mammals. While GABA is commonly referred to as an amino acid, it is not incorporated into proteins.
BACKGROUND. Although GABA was first synthesized in the 19th century, it wasn't until 1950 that it was first discovered to be a central component of the nervous system of mammals. GABA is synthesized in the brain from glutamate, a neuroexcitatory neurotransmitter, through the enzyme L-glutamic acid decarboxylase in conjunction with the active form of vitamin B6. GABA's main function in the brain is to balance neuroexcitatory neurotransmitters by preventing nerves from excessive firing. There are many pharmaceuticals that act on GABA receptors, including anti-anxiety medications, anti-seizure medications, and pain medications. Valerian, skullcap, kava and L-theanine are supplements that act on GABA receptors.
USES IN CFS/ME. GABA has not been widely investigated in CFS/ME patients. Kowalski et al proposed that decreased activity of the enzymes which produce GABA may be the cause of several disorders, including CFS/ME. However, Murrough et al did not find any significant decrease in GABA itself among CFS/ME patients. In contradiction to Murrough's findings, McGregor et al found decreased beta-alanine (a GABA analogue) in CFS/ME patients, correlating with symptoms. However, Theodorsson et al found that while there was abnormal excretion of beta-alanine in CFS/ME patients, it did not correlate with symptoms. Notwithstanding this collection of contradictory evidence, it has long been proposed that people with CFS/ME suffer from neuroexcitatory states corresponding to an upregulated immune system.
Some CFS/ME doctors recommend GABA for their patients who experience anxiety and/or insomnia. Because GABA does not easily cross the blood-brain barrier, most physicians prefer to use pharmaceutical analogues such as Neurontin.
PROTOCOL. Dr. Rosenbaum recommends 500-1500 mg of GABA to his patients with insomnia.
PROS AND CONS. Given its inability to cross the blood-brain barrier, there is some doubt as to whether taking GABA supplements has any effect at all on the nervous system. But putting scientific skepticism aside, some patients report that it makes them jittery the day after using it for insomnia, which means it has some ability to affect the brain.
AVAILABILITY AND COST. GABA is sold in health food stores and from online suppliers. It is relatively inexpensive, and is available in pill, sublingual and
479
powder form. The sublingual form is supposed to provide the greatest calming effect.
RESEARCH
Hannestad U, Theodorsson E, Evengård B. “Beta-Alanine and gamma-aminobutyric acid in chronic fatigue syndrome.” Clinica Chimica Acta. 2007 Feb;376(1-2):23-9. http://www.cfids-cab.org/cfs-inform/Hypotheses/hannestad.etal.06.txt
Kowalski A, Rebas E, Zylińska L. [Gamma-aminobutyric acid--metabolism and its disorders].Postepy Biochem. 2007;53(4):356-60. http://www.ncbi.nlm.nih.gov/pubmed/19024900 (Abstract)
McGregor NR, Dunstan RH, Zerbes M, Butt HL, Roberts TK, Klineberg IJ. “Preliminary determination of a molecular basis of chronic fatigue syndrome.” Biochem Mol Med. 1996 Apr;57(2):73-80. http://www.ncbi.nlm.nih.gov/pubmed/8733884 (Abstract)
Murrough JW, Mao X, Collins KA, Kelly C, Andrade G, Nestadt P, Levine SM, Mathew SJ, Shungu DC. “Increased ventricular lactate in chronic fatigue syndrome measured by 1H MRS imaging at 3.0 T. II: comparison with major depressive disorder.” NMR Biomed. 2010 Jul;23(6):643-50. http://www.ncbi.nlm.nih.gov/pubmed/20661876 (Abstract)
GALANTAMINE
DESCRIPTION. Galantamine is a selective acetylcholinesterase inhibitor.
BACKGROUND. Galantamine has been used for decades in Eastern Europe for various central nervous system disorders, including post-polio paralysis and myasthenia gravis. It was originally derived from the Galanthus Caucasicus (Caucasian snowdrop), whose nodding white blooms are among the first to appear in the spring. Recently, a synthetic compound, galantamine hydrobromide (brand name: Razadyne), was approved by the FDA as a treatment for Alzheimer's disease. Because galantamine increases acetylcholine, it has also been used to block the effects of nerve gas and organophosphate pesticides, which operate by blocking acetylcholine.
Chemically, galantamine reduces the action of acetylcholinesterase (AchE), the enzyme that breaks down acetylcholine. Galantamine also modulates nicotinic cholinergic receptors, which acts to increase the release of acetylcholine.
USES IN CFS/ME. The first study to test galantamine as a treatment for CFS/ME was conducted in 1996 by a team composed of Dr. Ernir Snorrason, Dr. Arni Geirsson and Dr. Kari Stefansson. Their hypothesis was that a dysfunction of the cholinergic system lay at the heart of CFS/ME. The researchers tested their hypothesis by administering galantamine hydrobromide to 39 CFS/ME patients.
The results were impressive; 43% reported an 50% improvement in fatigue, pain and sleep. The authors noted that the improvement was stable, and that none of the patients who had reported 50% improvement relapsed after the cessation of the trial. Most dramatic was the improvement in sleep. More than 60% of the patients who finished the study reported a 70% improvement of sleep disturbances.
480
Given the striking results of this study, it is puzzling that there was so little follow-up. In 2009 Turan et al investigated the effects of galantamine on stress hormones in a group of CFS/ME patients. The study found that DHEAS/cortisol ratios normalized with galantamine treatment. But, while the findings confirmed a cholinergic deficit in CFS/ME, there have been no further treatment studies.
PROTOCOL. There is no protocol for galantamine. The Snorasson group used several different doses, but even at the lowest dose (5 mg) several patients developed severe nausea. High doses caused hallucinations, sweating, diarrhea, vomiting and confusion. Even though the side effects passed, Snorasson's group recommended starting with very low doses and close monitoring by a physician. They also recommended taking galantamine several hours before bed so as to reduce the risk of nightmares. Galantamine should be taken with choline.
AVAILABILITY AND COST. Galantamine is in the unusual class of medications that are both prescription drugs and supplements. (Even more confusing, nobody seems to know if there is a difference between the two.)
Galanta Mind, a blend of 4 mg galantamine hydrobromide, choline and B6 made by Life Enhancement, is available from such diverse sources as amazon.com, iHerb, and Sears. A 90-capsule bottle costs between $40 and $57, depending on the supplier. The manufacturer cautions that galantamine is for adults only. Instructions on the bottle read: “Start with one capsule each morning with breakfast for the first week. Add a second capsule with lunch, starting the second week. If desired, add another capsule to the breakfast serving the third week. Then, if desired, add another capsule to the lunch serving the fourth week, for a total of four capsules per day. If sensitivity occurs, reduce the amount used. If sensitivity continues, stop taking this supplement.”
FURTHER READING
“If Only Galantamine Could Talk.” Great summary of galantamine's fascinating history as well as its medicinal properties: http://www.life-enhancement.com/article_template.asp?ID=973
“Can Galantamine Help Chronic Fatigue?” Article on acetylcholine deficiency in CFS/ME patients. http://www.life-enhancement.com/article_template.asp?id=2224
Ray Sahelian discusses galantamine: http://www.raysahelian.com/galantamine.html
RESEARCH
Snorrason E, Geirsson A, Stefansson K. “Trial of a selective acetylcholinesterase inhibitor, galanthamine hydrobromide, in the treatment of chronic fatigue syndrome.” Journal of Chronic Fatigue Syndrome 1996; 2(2/3): 35-54. http://www.hfme.org/researchmisc.htm (Scroll down for abstract.)
Spence VA, Khan F, Kennedy G, Abbot NC, Belch JJF. “Acetylcholine mediated vasodilatation in the microcirculation of patients with chronic fatigue syndrome:
481
a short review.” http://www.meresearch.org.uk/research/reviews/ach_review.html
Turan T, Izgi HB, Ozsoy S, Tanrıverdi F, Basturk M, Asdemir A, Beşirli A, Esel E, Sofuoglu S. “The effects of galantamine hydrobromide treatment on dehydroepiandrosterone sulfate and cortisol levels in patients with chronic fatigue syndrome.” Psychiatry Investig. 2009 Sep;6(3):204-10. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2796068/
GLUCOSAMINE SULFATE
DESCRIPTION. Glucosamine sulfate is a mucopolysaccharide made up of the sugar glucose and the amino acid glutamine. It is the synthetic form of glucosamine, a naturally occurring amino acid compound found in the joints.
BACKGROUND. Glucosamine sulfate has been used for many years in Europe, Asia, and the Philippines to treat osteoarthritis. It appears to stimulate the synthesis of connective tissue and cartilage by aiding in the production of glucosaminoglycans and proteoglycans, the key building blocks of cartilage. Because glucosamine is also one of the main components of the synovial fluids that cushion joints and surrounding tissues, it has been used to treat degenerative joint diseases. It also may have anti-inflammatory properties, thereby lessening the need for anti-inflammatory pain medications.
USES IN CFS/ME. It is difficult to determine how useful glucosamine may be for people with CFS/ME. Its mode of action indicates that, in theory, it may be of benefit to patients with joint pain, fibromyalgia, or interstitial cystitis.
PROTOCOL. Dr. Jason Theodasakis, author of The Arthritis Cure, suggests taking glucosamine sulfate with chondroitin, another mucopolysaccharide, for maximum benefits. His daily dosage recommendations are based on patient weight:
Less than 120 pounds: 1000 mg glucosamine sulfate plus 800 mg chondroitin
120 to 200 pounds: 1500 mg glucosamine sulfate plus 1200 mg chondroitin
200 pounds or more: 2000 mg glucosamine sulfate plus 1600 mg chondroitin
Other health care providers believe glucosamine sulfate is effective alone, although some recommend the addition of bromelain, an enzyme derived from pineapple, to help maximize its effects. Standard adult dosage as indicated by the manufacturer is one or two tablets three times a day. Health effects should be noticed within six to eight weeks. If no benefits are apparent by then, glucosamine sulfate should be discontinued.
PROS AND CONS. Glucosamine sulfate is generally considered safe and is well tolerated by most patients. However, some may be allergic to its source (usually crustacean shells). Patients taking blood thinners should consult with their physician before taking glucosamine sulfate because many of the mucopolysaccharides inhibit platelet formation.
AVAILABILITY AND COST. Glucosamine sulfate is available from health food stores and online distributors. A bottle of 120-tablets or capsules usually costs between $12 and $15. Glucosamine sulfate is also available in liquid form.
FURTHER READING
482
Results of a comprehensive multi-center investigation of glucosamine chondroitin. http://nccam.nih.gov/research/results/gait/qa.htm
GLUTATHIONE
DESCRIPTION. Glutathione is a tripeptide composed of glycine, cysteine, and glutamic acid.
BACKGROUND. Glutathione is found in high concentrations in every tissue in the body. It is one of the three most powerful antioxidants and detoxification agents in the body, protecting tissues against damage from oxygen radicals such as hydrogen peroxide and superoxide. It also helps reduce injury caused by radiation, chemotherapy, heavy metals (mercury), and drugs (including cigarettes and alcohol). NAC (N-acetyl-L-cysteine), a precurser to glutathione, is an antidote to acetaminophen poisoning and helps deter the toxic effects of naphthalene, benzene, and anthracine. Low glutathione levels are associated with cataracts and muscle wasting diseases.
USES IN CFS/ME. A relationship between glutathione, muscle fatigue, low natural killer (NK) cell activity and CFS/ME was first proposed in 1997 by Droge and Holm, two scientists researching HIV in Heidelberg, Germany. Notably, Droge and Holm suggested cysteine supplementation as an adjunct to antiviral therapies to correct low glutathione. Expanding on their idea in 1999, two researchers at McGill University proposed that competition for glutathione between the immune system and skeletal muscles might be the cause of fatigue, muscle weakness, and pain in CFS/ME patients. More recently, Shungu et al found that glutathione levels were low in the cerebrospinal fluid of CFS/ME patients.
Dr. Patricia Salvato of Houston, Texas, reported in the CFIDS Chronicle (Jan/Feb 1998) that she had treated 276 CFS/ME patients with glutathione injections. Eighty-two percent of her patients experienced improvement in fatigue, 71 % reported improvement in memory and concentration, and 62% reported reduced pain. Natural killer cell function was also measured, with 187 people showing a two-fold increase. Some patients received the therapy for as long as 16 months. The only adverse side effects observed were palpitations in a few patients and a slight rash or itching around the site of injection.
Dr. Paul Cheney, who at one time stated that glutathione deficiency was universal among CFS/ME patients, has noted a striking improvement in his patients' symptoms, especially headache, within days of initiating glutathione treatment.
PROTOCOL. Because oral glutathione is poorly absorbed in the gut, Dr. Cheney recommends reduced glutathione (CFIDS Chronicle, Spring 1995). Initial doses are high, from 150 to 425 mg three times a day. After a short time, doses can be reduced to 75 to 150 mg three times a day and maintained at those levels. Glutathione can also be administered IV.
AVAILABILITY AND COST. There is no way of knowing how much, in any, glutathione is absorbed by mouth, so injectable forms are preferred. (These require a doctor.) Alternative forms of glutathione (suppositories and troches) may have
483
greater absorption rates. A pack of 30 Zetpil glutathione suppositories are available through Forrest Health for $99. Glutathione troches are available through compounding pharmacies.
In part because glutathione is so difficult to administer effectively, a synthetic glutathione peroxidase mimic, ebselen, has been developed. Initial studies demonstrated that ebselen was effective in protecting against chemotherapy-induced hearing loss, renal injury and in recovery from stroke (if administered within 24 hours). Ebselen protects against manganese toxicity, inhibits Candida overgrowth, and performs a host of antioxidant activities. Ebselen has been licensed in the U.K. for treatment of ischemic stroke. It has not yet been approved by the FDA.
FURTHER READING
Rich Van Konynenburg's excellent review of glutathione, including protocols, dosages, suppliers. http://aboutmecfs.org.violet.arvixe.com/Trt/TrtGlutathioneBuild.aspx
Another excellent discussion by Rich Van Konynenburg proposing glutathione depletion as a cause of CFS/ME: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=1287095
A list of articles about glutathione written by Rich Van Konynenburg. http://forums.phoenixrising.me/showthread.php?12927-Documents-by-Rich-Van-Konynenburg
An interesting, if somewhat convoluted, discussion of glutathione and its role in CFS/ME. http://user.xmission.com/~total/temple/Soapbox/Articles/glutathione.html
Ray Sahelian discusses glutathione's role in various disease processes. Some good research citations. http://www.raysahelian.com/glutathione.html
Glutathione suppositories: http://www.forresthealth.com/reduced-glutathione-suppositories-30-count.html
RESEARCH
Bounous G, Molson J. “Competition for glutathione precursors between the immune system and the skeletal muscle: pathogenesis of chronic fatigue syndrome.” Med Hypotheses 1999 Oct;53(4):347-9. http://www.ncbi.nlm.nih.gov/pubmed/10608272 (Abstract)
Droge W, and Holm E. “Role of cysteine and glutathione in HIV infection and other diseases associated with muscle wasting and immunological dysfunction.” FASEB J. (1997) 11:1077-1089. http://www.fasebj.org/content/11/13/1077
Maes M, Mihaylova I, Kubera M, Uytterhoeven M, Vrydags N, Bosmans E. “Lower whole blood glutathione peroxidase (GPX) activity in depression, but not in myalgic encephalomyelitis / chronic fatigue syndrome: another pathway that may be associated with coronary artery disease and neuroprogression in depression.” Neuro Endocrinol Lett. 2011;32(2):133-40. http://www.ncbi.nlm.nih.gov/pubmed/21552194 (Abstract)
484
Nakamura, Yoshimasa, Qing Feng, Takeshi Kumagai, Koji Torikai, Hajime Ohigashi, Toshihiko Osawa, Noriko Noguchi, Etsuo Niki, and Koji Uchida. “Ebselen, a Glutathione Peroxidase Mimetic Seleno-organic Compound, as a Multifunctional Antioxidant: Implication for Inflammation-Associated Carcinogensis.” The Journal of Biological Chemistry, January 25, 2002, 277, 2687-2694. http://www.jbc.org/content/277/4/2687 (Abstract)
Shungu DC, Weiduschat N, Murrough JW, Mao X, Pillemer S, Dyke JP, Medow MS, Natelson BH, Stewart JM, Mathew SJ. “Increased ventricular lactate in chronic fatigue syndrome. III. Relationships to cortical glutathione and clinical symptoms implicate oxidative stress in disorder pathophysiology.” NMR Biomed. 2012 Jan 27. http://www.ncbi.nlm.nih.gov/pubmed/22281935 (Abstract)
HERBS
Aloe vera, Astragalus, Chamomile, Echinacea, Garlic, Ginger, Gingko, Ginseng, Goldenseal, Gotu kola, Kava, Licorice, Lomatium, Milk Thistle, St. John's Wort, Uva ursi, Valerian
DESCRIPTION. Medicinal herbs are plants taken orally as teas or tinctures, or applied topically as poultices in order to heal the body.
BACKGROUND. Plants have always been used as remedies, which makes herbal treatment the earliest form of medicine. (The earliest human graves contain remnants of medicinal flowers.) Even animals eat certain plants when they become ill. Throughout the ages, people have used herbal remedies for an assortment of problems and, until the nineteenth century, herbs were the treatment of choice for most common ailments. Herbs have such a long history they are regarded as folk remedies. The contemporary medical world, as a consequence, has largely excluded them from scientific investigations, with the exception of the Chinese, who take herbs quite seriously. The government of China has funded a considerable amount research to study the chemical components, action, and efficacy of a number of herbs.
USES IN CFS/ME. A large number of patients with CFS/ME symptoms use herbs regularly, either as herbal substitutes for pharmaceuticals or as adjuncts to other therapies. Although many find that a particular herb is helpful for a specific symptom, most report that herbs have limited value in treating CFS/ME over the long term. It should be noted, however, that patients who have tried Chinese herbs (usually on the recommendation of an acupuncturist) generally report a higher rate of success.
PROTOCOL. Although herbalists recommend blending herbs for maximum effect, patients with CFS/ME frequently have had poor responses to multiple-herb blends (with the notable exception of Chinese herbs). For CFS/ME symptoms, herbs are best taken singly in teas or tinctures. Teas are prepared according to the part of the plant used. One teaspoon of herb leaves is steeped in two cups of boiling water for 15 or 20 minutes or ½ teaspoon of herb root or bark is boiled in two cups of
485
water. One to two cups of tea per day can be taken for up to two weeks. After that, the herb loses its potency. Tinctures are usually purchased from health food stores. Because they are quite strong, tinctures are usually taken a few drops at a time in water. For chronic symptoms, teas are advised. Short-term problems (flu, toothache, etc.) are best treated with tinctures.
Note: Most tinctures are prepared in an alcohol medium. People with CFS/ME are advised to "flash off" the alcohol by adding the tincture to scalding hot water.
PROS AND CONS. Herbs are inexpensive, safe, and readily available. However, it is always best to purchase them from a health food or specialty store. Culinary herbs from the grocery store are usually treated with chemical preservatives, seldom organic, and have little medicinal worth. The advantage of herbs for many people with drug and chemical sensitivities is that they can produce the desired therapeutic effects without as many side effects. This is not to say that negative reactions are not possible. People with bladder problems (interstitial cystitis), gastrointestinal symptoms, or migraine headaches may find that many herbs produce the same side effects as pharmaceuticals.
In general, patients with CFS/ME should avoid herbs classified as stimulants (ephedra, lomatium, and ginseng), because these can overtax the adrenal glands. Ephedra (ma huang), used to treat bronchial infections, is a powerful stimulant and can cause high blood pressure, palpitations, and even stroke. Ginseng and lomatium, although not as strong as ephedra, can produce similar reactions in the severely ill. Echinacea, because it is an immune system stimulant, might best be avoided by those with upregulated immune systems.
Some herbs such as goldenseal and St. John's Wort must be used with caution. St. John's Wort acts like a monoamine oxidase inhibitor (MAOI) and must be treated with the same care as the drug. (The newsletter of the Center for Specialized Immunology reported a serious reaction in a patient who took St. John's Wort concomitantly with an antidepressant.)
Chapparal and comfrey have caused liver problems in some people who took too high a dose. However, there are many other herbs that can provide temporary, safe relief from numerous CFS/ME symptoms. Those interested in pursuing herbal remedies should read about herbs before embarking on an herbal therapy program or should consult with an herbalist.
FURTHER READING
Dr. Teitelbaum's herb recommendations for CFS/ME patients. http://www.immunesupport.com/news/99spr012.htm
Nicely organized site about herbs. Herbs are listed alphabetically for easy access. http://www.herbwisdom.com/
BOOK
Castleman, Michael. The Healing Herbs. Emmaus, Pa.: Rodale Press, 1991
This is a well-organized introduction to herbs and their uses.
486
ALOE VERA
Aloe vera is a succulent plant originating in Africa. Because it exudes a mucousy substance when cut, it has a long history as a topical treatment for minor burns. More recently, aloe juice has been promoted as an immune enhancer and as a treatment for cancer. Though research has not been able to substantiate these claims, aloe vera juice is recommended for people with a variety of immune system ailments.
While some people with CFS/ME have taken aloe and been pleased with the results, there are more negative than positive reviews. Although it is touted as a cure for IBS, aloe vera can cause diarrhea and intestinal irritation even in very small amounts.
FURTHER READING
General information about aloe vera: http://www.herbwisdom.com/herb-aloe-vera.html
CFS/ME patient reviews of aloe vera: http://www.revolutionhealth.com/drugs-treatments/rating/aloe-vera-aloe-barbadensis-for-chronic-fatigue-syndrome-cfs-cfids-me
ASTRAGALUS
Astragalus (Astragalus membranaceous) root has been popularized as an immune system modulator. It reputedly enhances immune system function when it is deficient and down regulates it when overactive. It is also thought to increase energy, stamina, and well-being and supports adrenal gland function. Some use it as a digestive aid. The effects of astragalus are not dramatic in most people, but some CFS/ME patients have noted increased energy after taking tincture of astragalus.
Recent research has shown that astragalus has measurable medicinal properties. A 2011 study by Cheng et al showed that astragalus may serve as a natural cholesterol-lowering agent. Astragalus has also been shown to enhance both humoral and cellular immune response (Th1 and Th2).
FURTHER READING
General information about astragalus http://www.immunesupport.com/news/98spr007.htm
More general information about astragalus: http://www.herbwisdom.com/herb-astragalus.html
RESEARCH
Cheng Y, Tang K, Wu S, Liu L, Qiang C, Lin X, Liu B. “Astragalus Polysaccharides Lowers Plasma Cholesterol through Mechanisms Distinct from Statins.” PLoS ONE. 2011;6(11):e27437. http://www.ncbi.nlm.nih.gov/pubmed/22110652 (Abstract)
487
Du X, Chen X, Zhao B, Lv Y, Zhang H, Liu H, Chen Z, Chen Y, Zeng X. “Astragalus polysaccharides enhance the humoral and cellular immune responses of hepatitis B surface antigen vaccination through inhibiting the expression of transforming growth factor β and the frequency of regulatory T cells.” FEMS Immunol Med Microbiol. 2011 Nov;63(2):228-35 http://www.ncbi.nlm.nih.gov/pubmed/22077226
CHAMOMILE
Chamomile (Matricaria chamomila [German chamomile]; Anthemis nobilis [Roman chamomile]) is a member of the daisy family. It is currently one of the most popular herbs in the United States and is widely used as an herb tea, in shampoos and soaps, and in skin-care products. Chamomile has been known as a sedative and antifever medicine since ancient times and was used by Greek and Roman physicians to treat a variety of ailments.
Contemporary herbalists recommend chamomile to treat digestive problems and ulcers, to prevent the spread of infections, and to reduce inflammation. Because chamomile is an antispasmodic, it has also been used to lessen the severity of menstrual cramps. Perhaps the most interesting effect of this herb is its ability to stimulate the immune system. British researchers discovered that chamomile increases macrophages and B lymphocytes.
USES IN CFS/ME. Patients with CFS/ME have chamomile tea before bedtime to help with insomnia and to alleviate gastrointestinal symptoms. Simply inhaling the steam is enough to produce a calming effect. (The sedative effects of the tea may be due to apigenin, a flavonoid that binds to benzodiazepine receptors.) In general, the herb is well tolerated. Chamomile tea should not be boiled because boiling makes the tea bitter. Those allergic to ragweed should avoid this herb.
FURTHER READING
General information about chamomile: http://www.herbwisdom.com/herb-chamomile.html
ECHINACEA
The roots of the purple coneflower (Echinacea angustifolia, E. purpura) were used by Plains Indians as a cure for all kinds of infections. Although it has been relied on as a topical wound healer since Colonial times, echinacea's antibiotic properties have largely been unexplored until recently. Research conducted in Germany in the 1950s through the 1980s revealed that echinacea has broad antibiotic properties, much like penicillin, due to a substance (echinacein) that counteracts cell-penetrating enzymes. In this manner, echinacea works to strengthen individual cell defenses.
Echinacea also acts as an immune system stimulant. Echinacea boosts the macrophage's ability to destroy germs. It possesses antifungal as well as antibacterial properties. As an antiviral agent, echinacea has been used effectively to treat influenza and the common cold as well as to check herpesvirus infections.
488
USES IN CFS/ME. People with CFS/ME often use echinacea at the first sign of a cold or flu to help lessen the severity of the illness, and some even report lessening of all symptoms after using this herb. Echinacea tinctures are more effective than pills or capsules. An alcohol-free tincture should be used, however, because alcohol dramatically lessens the potency of this herb. Dry echinacea root can be purchased in health food stores and boiled to make a tea.
PROTOCOL. Dr. Teitelbaum recommends 300 to 325 mg taken three times a day. He recommends that patients take a break from echinacea for one week each month, or it will stop working. He suggests echinacea may also improve adrenal function. Other practitioners recommend starting at lower doses (200 mg). Alcohol-free tinctures can be taken at 15 to 20 drops a day.
Dr. Cheney is not a fan of echinacea. He believes that the immune-activating properties of the herb may pose problems for CFS/ME patients with upregulated immune systems.
FURTHER READING
General information about echinacea: http://www.herbwisdom.com/herb-echinacea.html
CFS/ME patient reviews of echinacea: http://www.revolutionhealth.com/drugs-treatments/rating/echinacea-echinacea-spp-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
See DM, Broumand N, Sahl L, Tilles JG. “In vitro effects of echinacea and ginseng on natural killer and antibody-dependent cell cytotoxicity in healthy subjects and chronic fatigue syndrome or acquired immunodeficiency syndrome patients.” Immunopharmacology 1997 Jan;35(3):229-35. http://www.ncbi.nlm.nih.gov/pubmed/9043936 (Abstract)
GARLIC
Garlic (Allium sativum) has a long history as a medicinal plant. The earliest medicinal description of garlic dates from 3000 BC. Garlic was even found in the tomb of King Tut. It has been used to treat headache, insect bites, menstrual disorders, intestinal worms, tumors, and heart disease. Garlic is a powerful antibiotic and antiprotozoan agent. It kills intestinal parasites, destroys the bacterium that causes tuberculosis, and can be used against various fungi, including Candida albicans. Daily ingestion of as little as half a clove of garlic can lower cholesterol. Garlic also lowers blood pressure, which means it may have a negative effect on people with hypotension. Some people with CFS/ME tend to be sensitive to garlic in both its raw and cooked forms. Enteric, deodorized garlic pills can reduce intestinal upset. A commonly recommended brand of deodorized garlic in capsules, Kyolic, is widely available from health food stores.
FURTHER READING
489
General information about garlic: http://www.herbwisdom.com/herb-garlic.html
CFS/ME patient reviews of garlic: http://www.revolutionhealth.com/drugs-treatments/rating/garlic-allium-sativum-for-chronic-fatigue-syndrome-cfs-cfids-me
GINGER
Ginger (Zingiber officinale) was used by the ancient Greeks as a digestive aid. It is still used as an antidote for motion sickness, nausea, and numerous digestive disturbances. It soothes smooth muscles, making it useful for alleviating menstrual cramps, as well. Ginger can be taken in capsule form or boiled to make tea. Ginger root is available from grocery or health food stores. Ginger powder, however, as found in the spice section of a grocery store, should not be used as a medication because it is usually irradiated. Excessive amounts may cause mild headache. Some people with CFS/ME find ginger difficult to tolerate.
USES IN CFS/ME. Dr. Teitelbaum is a ginger enthusiast. He recommends it for relief of muscle and joint pain, nausea, migraines, motion sickness, and for raising blood pressure (for those with hypotension). The most common use among people with CFS/ME is for nausea, a symptom which can be utterly debilitating if unchecked.
PROTOCOL. Ginger is a food, so it can be taken on an as-needed basis. It can be purchased as a whole root, grated and added to food, or boiled to make a tea. For those with less tolerance for ginger's strong flavor, candied ginger may be eaten (or simply held under the tongue) as an alternative. Dry encapsulations are also available, although these tend to be less effective.
PROS AND CONS. A small amount of ginger goes a long way. CFS/ME patients find it especially effective for nausea and dizziness. It has an almost immediate effect. Dry ginger capsules may cause heartburn.
AVAILABILITY AND COST. Fresh ginger and candied ginger are available in health food stores, supermarkets and Asian specialty markets. Dried, encapsulated ginger can be purchased at health food stores and from online distributors. A 180-capsule bottle of Nature's Way dry ginger costs about $5 from Vitacost.
FURTHER READING
CFS/ME patient reviews of ginger: http://www.revolutionhealth.com/drugs-treatments/rating/ginger-zingiber-officinale-for-chronic-fatigue-syndrome-cfs-cfids-me
GINGKO
Gingko (Gingko biloba) is the oldest species of tree on the planet. The Chinese have used its leaves for over 5000 years as an elixir to promote longevity. Studies have shown that gingko, by increasing blood flow to the brain, helps reduce the risk of stroke. It can also dramatically improve memory and reaction time. The neuroprotective effects of gingko are well documented. There is some evidence that
490
gingko modulates serotonin and dopamine, and may have antidepressant-like effects. Gingko also acts as a potent antioxidant, reducing oxidative stress by simultaneously scavenging peroxynitrite, nitric oxide and superoxide. In Europe, gingko is used as a conventional drug for treating short-term memory loss, headache, tinnitus, anxiety, vertigo, and depression.
USES IN CFS/ME. Alan Logan and Cathy Wong, in their comprehensive assessment of non-drug treatments for CFS/ME, state that because ginkgo has specific effects on cerebral blood flow, it may be useful for CFS symptoms related to hypoperfusion in the brain. Many CFS/ME doctors have recommended gingko to their patients, including Dr. Cheney and Dr. Teitelbaum.
PROTOCOL. For maximum effectiveness, gingko biloba should be taken as an extract (not a tea). Extracts are available in either pill or liquid form. In pill form, Dr. Teitelbaum recommends a 50:1 extract standardized to have 24% Glycosides (this will be indicated on the label). A 60-mg capsule can be taken once a day. The standard dose of liquid extract is 20 drops, up to three times a day. It may take up to six weeks to take effect.
PROS. For some people, gingko has been a “lifesaver,” allowing them to process information again. Many CFS/ME patients have reported that gingko helps cognitive function, memory, and “brain fog.” Some report a decrease in migraines and headache, as well as increased circulation to the legs.
CONS. Although gingko is usually well tolerated, some patients with CFS/ME have reported increased fatigue. Excessive doses can cause irritability, restlessness, nausea, and diarrhea. Gingko has mild blood thinning properties, which means it cannot be taken in conjunction with pharmaceutical blood thinners (e.g., Coumadin).
FURTHER READING
General information about gingko: http://www.herbwisdom.com/herb-ginkgo-biloba.html
More general information about gingko: http://www.altnature.com/gallery/Ginkgo_Biloba.htm
CFS/ME patient reviews of gingko: http://www.revolutionhealth.com/drugs-treatments/rating/ginkgo-ginkgo-biloba-for-chronic-fatigue-syndrome-cfs-cfids-me
Logan, Alan C., and Cathy Wong. “Chronic Fatigue Syndrome: Oxidative Stress and Dietary Modifications.” http://www.thorne.com/altmedrev/.fulltext/6/5/450.pdf
RESEARCH
Bastianetto S, Ramassamy C, Doré S, Christen Y, Poirier J, Quirion R. “The Ginkgo biloba extract (EGb 761) protects hippocampal neurons against cell death induced by beta-amyloid.” Eur J Neurosci. 2000 Jun;12(6):1882-90. http://www.ncbi.nlm.nih.gov/pubmed/10886329 (Abstract)
Diamond BJ, Shiflett SC, Feiwel N, Matheis RJ, Noskin O, Richards JA, Schoenberger NE. “Ginkgo biloba extract: mechanisms and clinical indications.”
491
Arch Phys Med Rehabil. 2000 May;81(5):668-78. http://www.ncbi.nlm.nih.gov/pubmed/10807109 (Abstract)
Ihl R., Bachinskaya N., Tribanek M., Hoerr R. and Napryeyenko O. for the GOTADAY Study Group. “Efficacy and Tolerability of a Once Daily Formulation of Ginkgo biloba Extract EGb 761® in Alzheimer's disease and Vascular Dementia: Results from a Randomised Controlled Trial.” Pharmacopsychiatry. 2011 Nov 15. http://www.ncbi.nlm.nih.gov/pubmed/22086747 (Abstract)
Rojas P, Serrano-García N, Medina-Campos ON, Pedraza-Chaverri J, Ogren SO, Rojas C. “Antidepressant-like effect of a Ginkgo biloba extract (EGb761) in the mouse forced swimming test: role of oxidative stress.” Neurochem Int. 2011 Oct;59(5):628-36. http://www.ncbi.nlm.nih.gov/pubmed/21672588 (Abstract)
Woelk H, Arnoldt KH, Kieser M, Hoerr R. “Ginkgo biloba special extract EGb 761 in generalized anxiety disorder and adjustment disorder with anxious mood: a randomized, double-blind, placebo-controlled trial.” J Psychiatr Res. 2007 Sep;41(6):472-80. http://www.ncbi.nlm.nih.gov/pubmed/16808927 (Abstract)
GINSENG
Ginseng (Panax schinseng,aka Chinese or Korean ginseng) is an ancient tonic and stimulant. It has been shown to possess anti-inflammatory, anti-diabetic, and antioxidant properties. Ginseng is frequently described as an “adaptogen,” which means it can have normalizing metabolic effects, especially when homeostasis is disrupted. Although it possesses enormous therapeutic potential for common ailments, ginseng is usually not recommended to patients with severe CFS/ME. Ginseng stimulates the adrenal glands and can increase production of interferon. Because most patients with CFS/ME have excessive interferon production as well as endocrine abnormalities, panax ginseng may increase symptoms.
Siberian ginseng (Eleutherococcus senticoccus), although it belongs to a different genus, has similar medicinal qualities to panax ginseng. (Though interestingly, Siberian ginseng appears to have the opposite effect of reducing inflammatory responses.) Siberian ginseng, marketed as Eleutherococcus Senticosus, is less expensive than panax ginseng and is often found in herbal ginseng formulations. (Check the label if you are looking for pure panax ginseng.)
Ginseng should not be used with estrogens or corticosteroids because of possible additive effects. It may affect the blood glucose levels of patients with diabetes mellitus.
RESEARCH
Gaffney BT, Hügel HM, Rich PA. “Panax ginseng and Eleutherococcus senticosus may exaggerate an already existing biphasic response to stress via inhibition of enzymes which limit the binding of stress hormones to their receptors.” Med Hypotheses. 2001 May;56(5):567-72. http://www.ncbi.nlm.nih.gov/pubmed/11388770 (Abstract)
Jung CH, Jung H, Shin YC, Park JH, Jun CY, Kim HM, Yim HS, Shin MG, Bae HS, Kim SH, Ko SG. “Eleutherococcus senticosus extract attenuates LPS-induced
492
iNOS expression through the inhibition of Akt and JNK pathways in murine macrophage.” J Ethnopharmacol. 2007 Aug 15;113(1):183-7. http://www.ncbi.nlm.nih.gov/pubmed/17644291 (Abstract)
See DM, Broumand N, Sahl L, Tilles JG. “In vitro effects of echinacea and ginseng on natural killer and antibody-dependent cell cytotoxicity in healthy subjects and chronic fatigue syndrome or acquired immunodeficiency syndrome patients.” Immunopharmacology. 1997 Jan;35(3):229-35. http://www.ncbi.nlm.nih.gov/pubmed/9043936 (Abstract)
GOLDENSEAL
Goldenseal (Hydrastis canadensis) is a North American herb known best for its antibiotic properties. Berberine, a substance found in goldenseal, kills many of the bacteria that cause diarrhea, as well as the protozoa that cause amoebic dysentery and giardiasis. It has been used against cholera bacteria and as a treatment for throat, sinus, and topical bacterial infections. Research has shown that goldenseal is also effective against some viral infections. People with CFS/ME generally use goldenseal to treat sinusitis and canker sores. It should be used with caution, however. Excessive or lengthy (more than 10 days) treatment can lead to neurological disturbances and gastrointestinal upset. The safest way to take goldenseal is externally as a poultice or paste spread directly over the sinuses or other affected area. Goldenseal should not be used during pregnancy because it stimulates uterine contractions.
RESEARCH
Cecil CE, Davis JM, Cech NB, Laster SM. “Inhibition of H1N1 influenza A virus growth and induction of inflammatory mediators by the isoquinoline alkaloid berberine and extracts of goldenseal (Hydrastis canadensis).” Int Immunopharmacol. 2011 Nov;11(11):1706-14. http://www.ncbi.nlm.nih.gov/pubmed/21683808 (Abstract)
GOTU KOLA
Gotu kola (Centella asiatica; Hydrocotyle asiatica), also known as sheep rot, Indian pennywort, marsh penny, and water pennywort, was originally used in Sri Lanka as a promoter of longevity. It is a member of the Umbelliferae family, which also includes carrots, parsley, dill, and fennel. Despite the similarity in name, gotu kola is not related to the stimulant kola. In small amounts, gotu kola is taken as a tonic, and in larger amounts as a sedative. Gotu kola traditionally has been used in the treatment of leprosy, but it is also noted for its ability to promote blood circulation. Gotu kola has been used to increase memory and mental function by increasing circulation to the brain.
FURTHER READING
Shinomol G K, Muralidhara, Bharath M M. “Exploring the Role of "Brahmi" (Bocopa monnieri and Centella asiatica) in Brain Function and Therapy.”
493
Recent Pat Endocr Metab Immune Drug Discov 2011 Jan;5 1:33-49. http://www.ncbi.nlm.nih.gov/pubmed/22074576 (Abstract)
KAVA
Kava, or kava-kava (Piper methysticum) is a plant native to the Pacific. Traditionally, it has been used in the South Pacific in drinks. The roots of the plants have a sedative effect, making it a popular treatment for anxiety.
There has been a considerable amount of controversy surrounding the medicinal use of kava in recent years. In 2001, researchers discovered an apparent link to kava and liver toxicity which led European, British and Canadian authorities to ban kava sales in 2002. However, further research indicated that the toxic compounds were located in the stem peelings and leaves, which are parts of the plant not traditionally consumed. (Only the roots are used in Pacific cultures.) A study published in 2003 by Whitton et al found that modern extraction methods, using acetone or ethanol, were responsible for kava toxicity.
Kava is used primarily as a sleep aid and as an anxiolytic. In 1997 Volz et al found that an extract of kava was just as efficacious as benzodiazepines or antidepressants in reducing anxiety, and with none of the side effects. There is also some evidence that kava may be useful in treating ADD, which might help reduce the need for stimulant medications in children.
PROTOCOL. The recommended dose of kava extract for insomnia is 70 – 200 mg taken an hour before bedtime. For daytime anxiety, 70 mg may be taken one to three times a day. Kava is not sedating when taken at moderate doses. To avoid stomach upset, it's best to take kava with a little food.
RESEARCH
Sarris J, Kean J, Schweitzer I, Lake J. “Complementary medicines (herbal and nutritional products) in the treatment of Attention Deficit Hyperactivity Disorder (ADHD): a systematic review of the evidence.” Complement Ther Med. 2011 Aug;19(4):216-27. http://www.ncbi.nlm.nih.gov/pubmed/21827936 (Abstract)
Teschke R, Sarris J, Schweitzer I. “Kava hepatotoxicity in traditional and modern use: The presumed Pacific kava paradox hypothesis revisited.” Br J Clin Pharmacol. 2011 Jul 29. http://www.ncbi.nlm.nih.gov/pubmed/21801196 (Abstract)
Volz HP, Kieser M. “Kava-kava extract WS 1490 versus placebo in anxiety disorders--a randomized placebo-controlled 25-week outpatient trial.” Pharmacopsychiatry 1997 Jan;30(1):1-5. http://www.ncbi.nlm.nih.gov/pubmed/9065962 (Abstract)
Whitton, Peter A., Andrew Lau, Alicia Salisbur, Julie Whitehousec, Christine S. Evans. “Kava lactones and the kava-kava controversy.” Phytochemistry, Volume 64, Issue 3, October 2003, Pages 673-679. http://www.sciencedirect.com/science/article/pii/S0031942203003819
494
LICORICE
Licorice (Glycyrrhiza glabra) has long been known as one of nature's most potent healing herbs. It is a popular ingredient in many Chinese herbal remedies and has been used to treat cough, sore throat, ulcers, arthritis, herpes infections, and hepatitis. When combined with other herbs, licorice can increase their effectiveness.
USES IN CFS/ME. In CFS/ME, licorice is reputed to alleviate symptoms associated with adrenal insufficiency (intolerance to heat, cold, noise, and other stimuli, low blood pressure, faintness). Because the action of licorice's main active chemical, glycyrretinic acid (GA), resembles that of the adrenal hormone aldosterone, licorice helps the body retain salt (and water) and ultimately may help raise blood volume and pressure. Because low blood pressure is a problem for many patients with CFS/ME, licorice could prove beneficial, especially for those who are sensitive to the drugs normally recommended to correct low blood pressure. In addition, licorice raises serum cortisol levels (often low in CFS/ME patients) and stimulates natural killer cell activity.
PROTOCOL. Dr. Riccardo Baschetti has used licorice for patients with low or low-normal plasma levels of cortisol. He claimed that dramatic improvement in CFS/ME symptoms could be seen after taking licorice for just three days (New Zealand Medical Journal, 1995). Baschetti recommends 2.5 gm of licorice root a day, in extract or capsules dissolved in milk. (Milk enhances the aldosterone-like effects of the licorice.)
Dr. Peter D'Adamo, a naturopath who also uses licorice to treat symptoms of CFS/ME, suggests taking ¼ teaspoon (2 gm) of solid licorice extract one to three times a day. He recommends his patients take 500 mg of the amino acid methionine and 99 mg of potassium supplement three times a day along with the licorice to counteract any potassium and sodium imbalances.
A number of physicians have recommended licorice for NMH (neurally mediated hypotension). NMH is a common problem for patients with CFS/ME, affecting up to 90% of the CFS/ME population. Many people with CFS/ME are sensitive to Florinef, the medication normally prescribed for NMH. Dr. Calkins, a member of the team at Johns Hopkins Medical Center that performed the initial investigations on NMH in adolescents, stated that "medicinal licorice is a good alternative for those sensitive to Florinef."
Dr. Cheney also endorses licorice for treating NMH. Dr. Cheney has found that Florinef forces potassium depletion, which further depresses the HPA (hypothalamus-pituitary-adrenal) axis in CFS/ME patients. Licorice can accomplish the same results as Florinef, without the side effects. He recommends two licorice root tablets with glycerizzin two times a day. Dr. Cheney adds the caution, “Blood pressure must be monitored when taking licorice root!”
For optimal effect, licorice should be taken in the morning. (Cortisol levels in the body reach their peak at about 8AM.) It is important to note that licorice candies produced in the U.S. do not use licorice, but anise, as a flavoring. Doctors caution their patients to use pure licorice, not DGL. DGL (de-glycyrrhizinated
495
licorice ), a form of licorice in which glycyrrhizin has been removed. Glycyrrhizin is removed in DGL to prevent hypertension, however, it is the ingredient in licorice that treats NMH.
PROS AND CONS. Patients who have taken licorice report increased energy levels and improvement in symptoms of hypoglycemia, though some have noticed that its effectiveness wanes after a few months. Because of its steroid-like qualities, and due to its ability to help retain sodium, it is important to monitor licorice intake. Too much licorice, especially without potassium supplementation, can cause serious side effects. If high blood pressure, headaches, lethargy, and water retention develop, the dosage should be decreased immediately. Patients taking drugs that could interact with licorice, such as heart medications, MAOIs, or diuretics, should consult with their physician before embarking on a licorice protocol.
AVAILABILITY AND COST. Solid licorice extract is marketed by Allergy Research Group. A 4-oz container (½ tsp = 3 grams) sells for $24 through PureFormulas.com (online). Douglas Labs sells a 60-capsule bottle of pure licorice (500 mg) for $16 (also through PureFormulas.com).
FURTHER READING
Good article on licorice: http://drholly.typepad.com/licorice/
Excellent summary of licorice as a treatment for CFS/ME: http://www.encognitive.com/node/15023
General information on licorice root: http://www.herbwisdom.com/herb-licorice-root.html
Ray Sahelian on licorice: http://www.raysahelian.com/licorice.html
Baschetti, R. “Chronic fatigue syndrome and liquorice” N Z Med J. 1995 Apr 26;108(998):156-7.
LOMATIUM
Lomatium is a North American herb reputed to have antiviral properties. It has been used to treat influenza, colds, and diseases such as measles. A number of patients who have tried lomatia extract have felt overstimulated. Some have experienced malaise, insomnia, and jitteriness after as little as one drop. Reports from the late 1980s stated that some CFS/ME patients have developed severe allergic reactions while taking this herb.
FURTHER READING
Literally everything you need to know about lomatium: http://www.naturalpedia.com/Lomatium.html
MILK THISTLE/SILYMARIN
Milk thistle (Silybum marianum), also referred to as silymarin, appears to have a remarkable effect on the liver. There is a great deal of research showing that active ingredient in silymarin, silybin, stimulates liver cells to regenerate and is effective in treating jaundice, hepatitis C, and cirrhosis. Silymarin increases the
496
amount of liver glutathione, a tripeptide that activates liver enzymes. As a consequence, milk thistle helps protect the liver from toxins, including poisonous mushrooms, and various petrochemicals. In addition, silymarin has powerful antioxidant, anti-inflammatory, anti-cancer and cardioprotective properties. It also helps synthesize superoxide dismutase (SOD), an enzyme that increases mitochondrial function and can prevent oxidative stress both within and outside cell walls.
USES IN CFS/ME. Dr. Cheney has proposed that many people with CFS/ME have reduced liver function, and even subclinical hepatitis. For CFS/ME patients with mild liver dysfunction, milk thistle may provide some relief.
PROTOCOL. Milk thistle is poorly absorbed, so 150-300 mg a day is needed for basic liver support. Dr. Cheney recommends 150 mg silymarin/milk thistle taken twice a day. Siliphos, a more bioavailable form of silymarin, may be taken at lower doses. Some studies show that a silymarin-phosphatidylcholine complex may be absorbed more easily than regular standardized milk thistle. Phosphatidylcholine, a key element in cell membranes, helps silymarin attach easily to cell membranes, which may help in keeping toxins from getting inside liver cells.
PROS AND CONS. While milk thistle is generally well tolerated, common side effects are itching, indigestion and headache. Some patients have reported nausea and poor appetite on higher doses. People with allergies to plants in the aster family: daisies, artichokes, ragweed, chrysanthemums, marigolds, chamomile, yarrow, kiwi, and common thistle may also be allergic to milk thistle.
AVAILABILITY AND COST. Milk thistle, in liquid or capsule form, can be purchased at any health food store and through online vitamin suppliers. Standardized milk thistle extracts yielding 80% of the active ingredient in silymarin, silybin, are recommended. Jarrow, Metabolic Maintenance, Pure Encapsulations, and Douglas Labs all market standardized milk thistle. Prices range from $13 to $30 for a 100-capsule bottle. Siliphos is available from Vitacost and PureFormulas.com for roughly the same price.
FURTHER READING
Detailed information on silymarin: http://www.salamresearch.com/html/milk_thistle_product.html
Ray Sahelian on milk thistle. Includes dosage, research and medical uses. http://www.raysahelian.com/silymarin.html
RESEARCH
Chen IS, Chen YC, Chou CH, Chuang RF, Sheen LY, Chiu CH. “Hepatoprotection of silymarin against thioacetamide-induced chronic liver fibrosis.” J Sci Food Agric. 2011 Nov 18. http://www.ncbi.nlm.nih.gov/pubmed/22102319 (Abstract)
Kalantari H, Shahshahan Z, Hejazi SM, Ghafghazi T, Sebghatolahi V. “Effects of silybum marianum on patients with chronic hepatitis C.” J Res Med Sci. 2011 Mar;16(3):287-90. http://www.ncbi.nlm.nih.gov/pubmed/22091246 (Abstract)
497
Rašković, A.; Stilinović, N.; Kolarović, J.; Vasović, V.; Vukmirović, S.; Mikov, M. “The protective effects of silymarin against doxorubicin-induced cardiotoxicity and hepatotoxicity in rats.” Molecules. 2011 Oct 12;16(10):8601-13. http://www.mdpi.com/1420-3049/16/10/8601
ST. JOHN'S WORT
St. John's Wort (Hypericum perforatum), a plant with anti-inflammatory, antiseptic and mood lifting properties, has been documented as a remedy for roughly two thousand years. Currently, it is a well-established treatment for depression. In Germany, St. John's Wort is widely prescribed for children and teens with depression as a safe alternative to antidepressants. The Cochrane Collaboration, an organization that reviews trials of health care treatments, found that in 29 studies with over 5,400 depressed patients St. John's Wort fared better than placebo.
Like most herbs, St. John's Wort has the potential to treat a variety of health problems. In 2011 Mozaffari et al found that St. John's Wort was useful for treating IBS (irritable bowel syndrome), a bowel motility condition for which antidepressants are sometimes prescribed. Studies have shown that St. John's Wort increases mitochondrial function, reduces inflammation, and inhibits nerve firing in epilepsy.
PROS AND CONS. St. John's Wort is generally well tolerated. However, it cannot be taken in conjunction with other antidepressants. Like any pharmaceutical antidepressant, it cannot be taken within two weeks of treatment with MAOIs. St. John's Wort decreases the effectiveness of many drugs, including benzodiazepines, oral contraceptives, beta blockers, statins, antiretrovirals, and theophylline.
FURTHER READING
Good general information about St. John's Wort: http://www.herbwisdom.com/herb-st-johns-wort.html
Cochrane Collaboration's summary of research on St. John's Wort for depression. http://summaries.cochrane.org/CD000448/st.-johns-wort-for-treating-depression.
A CFS/ME patient's review of St. John's Wort: http://www.revolutionhealth.com/drugs-treatments/rating/st-johns-wort-hypericum-perforatum-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Huang N, Rizshsky L, Hauck C, Nikolau BJ, Murphy PA, Birt DF. “Identification of anti-inflammatory constituents in Hypericum perforatum and Hypericum gentianoides extracts using RAW 264.7 mouse macrophages.” Phytochemistry. 2011 Nov;72(16):2015-23. http://www.ncbi.nlm.nih.gov/pubmed/21855951 (Abstract)
Mozaffari S, Esmaily H, Rahimi R, Baeeri M, Sanei Y, Asadi-Shahmirzadi A, Salehi-Surmaghi MH, Abdollahi M. “Effects of Hypericum perforatum extract
498
on rat irritable bowel syndrome.” Pharmacogn Mag. 2011 Jul;7(27):213-23. http://www.ncbi.nlm.nih.gov/pubmed/21969792 (Abstract)
Wang Y, Zhang Y, He J, Zhang H, Xiao L, Nazarali A, Zhang Z, Zhang D, Tan Q, Kong J, Li XM. “Hyperforin promotes mitochondrial function and development of oligodendrocytes.” J Neurochem. 2011 Nov;119(3):555-68. http://www.ncbi.nlm.nih.gov/pubmed/21848657 (Abstract)
Woelk H. “Comparison of St John's wort and imipramine for treating depression: randomised controlled trial.” BMJ. 2000 Sep 2;321(7260):536-9. http://www.ncbi.nlm.nih.gov/pubmed/10968813 (Abstract)
UVA URSI
A member of the Ericaceae family, uva ursi (Arctostaphylos uva-ursi) has been used for more than 100 years as a urinary tract antiseptic. Once in the urinary tract, the chemical (arbutin) found in uva ursi is transformed into an antiseptic agent, hydroquinone. This herb also contains diuretic chemicals (ursolic acid) and astringents. However, uva ursi is effective against urinary tract infections only if the urine is alkaline; therefore, citrus fruits (including tomatoes), vitamin C, and acidic foods should be avoided immediately before and after taking it.
Uva ursi is also used as an anti-Candida treatment and as an anti-bacterial.
PROS AND CONS. Some patients have reported “die-off” reactions from taking uva ursi.
VALERIAN
Valerian (Valeriana officionalis) has long been used as a tranquilizer, and for treating epilepsy, nervousness, anxiety, insomnia, headache, and intestinal cramps. During World War I, it was routinely taken to relieve the "overwrought nerves" brought on by artillery bombardment. Valerian is used extensively in Germany, where it is the active ingredient in more than 100 over-the-counter sleep aids. The active ingredients in valerian are chemicals known as valepotriates, which are found in highest concentrations in the roots of the plant.
CFS/ME physicians recommend valerian primarily as a sleep aid. It can be taken as a tea or in capsule form, but because of its odor, capsules are usually preferred. Valerian should be taken with a little milk or food to prevent stomach upset. Valerian is often combined with other herbal sleep aids, such as passionflower, hops, and skullcap.
FURTHER READING
Good summary of the uses of valerian: http://www.herbwisdom.com/herb-valerian.html
Several CFS/ME doctors discuss remedies for insomnia, including valerian. http://www.prohealth.com/library/showarticle.cfm?libid=8563
RESEARCH
499
Dimpfel W, Suter A. “Sleep improving effects of a single dose administration of a valerian/hops fluid extract - a double blind, randomized, placebo-controlled sleep-EEG study in a parallel design using electrohypnograms.” Eur J Med Res. 2008 May 26;13(5):200-4. http://www.ncbi.nlm.nih.gov/pubmed/18559301 (Abstract)
Leathwood PD, Chauffard F, Heck E, Munoz-Box R. “Aqueous extract of valerian root (Valeriana officinalis L.) improves sleep quality in man.” Pharmacol Biochem Behav. 1982 Jul;17(1):65-71. http://www.ncbi.nlm.nih.gov/pubmed/7122669 (Abstract)
Taavoni S, Ekbatani N, Kashaniyan M, Haghani H. “Effect of valerian on sleep quality in postmenopausal women: a randomized placebo-controlled clinical trial.” Menopause. 2011 Sep;18(9):951-5. http://www.ncbi.nlm.nih.gov/pubmed/21775910 (Abstract)
HISTAME
DESCRIPTION. Histame is a dietary supplement containing the enzyme, diamine oxidase (DAO).
BACKGROUND. Diamine oxidase (also known as histaminase) is an enzyme found in large concentrations in the intestinal lining (mucosa) of all mammals. Its function is to break down histamine. Unlike antihistamines, Histame does not block histamine receptors, but acts directly on histamine itself.
In a study published in 1980, Luk et al found that after inducing damage to the intestines of rats, the amount of diamine oxidase was an accurate marker of intestinal integrity. The lower the amount of diamine oxidase, the greater the degree of damage. The researchers concluded that diamine oxidase was unique among intestinal mucosal enzymes in its ability to predict intestinal integrity.
In 2007 Maintz and Novak observed that people with low amounts of DAO can develop food sensitivities which symptomatically mimic food allergies (flushing, hypotension, diarrhea, headache, tachycardia, and itching). Although their symptoms match those of true allergies, these individuals do not test positive for IgE-mediated allergies. Low levels of circulating DAO prevent the breakdown of histamine in their intestines, causing allergic-type reactions, particularly to histamine-rich foods. Foods that are rich in histamine include all fermented and aged foods: cheese, alcohol, sauerkraut, canned fish (tuna, sardines), pizza, processed meats, as well as many fruits and chocolate. Nearly 100 drugs have been found to cause a decrease in DAO activity, including doxycycline, MAO inhibitors, cimetidine (Tagamet), and Verapamil (a calcium-channel blocker). DAO requires copper and Vitamins B2 and B6.
USES IN CFS/ME. Histamine intolerance is characteristic of CFS/ME patients. Aside from new allergies, many CFS/ME patients develop food sensitivities, as well as conditions such as migraines, rosacea and interstitial cystitis, which are provoked by tyrosine-rich foods. (Tyrosine is converted to tyramine, which is closely related to histamine.) Histame has been recommended by Dr. Kenny De Meirleir as part of treating gut dysbiosis in CFS/ME patients.
500
PROTOCOL. The makers of Histame recommend taking one or two tablets within 15 minutes of consuming histamine-rich food. The capsules can be opened and the contents swallowed, if preferred.
AVAILABILITY. Histame can be purchased from a number of online sources. Prices range from $20-$40 for a bottle of 30 capsules.
FURTHER READING
Histame website: http://histame.com/
Patient thread on Histame: http://forums.phoenixrising.me/showthread.php?11967-90-cured-from-bed-bound-with-Histrelief-Histame-Daosin
Patient thread on histamine intolerance: http://forums.phoenixrising.me/archive/index.php/t-1804.html
Comprehensive list of histamine-rich foods: http://histame.com/histamine-rich-foods-substances
An interesting study about histamine fish poisoning: http://www.allergyclinic.co.nz/guides/63.html
RESEARCH
Luk, G D, T M Bayless, and S B Baylin Diamine oxidase (histaminase). “A circulating marker for rat intestinal mucosal maturation and integrity.” J Clin Invest. 1980 July; 66(1): 66–70. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC371506/
Maintz, Laura and Natalija Novak. “Histamine and histamine intolerance.” American Journal of Clinical Nutrition, Vol. 85, No. 5, 1185-1196, May 2007 http://www.ajcn.org/content/85/5/1185.full
In-depth medical study examining the effects of histamine on the gut, histamine intolerance, and the correlation of DAO levels with food intolerance.
INOSINE/ISOPRINOSINE
DESCRIPTION. Inosine is a purine ribonucleoside (a nitrogen-containing compound combined with D-ribose). Isoprinosine (brand: Imunovir) is its pharmaceutical equivalent (now largely replaced by inosine).
BACKGROUND. Inosine is a naturally occurring chemical in the body which leads to the production of uric acid, a potent free radical scavenger. As a basic component of cells, uric acid is involved in a number of physiological processes including carbohydrate metabolism, insulin regulation, and protein synthesis. Uric acid levels are low in all inflammatory diseases, including CFS/ME. Pharmaceutical forms of inosine (inosine pranobex, or isoprinosine) have been used as immune system modulators. Currently, inosine is being investigated as a possible treatment for Parkinson's disease.
As a supplement, inosine is primarily used to enhance athletic performance. Manufacturers claim that because inosine is a precursor to adenosine, it facilitates the production of ATP (adenosine triphosphate). As a consequence, inosine should theoretically increase energy and endurance. Although there does not appear to be
501
any research to substantiate these claims, inosine is included in many sports supplements.
USES IN CFS/ME. Both Dr. Kenny De Meirleir and Dr. Cheney have largely replaced isoprinosine with inosine in their treatment protocols, under the assumption that the two are equivalent. Inosine, like its pharmaceutical counterpart, is supposed to modulate the immune system and act as an antiviral. However, inosine does not appear to possess the same antiviral properties as isoprinosine. The main function of inosine is as an antioxidant, which is linked to its ability to raise uric acid levels in the blood.
Dr. Klimas still uses isoprinosine (Imunovir) with her patients. The protocol is to alternate taking 3 and 6 pills daily, with weekends off, for three months. Over the next three months no Imunovir is taken. The physician decides how often to repeat this course of medication based on immune markers (as determined by blood tests).
PROTOCOL. The standard dosage of inosine is 500 mg three times a day for five days a week (allowing for weekend “drug holidays”). As always, CFS/ME patients are advised to start with low doses.
PROS AND CONS. Paradoxically, inosine seems to help with joint pain (gout is caused by an excess of uric acid, which is raised by inosine) and, to some degree, with energy. Although inosine functions as an antioxidant, the process of converting it to uric acid produces superoxide, a potent oxidant. Some patients report that inosine works fine for a while and then stops having an effect. Patients who were previously able to tolerate isoprinosine have reported headaches and insomnia while taking inosine.
AVAILABILITY AND COST. Inosine is a supplement, which means it can be purchased without a prescription at health food stores and from online distributors. Source Naturals markets a 120-tablet bottle of inosine (500 mg) for roughly $20. Imunovir is currently registered outside the United States for the treatment of acute and chronic viral infections, including herpes and measles. It can be obtained in Canada.
FURTHER READING
Basic information on isoprinosine, including sources. http://www.anapsid.org/cnd/drugs/isoprinosine.html
Manufacturer's description of Imunovir: http://www.rivexpharma.com/products_imunovir.html
CFS/ME patient thread discussing isoprinosine and inosine: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=1396515
INOSITOL
DESCRIPTION. Inositol is a carbocyclic polyol (a sugar alcohol) which forms an essential component of cell membranes.
BACKGROUND. Inositol, like choline, is an important component of phospholipids, the fatty substances which surround all cells in the body. Also like
502
choline, inositol helps with the transportation of fats, and prevents their accumulation in any one site (e.g., the liver). Because it is a key component of the myelin sheaths that surround nerves in the central nervous system, inositol performs a crucial role in maintaining the integrity of the nervous system.
Inositol also plays an important role in energy metabolism; its metabolites regulate bone mass and mediate amino acid signaling, acting as a “second messenger” for cell receptors. Inositol phosphates are important for a number of cellular functions, including cell growth, apoptosis (programmed cell death), cell migration, and cell differentiation. Inositol is found in the brain and nerves, muscles, bones, reproductive organs, stomach, kidney, spleen, liver and heart.
Because inositol is a second messenger of serotonin, it has been successfully used to treat several psychiatric conditions. (Second messengers are molecules that relay signals from neurotransmitters into the cell.) Medical uses of inositol include treatment of obsessive-compulsive disorder (OCD), anxiety, and depression. Inositol is also used for insomnia.
Inositol is produced in the gut in limited quantities by bacterial flora. Dietary sources include calf liver, cantaloupe, beans, dried beans, lentils, milk, nuts, oats, pork, rice, veal, wheat germ and whole-grain products.
PROTOCOL. Dr. Myhill recommends 500-2,000 mgs for low GABA activity. Dr. Teitelbaum recommends a slightly lower dose, 500-1,000 mgs a day. Maija Haavisto reports that 500 – 750 mg taken at bedtime improves insomnia.
PROS AND CONS. Inositol is safe and inexpensive. Some people report that they wake up at night with it. (This may be due to its SSRI-like effects.)
AVAILABILITY AND COST. Pure inositol (also known as myoinositol) can be purchased in powder form. PureFormulas.com markets a 250-gram container made by Pure Encapsulations for $35 (at 500 mg a day, this will last approximately a year and five months). Inositol frequently comes combined with choline. Twinlabs, NOW, Solgar and Source Naturals all market inositol/choline combinations (500 mg) at less than $10 a bottle. Inositol often is included in B complex supplements.
FURTHER READING
Ray Sahelian's informative page on inositol: http://www.raysahelian.com/inositol.html
Links to useful articles about inositol: http://www.livestrong.com/inositol/
A nice summary of the functions of inositol in the body: http://www.diagnose-me.com/treat/T47006.html
Treatment of obsessive-compulsive disorder, panic attacks, and depression with inositol. http://www.comprehensivepsychiatricresources.com/item.php?item_id=221&category_id=48
Maija Haavisto's excellent summary of treatments she has tried. Scroll down for inositol, or read them all: http://www.fiikus.net/?cfssupplements
503
Very interesting and informative patient thread about the use of inositol in OCD and its relationship with histamine: http://www.stuckinadoorway.org/forums/archive/index.php?t-10476.html
RESEARCH
Gianfranco C, Vittorio U, Silvia B, Francesco D. “Myo-inositol in the treatment of premenstrual dysphoric disorder.” Hum Psychopharmacol. 2011 Oct;26(7):526-30. http://www.ncbi.nlm.nih.gov/pubmed/22031267 (Abstract)
MALIC ACID
DESCRIPTION. Malic acid, an intermediate in the Krebs cycle, aids in the production of adenosine triphosphate (ATP).
BACKGROUND. Malic acid is found primarily in apples and pears, as well as other fruits. It is used primarily as a flavor enhancer and to lend tartness to food products. Malic acid helps in the breakdown and utilization of fats and glucose in muscle tissue, even in low oxygen conditions, and plays an important role in the production of ATP.
USES IN CFS/ME. Because of the prominent role malic acid plays in the energy-producing Krebs cycle, a deficiency can lead to inadequate breakdown of glucose in muscle tissue, with resulting buildup of lactic acid and other toxins. Increased amounts of malic acid should relieve many of the symptoms associated with tissue acidosis (spasms, cramps, and burning pain). A number of CFS/ME physicians recommend malic acid combined with magnesium to treat fibromyalgia symptoms. Dr. Guy Abraham, Dr. J. E. Michalek, Dr. Jorge Flechas, and Dr. I. Jon Russell observed improvement in pain among CFS/ME patients taking Super Malic, a combination of 200 mg of malic acid and 50 mg of magnesium (Journal of Rheumatology, 1995). The researchers noted that low doses of Super Malic were not effective, and recommended six tablets a day for two months.
PROTOCOL. As with other supplements, physicians recommend starting with the lowest dose, one tablet daily taken with food and water, to check for possible sensitivities. The dosage can be increased gradually to between 6 and 12 tablets daily, depending on tolerance. If gastrointestinal problems develop, the dosage should be decreased. Although results may be experienced within a few days, most physicians recommend a trial of several months.
PROS. As a dietary supplement, malic acid is relatively risk free. People with CFS/ME report increased energy, less muscle pain and more stamina. One patient reported a complete cessation of leg spasms, allowing her to rest better. Surprisingly, a patient with kidney stones reported that they decreased after taking malic acid for ten days.
CONS. Some patients report nausea and stomach cramps (on 400 mg a day). Others find malic acid to be too stimulating, resulting in insomnia. The stimulating effects can be reduced by combining malic acid with magnesium.
AVAILABILITY AND COST. Malic acid is available from most health food and vitamin stores. Malic acid supplements are inexpensive. PureFormulas.com
504
sells a bottle of 90 capsules (600 mg) made by Ecological Formulas for $12. Super Malic has been discontinued. However, various combinations of magnesium and malic acid are still available. Allergy Research Group markets a 120-tablet bottle of Magnesium Malate Forte (124 mg magnesium, 500 mg malic acid, with 10 mg B2) for roughly $20 (through PureFormulas.com).
FURTHER READING
Patient thread on malic acid: http://www.chronicfatiguetreatments.com/forums/vitamins-for-chronic-fatigue-f7/topic593.html
RESEARCH
Russell IJ, Michalek JE, Flechas JD, Abraham GE. Treatment of fibromyalgia syndrome with Super Malic: a randomized, double blind, placebo controlled, crossover pilot study.” J Rheumatol. 1995 May;22(5):953-8. http://www.ncbi.nlm.nih.gov/pubmed/8587088 (Abstract)
MELATONIN
DESCRIPTION. Melatonin is a hormone produced by the pineal gland.
BACKGROUND. Melatonin is a naturally occurring hormone produced in the pineal gland, the brain's "master gland." It is derived from serotonin, one of the brain's most important neurotransmitters. Serotonin, a neurochemical derived from the amino acid tryptophan, is converted by enzymes sensitive to the diurnal cycle of darkness and light into melatonin. Melatonin, because it is produced in the part of the brain that regulates diurnal rhythms, is essential for maintaining normal sleep patterns. Large amounts of melatonin are produced in children, which is one reason why young people sleep so much. As we age, melatonin levels decrease, making it more difficult for the elderly to sleep through the night.
Disruption of both melatonin and serotonin production has been implicated in seasonal affective disorder, the treatment of which involves increasing melatonin levels through exposure to full-spectrum light early in the day. Low melatonin and serotonin levels have also been implicated as contributing factors to depression. Currently, physicians are exploring the use of melatonin as an anti-aging factor. It is possible that supplementation with melatonin in the elderly may help correct the disturbed sleep, poor immune response, and diminished capacity for tissue repair typical of the aging process.
Melatonin may also help correct insomnia in the young. Studies released by the Massachusetts Institute of Technology showed that it took less than half the time for volunteers given melatonin to fall asleep than those given a placebo. Subjects given melatonin also tended to sleep about twice as long as those given placebo and woke without the “hangover” normally associated with sleeping pills. The results of this study are encouraging to those with sleep disorders. However, the effectiveness of melatonin depends on a number of other factors.
505
Benita Middleton and her colleagues at the University of Surrey tested the effect of melatonin in conjunction with body temperature. They discovered that in subjects whose body temperature rose later in the day, melatonin had a negative effect on sleep, producing extremely fragmented sleeping and waking patterns. Although melatonin is produced in the pineal gland, it is regulated by a part of the hypothalamus, the suprachiasmatic nucleus, which acts as the body's “clock” by tracking the length of the day. The hypothalamus also controls body temperature, so it is not surprising that the body's internal clock is linked to core temperature. Middleton concluded that while melatonin plays an important role in circadian sleep cycles, the effects are highly individualized.
Melatonin also regulates the “gut clock.” About 400 times more melatonin is produced in the gut than in the brain. The reason for this vast production of melatonin is that digestion is regulated by circadian rhythms. Bile flow increases at night, as do other digestive secretions. Melatonin functions not only to set the circadian rhythms of the digestive system, but to harmonize them with immune and endocrine functions. When these rhythms are disrupted, digestive disturbances result.
It is known that people with severe insomnia are prone to irritable bowel syndrome (IBS), peptic ulcers, fatty liver, GERD, and dyspepsia. In an interesting study of the use of melatonin for treating IBS conducted by Lu et al in 2005, 88% of the patients reported significant improvement of their GI symptoms after 8 weeks of treatment with melatonin over placebo. Oddly enough, the patients experienced no difference in sleep between melatonin and placebo.
USES IN CFS/ME. Sleep disturbance is one of the primary symptoms of CFS/ME. Many patients experience persistent insomnia throughout the illness. Even after a full night's rest, patients with CFS/ME awaken tired. Many clinicians believe that treating the CFS/ME sleep disorder is of primary importance because it reduces the severity of many other symptoms. However, owing to the prevalence of drug and chemical sensitivities in the CFS/ME population, it is not always easy to find a safe, effective means of obtaining a good night's rest. Melatonin may offer an alternative.
In 2006 van Heukelom et al explored the use of melatonin on CFS/ME patients with Dim Light Melatonin Onset (DLMO) later than 11:30 PM. DLMO is when the body begins its own production of melatonin. In healthy people, it occurs roughly two hours before bedtime, provided the light is dim. Van Huekelom's group found that in people with CFS/ME the delayed onset of DLMO was rectified by administration of 5 mg of melatonin five hours before DLMO. After three months, fatigue, energy, and concentration were significantly improved. The researchers concluded that melatonin was an effective therapy for those CFS/ME patients with significantly delayed sleep onset.
Although many CFS/ME physicians use melatonin, there is no clear evidence from the literature that melatonin levels are actually deficient in CFS/ME patients. In a study of 13 adolescents with CFS/ME, Knook et al found that melatonin levels were actually higher in the CFS/ME group than in controls.
506
There is a possible explanation for why some CFS/ME patients might be high in melatonin. Researchers have found that melatonin increases the release of cytokines, immune system chemicals that act as messengers to initiate various immune responses. In 1997 Garcia-Maurino et al found that melatonin increased the production of IL-2, IL-6 and gamma interferon, enhancing the effectiveness of Th1 (cellular) immunity (the type of immune function that combats viruses).
A previous study by Ben-Nathan et al found that injecting virus-infected mice with melatonin significantly reduced mortality rates. The implication for at least some people with CFS/ME is that the excess melatonin might be a response to reactivated viruses, providing a hormonal route to immune activation. In light of melatonin's role in enhancing cellular immunity, which is deficient in people with CFS/ME, this is an area which warrants further investigation, especially given the strong association between mono and CFS in teens.
PROTOCOL. Dr. Lapp uses melatonin with patients who have “phase shifted.” That is, they can't fall asleep until 1 or 2AM, and then sleep all day (indicating that the body's “clock” needs to be reset). He recommends starting with as little as 0.1 mg taken a half-hour before bedtime and increasing the dose until the desired effect is achieved. He also has observed that synthetic (not from animal sources) and sublingual forms of melatonin are safest and most effective (MEssenger, 1997). Dr. Lapp does not recommend melatonin for children younger than the late teens.
While product labels usually recommend one to two tablets (3 to 6 mg) taken before bedtime, studies at the Massachusetts Institute of Technology indicate 0.3 mg daily is sufficient to raise blood levels to normal. MIT researcher, Dr. Richard Wurtman, claims that serious side effects can be produced by taking standard doses, which can raise blood levels to more than 10 times the norm. Dr. Teitelbaum also agrees that the standard dose of 3 mg is too high. He recommends taking no more than 0.5 mg.
PROS. A number of CFS/ME patients have reported that melatonin has given them their best night's sleep in years. Melatonin works quickly. For people who become insomniacs while taking beta blockers, melatonin supplementation may provide considerable relief. (Beta blockers can deplete the body of melatonin.)
CONS. Melatonin can lose its effectiveness over time. After working beautifully for a few weeks or months, it can suddenly stop providing the desired results. Some people report paradoxical reactions, such as feeling more awake or experiencing partial or light sleep states. The reason melatonin works for some but not for others may have to do with individual biorhythms (see above). It is possible that patients with CFS/ME whose temperatures rise in the evening due to immune activation may not respond well to melatonin treatment.
Excessive doses of melatonin can cause jitters and headaches. Female patients may experience hormonal disturbances (early onset of periods). Interactions with antidepressant drugs such as Prozac, Elavil, or Zoloft and the pain medication, Ultram, have been reported. People taking antidepressants should
507
discuss the risks and benefits of melatonin with their physicians. Preexisting depression as well as orthostatic intolerance may be worsened by melatonin.
AVAILABILITY AND COST. Although it is a hormone, melatonin is currently considered a nutritional supplement. Consequently, it can be purchased over the counter from most health food stores and vitamin catalogs. A 100-tablet bottle of melatonin (3mg) can cost less than $5. Those who wish to start with lower doses should order the liquid.
FURTHER READING
“Sleep and Snake Oil.” Rachel Preiser. Discover Magazine. March 1997. http://discovermagazine.com/1997/mar/sleepandsnakeoil1082
Cort Johnson's informative page about melatonin in CFS/ME. http://aboutmecfs.org.violet.arvixe.com/Trt/TrtMelatonin.aspx
Dr. Lapp on melatonin and other sleep medications. http://www.prohealth.com/library/showarticle.cfm?libid=8563
Melatonin safety assessment by the Mayo Clinic. http://www.mayoclinic.com/health/melatonin/NS_patient-melatonin/DSECTION=safety
CFS/ME patient forum on melatonin: http://forums.phoenixrising.me/archive/index.php/t-12516.html?s=8dd572918a1b8e25a023bda45d398c90
RESEARCH Ben-Nathan D, Maestroni GJ, Lustig S, Conti A. “Protective effects of melatonin in mice infected with encephalitis viruses.” Arch Virol. 1995;140(2):223-30. http://www.ncbi.nlm.nih.gov/pubmed/7710351 (Abstract)
Carrillo-Vico A, Guerrero JM, Lardone PJ, Reiter RJ. “A review of the multiple actions of melatonin on the immune system.” Endocrine. 2005 Jul;27(2):189-200. http://www.ncbi.nlm.nih.gov/pubmed/16217132 (Abstract)
Garcia-Maurino S, MG Gonzalez-Haba, JR Calvo, M Rafii-El-Idrissi, V Sanchez- Margalet, R Goberna and JM Guerrero. “Melatonin enhances IL-2, IL-6, and IFN-gamma production by human circulating CD4+ cells: a possible nuclear receptor-mediated mechanism involving T helper type 1 lymphocytes and monocytes.” The Journal of Immunology, Vol 159, Issue 2 574-581, 1997. http://www.jimmunol.org/content/159/2/574.abstract (Abstract) Guerrero JM, Reiter RJ. “Melatonin-immune system relationships.” Curr Top Med Chem. 2002 Feb;2(2):167-79. http://www.ncbi.nlm.nih.gov/pubmed/11899099 (Abstract) Knook L, Kavelaars A, Sinnema G, Kuis W, Heijnen CJ. “High nocturnal melatonin in adolescents with chronic fatigue syndrome.” J Clin Endocrinol Metab. 2000 Oct;85(10):3690-2. http://www.ncbi.nlm.nih.gov/pubmed/11061525 (Abstract) Konturek PC, Brzozowski T, Konturek SJ. “Gut clock: implication of circadian rhythms in the gastrointestinal tract.” J Physiol Pharmacol. 2011 Apr;62(2):139-50. http://www.ncbi.nlm.nih.gov/pubmed/21673361 (Abstract)
508
http://www.jpp.krakow.pl/journal/archive/04_11/pdf/139_04_11_article.pdf (Full text) Lu WZ, Gwee KA, Moochalla S, Ho KY. “Melatonin improves bowel symptoms in female patients with irritable bowel syndrome: a double-blind placebo-controlled study.” Aliment Pharmacol Ther. 2005; 22: 927-934. http://www.ncbi.nlm.nih.gov/pubmed/16268966 (Abstract) Smits M G, Van Rooy R, Nagtegaal J E. “Influence of Melatonin on Quality of Life in Patients with Chronic Fatigue and Late Melatonin Onset.” J Chronic Fatigue Syndrome. 2002;10(3/4):25-32. 29. http://www.cfids-cab.org/cfs-inform/Melatonin/smits.etal02.pdf van Heukelom RO, Prins JB, Smits MG, Bleijenberg G. “Influence of melatonin on fatigue severity in patients with chronic fatigue syndrome and late melatonin secretion.” Eur J Neurol. 2006 Jan;13(1):55-60. http://www.ncbi.nlm.nih.gov/pubmed/16420393 (Abstract) Williams G, Waterhouse J, Mugarza J, Minors D, Hayden K. “Therapy of circadian rhythm disorders in chronic fatigue syndrome: no symptomatic improvement with melatonin or phototherapy.” Eur J Clin Invest. 2002 Nov;32(11):831-7. http://www.ncbi.nlm.nih.gov/pubmed/12423324 (Abstract)
MINERALS
Calcium, Magnesium, Selenium, Colloidal Silver, Zinc
CALCIUM
BACKGROUND. Calcium is the most abundant mineral in the human body. A 150-pound adult's body contains about three pounds of calcium, 99% of which is found in the skeletal bones. The small portion of calcium found in soft tissues and body fluids is essential for maintaining a number of important biochemical functions, including regular heartbeat and transmission of nerve impulses. Calcium also prevents muscle cramps and is vital for the formation of healthy teeth and strong bones.
There are two main forms of calcium: inorganic and organic. The inorganic forms (sulfate, carbonate, and phosphate) are poorly absorbed. The organic forms (citrate, lactate, gluconate, orotate, aspartate, ascorbate and various chelates) are better absorbed. Once calcium is metabolized through the action of stomach acid, it passes into the small intestine where the ionized (liquified) calcium is absorbed into the bloodstream. Ionized calcium is the most important physiological component of calcium. In fact, because calcium is so easily bound to other compounds, blood measurements of total calcium are useless for determining the amount of calcium actually available in the body. Only ionized calcium gives an accurate picture as to how much calcium is actually available to maintain physiological functions.
USES IN CFS/ME. CFS/ME patients often take calcium at night to alleviate insomnia. It is also useful for treating muscle spasms. Those ingesting high amounts of protein or phosphorus may want to supplement their intake of dietary
509
calcium because both protein and phosphorus increase calcium excretion from the body. Good natural sources of calcium are dairy products and green leafy vegetables.
PROTOCOL. Dr. Lapp recommends 1,000 mg to 1,500 mg daily. Calcium intake should not exceed 2500 mg a day. Calcium cannot be properly absorbed and assimilated unless vitamin D and trace minerals are present (chromium, boron, copper, iron, manganese, phosphorus, silicon, strontium, and zinc). It is important to supplement with these trace minerals while taking calcium, because calcium competes with other minerals for absorption in the intestines. It is also important to supplement with magnesium. (Magnesium prevents plaque buildup from unabsorbed calcium.)
Liquid ionic calcium is more easily absorbed and utilized than other forms of calcium. For example, only 10% of either calcium carbonate (Tums) or calcium citrate is absorbed. This means you get 100 mg of usable calcium for every 1,000 mg consumed. (You'd have to eat over 30 Tums to get 1000 mg of calcium.) Calcium lactate, found in milk, fares a little better at 33%. In contrast, calcium aspartate is 85% absorbed and calcium orotate is 90-95% absorbed. Ionic calcium is nearly 100% absorbed.
CFS/ME patients taking verapamil (a calcium channel blocker) to treat cognitive dysfunction need to be aware that calcium supplements may interfere with the effects of this medication. People with a history of kidney disease or kidney stones should not take calcium supplements, because the additional calcium may exacerbate the condition.
PROS AND CONS. Calcium is inexpensive and generally well tolerated. Calcium supplements can interfere with the absorption of both iron and zinc (but not magnesium), so if you are supplementing with either of these minerals, be sure to take them at least two hours after (or before) taking calcium.
AVAILABILITY AND COST. There is a wide variety of calcium supplements available at supermarkets, drug stores, health food stores, and from online distributors. Mineral Life sells an 8-oz bottle of liquid ionic calcium for $20 (60-day supply). Pure Essence markets Ionic Fizz (a blend of ionic trace minerals and vitamins) for $16 through Vitacost. Advanced Research markets a 100-tablet bottle of calcium orotate combined with magnesium for about $20 (through amazon.com). Advanced Research also markets a 100-tablet bottle of calcium aspartate for the very affordable price of $7.
FURTHER READING
Good overview of calcium, including rates of absorption for different calcium compounds. http://www.uswellnessmeats.com/Calcium_Myth_and_Facts.pdf
Brief interview with Dr. Spreen about the different forms of calcium and their bioavailability. http://www.alkalizeforhealth.net/Lcalcium.htm
Ionic calcium supplier: http://www.mineralifeonline.com/pd-calcium-8oz-60-day-supply.cfm
510
“When Is It Appropriate to Order an Ionized Calcium?” Laura M. Calvi and David A. Bushinsky. JASN July 1, 2008 vol. 19 no. 71257-1260. http://jasn.asnjournals.org/content/19/7/1257.full
Good medical article about the importance of measuring ionic calcium in the bloodstream.
MAGNESIUM
BACKGROUND. Magnesium is one of the six major minerals classified as essential for the functioning of the human body. The average human body contains about 25 grams of magnesium salts, about half of which is stored in the bones and one-fourth in muscle. Only about 2% circulates freely in the blood. The rest is located within the cells. Blood levels of magnesium are controlled by the kidneys.
Magnesium is necessary for relaying nervous system impulses and for normal metabolism of calcium and potassium. Much like a vitamin, magnesium functions as a coenzyme, aiding in enzyme systems, storage and release of energy generated from carbohydrates, and synthesis of proteins and DNA. Magnesium deficiency can result in anorexia, nausea, learning disabilities, personality changes, weakness, exhaustion, and muscle pain.
According to the USDA, a staggering 68% of Americans do not consume the daily recommended intake for magnesium. In a forward-looking article written in 1990, Kubena et al outlined the effects of chronic marginal intakes of magnesium, including “abnormalities in reproduction, growth, and development and disorders of neuromuscular, cardiovascular, renal, and immune function.” In addition, the authors pointed out that problems related to the use of pharmacological agents or trace metals, such as aluminum (which has been implicated in the development of Alzheimer's disease), may be worsened with a low intake of magnesium. Dr. Pall has speculated that, given the likelihood that people with CFS/ME are marginally deficient in magnesium before falling ill, magnesium deficiency may contribute to the pathogenesis of the illness.
USES IN CFS/ME. Magnesium is an indispensable supplement for people with CFS/ME. Nearly every CFS/ME physician includes either injectable or oral magnesium as part of their protocol. In early 1991, I.M. Cox, M.J. Campbell, and D. Dowson published a preliminary study on magnesium levels in CFS/ME patients (Lancet, 1991). All 22 patients studied had reduced levels of serum magnesium.
They followed up their findings with a randomized clinical study in which 15 of the patients received intramuscular injections of magnesium sulfate every week for six weeks and 17 received a placebo. Of the 15 patients receiving magnesium, 12 reported improvement in symptoms. Although subsequent studies have not confirmed low serum levels of magnesium to be universal among CFS/ME patients, magnesium is still the most frequently recommended mineral supplement for patients with CFS/ME.
In his book, Explaining “Unexplained Illnesses,” Dr. Martin Pall presents a compelling argument implicating oxidative stress in the etiology of CFS/ME. An important part of the ongoing oxidative stress typical of multisystem illnesses like
511
CFS/ME, FM and Gulf War Syndrome is the chronic excitability of NMDA receptors, which results in a hyperactive nervous system (along with cell damage, inflammation, and lowered production of ATP). Magnesium is one of the principal inhibitors of NMDA activity, which makes it a valuable treatment for any illness involving chronic oxidative stress.
Dr. Myhill believes that low magnesium levels in CFS/ME patients is a symptom of mitochondrial failure. When mitochondria fail, calcium leaks into cells and magnesium leaks out. According to Dr. Myhill, this leakage explains why it is useless to test serum levels of magnesium. As she puts it, “Serum levels are maintained at the expense of intracellular levels. If serum levels change this causes heart irregularities and so the body maintains serum levels at all cost. It will drain magnesium from inside cells and indeed from bone in order to achieve this.” Dr. Myhill's explanation not only accounts for why serum levels of magnesium are inconsistent in CFS/ME, but why magnesium supplementation is effective.
PROTOCOL. Magnesium can be administered orally or by injection. Because oral magnesium is difficult to absorb, the forms most frequently recommended are magnesium citrate and magnesium glycinate. Magnesium citrate will dissolve in water, which makes it more bioavailable than most other forms of magnesium. However, Dr. Cheney has observed that magnesium glycinate causes the least intestinal upset and is the most easily absorbed. The usual recommended dosage is 200 to 400 mg/day taken with food, although CFS/ME patients are cautioned to start with a smaller dose and increase it gradually. Intramuscular injections of 1 cc of magnesium sulfate (50%) or magnesium chloride can be administered once or twice a week. Because of magnesium's effect on heart function, the first injection should be performed in a physician's office.
PROS AND CONS. Most people who take magnesium, whether oral or injected, report increased stamina and energy. Many include better sleep as an additional benefit (most likely due to magnesium's muscle-relaxing effects). The main drawback of injected magnesium is that the injections are painful. The simultaneous administration of vitamin B12 or lidocaine helps relieve the pain of the injection. Because magnesium is a cathartic, high doses can cause diarrhea. In patients prone to gastrointestinal upset, a low dose is normally recommended.
AVAILABILITY AND COST. Oral magnesium is readily available from health food stores, online vitamin suppliers, and most drugstores. It is inexpensive. A bottle of 120 tablets of either magnesium glycinate or magnesium citrate (400 mg) costs $12 from Vitacost. Topical magnesium creams are also available. PureFormulas.com markets a 4-ounce jar of magnesium cream made by Kirkman for $16. (Or you can make your own cream using Epsom salts.) Magnesium can be purchased as a powder and mixed into a beverage for easier assimilation. Magnesium sulfate injections usually cost $16 to $20 per injection.
FURTHER READING
Excellent summary of magnesium's effects on the body from the Linus Pauling Institute. http://lpi.oregonstate.edu/infocenter/minerals/magnesium/
512
Dr. Myhill discusses magnesium deficiency and treatment in CFS/ME patients. http://www.drmyhill.co.uk/wiki/Magnesium_-_treating_a_deficiency
USDA statistics on nutrient consumption by state and nationally. http://www.ars.usda.gov/Services/docs.htm?docid=11197
“Review and Hypothesis: Might Patients with the Chronic Fatigue Syndrome Have Latent Tetany of Magnesium Deficiency.” Mildred Seelig, MD, MPH http://www.mgwater.com/clmd.shtml
RESEARCH
Cox IM, Campbell MJ, Dowson D. “Red blood cell magnesium and chronic fatigue syndrome.” Lancet. 1991 Mar 30;337(8744):757-60. http://www.ncbi.nlm.nih.gov/pubmed/1672392 (Abstract)
Kubena KS, Durlach J. “Historical review of the effects of marginal intake of magnesium in chronic experimental magnesium deficiency.” Magnes Res.1990 Sep;3(3):219-26. http://www.ncbi.nlm.nih.gov/pubmed/2132753 (Abstract)
Lindberg JS, Zobitz MM, Poindexter JR, Pak CY. “Magnesium bioavailability from magnesium citrate and magnesium oxide.” J Am Coll Nutr. 1990 Feb;9(1):48-55. http://www.ncbi.nlm.nih.gov/pubmed/2407766 (Abstract)
Manuel y Keenoy, B, Moorkens, G, Vertommen, J, Noe, M, Neve, J, and De Leeuw, I. “Magnesium status and parameters of the oxidant-antioxidant balance in patients with chronic fatigue: effects of supplementation with magnesium.” J Am Coll Nutr. 2000 Jun;19(3):374-82. http://www.ncbi.nlm.nih.gov/pubmed/10872900 (Abstract)
Seelig, Mildred MD, MPH. “Review and Hypothesis: Might Patients with the Chronic Fatigue Syndrome Have Latent Tetany of Magnesium Deficiency.” Journal of Chronic Fatigue Syndrome, Vol. 4(2) 1998 http://www.mgwater.com/clmd.shtml
SELENIUM
BACKGROUND. Selenium is a trace mineral found in the soil, and in foods such as lobster, tuna, shrimp, oysters, fish, brown rice, garlic, whole grains, sesame seeds, and mushrooms. Although it is needed in only small amounts, selenium performs an important role in kidney, spleen, pancreas and liver function, as well as in reproduction. In men, about half of the body's selenium is concentrated in the testes. Selenium forms a component of glutathione peroxidase, the body's most prolific antioxidant. Deficiencies in selenium can lead to infertility, arthritis, hypothyroidism (selenium is essential for making T3), loss of energy, immune system deficiency, and, in children, cardiac problems.
Apart from its many metabolic functions, selenium performs an important role in the functioning of the immune system. In a 1994 study performed at New York University, subjects who received a 200 mcg daily supplement of selenium for eight weeks showed an enhanced immune response to foreign antigens, including an increase natural killer cell activity. Research also indicates that selenium up-regulates IL-2 and increases activation of T helper cells. Selenium supplementation
513
may also down regulate abnormally high levels of the inflammatory cytokines IL-8 and TNF alpha.
It is because of selenium's dual function as an antioxidant and as an immune system enhancer that attention has recently been drawn to its possible role in the creation of “superbugs,” such as the Ebola virus. In the mid-1990s two researchers, Melinda Beck, a virologist at the University of North Carolina, and Orville Levander, a nutritional chemist with the USDA, set about to investigate the effects of selenium deficiencies on mice infected with Coxsackie virus. They discovered that not only did the mice develop virally induced heart disease, but that the virus itself had mutated into a more virulent strain.
Subsequent studies by Beck and colleagues confirmed that a host deficient in selenium not only has a poor immune response, but also can influence the genetic makeup of the virus, producing a more deadly strain. In an enormously understated conclusion, the authors stated that “this latter finding markedly changes our concept of host-pathogen interactions and creates a new paradigm for the study of such phenomena.” For those who have suffered for decades from the long-term effects of viral infections, the implications of this study are ominous.
USES IN CFS/ME. In CFS/ME, selenium is used primarily as an antioxidant. Selenium helps form glutathione peroxidases (which eliminate peroxide oxidants in the cell), as well as acting as a peroxynitrite scavenger. Both of these properties make selenium an important adjunct in antioxidant therapy. Selenium's role in thyroid hormone production also make it an essential supplement for people suffering from borderline hypothyroidism (a common finding in CFS/ME, due to disturbances in the endocrine system). Selenium has been identified as a mood enhancer as well.
In an interesting study of the psychological impact of selenium, Benton observed that “the metabolism of selenium by the brain differs from other organs in that at times of deficiency the brain retains selenium to a greater extent.” Benton proposed that this preference indicates that selenium is important in psychological function, particularly mood. In his article, Benton cites five studies that have associated low selenium intake with poorer mood. These studies seem to bear out independent reports from CFS/ME patients who have successfully taken selenium in place of antidepressants.
PROTOCOL. Dr. Pall recommends selenium methionine as the best form of selenium. Unless there is a verified selenium deficiency, low doses are recommended (50 mcg).
PROS AND CONS. Selenium is toxic at high levels, and overdoses can cause numerous symptoms: hair loss, tooth decay, brittle nails, nausea, vomiting, poor appetite, metallic taste in the mouth, loss of feeling in the hands and feet, and changes in skin pigmentation. (A garlic smell on the breath is an indication of excessive selenium intake.) Selenium is often produced as a yeast, which is problematic for people with Candida overgrowth and mold allergies, so check the label carefully.
514
AVAILABILITY AND COST. Selenium is widely available at health food stores and from online suppliers. PureFormulas.com markets a bottle of yeast-free seleno-methionine capsules (200 mcg) made by Douglas Labs for $26.40 (250 capsules). Capsules can be divided for a lower dose.
FURTHER READING
Detailed information about selenium from the Linus Pauling Institute.
http://lpi.oregonstate.edu/infocenter/minerals/selenium/
“Is Selenium Deficiency Behind Ebola, AIDS and Other Deadly Infections?” http://infonom.com.ar/task/html/selenium_deficiency_behind_tod.html
RESEARCH
Beck, Melinda A., Heather K. Nelson, Qing Shi, Peter Van Dael, Eduardo J. Schiffrin, Stephanie Blum, Denis Barclay, and Orville A. Levande. “Selenium deficiency increases the pathology of an influenza virus infection.” FASEB J. 2001 Jun;15(8):1481-3. http://www.fasebj.org/content/15/8/1481.full.pdf
Beck MA, Levander OA, Handy J. “Selenium deficiency and viral infection.” J Nutr. 2003 May;133(5 Suppl 1):1463S-7S. http://www.ncbi.nlm.nih.gov/pubmed/12730444 (Abstract)
Beck MA, Handy J, Levander OA. “Host nutritional status: the neglected virulence factor.” Trends Microbiol. 2004 Sep;12(9):417-23. http://www.ncbi.nlm.nih.gov/pubmed/15337163 (Abstract)
Benton D. “Selenium intake, mood and other aspects of psychological functioning.” Nutr Neurosci. 2002 Dec;5(6):363-74. http://www.ncbi.nlm.nih.gov/pubmed/12509066 (Abstract)
Kiremidjian-Schumacher L, Roy M, Wishe HI, Cohen MW, Stotzky G. “Supplementation with selenium and human immune cell functions. II. Effect on cytotoxic lymphocytes and natural killer cells.” Biol Trace Elem Res. 1994 Apr-May;41(1-2):115-27. http://www.ncbi.nlm.nih.gov/pubmed/7946899 (Abstract)
COLLOIDAL SILVER
NOTE: Some of the colloidal minerals distributed by multilevel marketers contain arsenic and lead, which are toxic even in small doses. Caution should be exercised. Read labels carefully!
DESCRIPTION. Colloidal silver solution is composed of ultrafine, non-soluble particles of silver suspended in a liquid medium such as water.
BACKGROUND. Colloidal silver has long been used as a germicide. In the early twentieth century, colloidal silver was used in place of antibiotics. Silver was used orally, intravenously, and intramuscularly (as an injection), as a throat gargle, and in eyedrops. Colloidal silver has been used to treat such varied maladies as tonsillitis, cystitis, ringworm, and dysentery. Over the course of this century,
515
antibiotics have replaced silver as drugs of choice, although silver nitrate is still used to prevent eye infection in newborn infants.
USES IN CFS/ME. Some patients with CFS/ME report that colloidal silver helps control recurring infections, particularly in the mouth. Research has shown that colloidal silver may be of benefit in treating oral infections, sinusitis, sore throat, and canker sores.
PROTOCOL. Dosage varies, depending on the concentration of the product used.
PROS AND CONS. It appears that low doses of silver are fairly safe. However, argyria (grayish skin discoloration) may develop when excessive doses of silver are ingested. Because most studies evaluating the antimicrobial properties of silver are not conducted on people, patients are cautioned to exercise judgment before choosing silver over a medication whose mode of action and recommended dosage are better known.
AVAILABILITY AND COST. Colloidal silver may be purchased from most health food stores and online distributors. It costs $12 to $25 for a 4-oz bottle, depending on the brand. Some companies make a spray colloidal silver for oral use. Stick to reputable brands such as Source Naturals when purchasing.
RESEARCH
Damiani V, Di Carlo M, Grappasonni G, Di Domenico R, Dominici P. “Efficacy of a new medical device based on colloidal silver and carbossimetyl beta glucan in treatment of upper airways disease in children.” Minerva Peditr. 2011 Oct;63(5):347-54. http://www.ncbi.nlm.nih.gov/pubmed/21946445 (Abstract)
Eby DM, Luckarift HR, Johnson GR. “Hybrid antimicrobial enzyme and silver nanoparticle coatings for medical instruments.” ACS Appl Mater Interfaces. 2009 Jul;1(7):1553-60. http://www.ncbi.nlm.nih.gov/pubmed/20355960 (Abstract)
Khan SS, Mukherjee A, Chandrasekaran N. “Studies on interaction of colloidal silver nanoparticles (SNPs) with five different bacterial species.” Colloids Surf B Biointerfaces. 2011 Oct 1;87(1):129-38. http://www.ncbi.nlm.nih.gov/pubmed/21640562 (Abstract)
Lansdown AB. “Silver in health care: antimicrobial effects and safety in use.” Curr Probl Dermatol. 2006;33:17-34. http://www.ncbi.nlm.nih.gov/pubmed/16766878 (Abstract)
Monteiro DR, Gorup LF, Silva S, Negri M, de Camargo ER, Oliveira R, Barbosa DB, Henriques M. “Silver colloidal nanoparticles: antifungal effect against adhered cells and biofilms of Candida albicans and Candida glabrata.” Biofouling. 2011 Aug;27(7):711-9. http://www.ncbi.nlm.nih.gov/pubmed/2175619 2 (Abstract)
ZINC
BACKGROUND. Zinc is a remarkably versatile mineral. It plays an important role in the more than 70 enzyme systems that regulate most metabolic processes. It stimulates digestion, aids in extracting stores of vitamin A from the
516
liver, helps maintain the mucous lining of the mouth, throat, stomach, and intestines, is vital for the normal growth of hair, skin, and nails, controls sexual maturation and fertility (zinc deficiency in men can lead to infertility), and aids in the healing of wounds. Zinc is necessary for the utilization of vitamin B6, a vitamin which is crucial for nervous system function. It also helps improve immune responses, although excessive intake of zinc (more than 50 mg) can suppress immune function. (High doses of zinc also deplete copper.)
USES IN CFS/ME. Many CFS/ME patients take zinc to help relieve sore throat and other viral symptoms. In a 2005 study published by Maes et al, 33 CFS/ME patients were examined for serum zinc deficiencies. The researchers found that serum levels of zinc were lower in CFS/ME patients than in controls. In addition, low serum zinc status was related to signs of inflammation and defects in early T cell activation pathways. Since zinc is a strong antioxidant, the results of this study support the findings that CFS is accompanied by increased oxidative stress. The researchers concluded that “the results of these reports suggest that some patients with CFS should be treated with specific antioxidants, including zinc supplements.”
PROTOCOL. The recommended daily allowance for zinc is 15 mg. The most bioavailable form is high-zinc yeast. This is a form of yeast that has a high zinc content. Unfortunately, it is not available in the U.S. (Lalmin Zn, a high-zinc yeast supplement using Saccharomyces cerevisiae, is produced in Denmark.) Zinc picolinate is well-absorbed, as is zinc citrate. Zinc carnosine, a combination of zinc and the amino acid carnosine, is reported to be well absorbed, as well as providing support for the mucosal lining of the stomach and gut.
AVAILABILITY AND COST. Zinc is available from health food stores, vitamin catalogs, and some drugstores. As with other mineral supplements, it is not expensive. A 100-tablet bottle of zinc picolinate (25 mg) made by Country Life costs less than $5 on Vitacost. Zinc should be taken with food to avoid stomach upset. Zinc is found naturally in pumpkin seeds, liver, egg yolks, and seafood (especially oysters).
FURTHER READING
Essential reading about zinc: http://ods.od.nih.gov/factsheets/Zinc-HealthProfessional/
Article discussing zinc bound in yeast: http://www.nutraingredients.com/Research/Zinc-bound-in-yeast-promotes-superior-bioavailability-claims-study
Interesting study of high-zinc yeast in rats: http://www.beta-glucan-info.com/pdf/Zinc_Bioavailability.pdf
RESEARCH
Maes, Michael, Ivana Mihaylova, Marcel De Ruyter. “Lower serum zinc in Chronic Fatigue Syndrome (CFS): Relationships to immune dysfunctions and relevance
517
for the oxidative stress status in CFS.” Journal of Affective Disorders. 2006 Feb;90(2-3):141-7. http://cfids-cab.org/cfs-inform/Hypotheses/maes.etal05.pdf
Mahmood A , A J FitzGerald, T Marchbank, E Ntatsaki, D Murray, S Ghosh, and R J Playford. “Zinc carnosine, a health food supplement that stabilises small bowel integrity and stimulates gut repair processes.” Gut. 2007 February; 56(2): 168–175. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1856764/
MONOLAURIN
DESCRIPTION. Monolaurin is a mono-ester formed from glycerol and lauric acid.
BACKGROUND. Monolaurin is a fatty acid found in human breast milk. Lauric acid, a closely related compound, is found in coconuts. It has broad anti-microbial properties. In in vitro studies, monolaurin was able to destroy several strains of bacteria. H. Pylori is particularly susceptible – which may be why coconut water is traditionally used as a treatment for dyspepsia in tropical countries.
Other in vitro studies have shown that monolaurin can kill viruses by destroying their lipid membrane. (Laurates are commonly found in soap.) Some of the viruses inactivated by these lipids are measles, herpes simplex, hepatitis C, and cytomegalovirus (CMV). A number of fungi, yeasts, and protozoa are also inactivated or killed by monolaurin. These include ringworm, Candida albicans, and the protozoan parasite Giardia lamblia. Among the many benefits of monolaurin is the fact that it can destroy harmful bacteria without affecting beneficial intestinal flora.
USES IN CFS/ME. Monolaurin is an antiviral, antifungal and anti-Candida treatment. It is used as a safe alternative to pharmaceutical antivirals and antifungals, which often have harmful side effects.
PROTOCOL. Physicians advise starting with very low doses (¼ scoop of Lauricidin) to prevent Herxheimer, or “die-off,” reactions. The makers of Lauricidin recommend starting with one pellet a day (approx 30 mg) in order to avoid Herxheimer reactions. Do not chew the pellets. (They taste like soap.) Monolaurin capsules can be taken with greater frequency. Dr. Teitelbaum recommends taking 9 capsules (300 mg) once a day on an empty stomach for 1 week, followed by 6 capsules once a day for 20 days. He recommends taking lysine 1500 mg twice a day while on monolaurin.
PROS AND CONS. Patients report that monolaurin helps ward off colds and flus. One patient wrote that at high doses (500 mg) it helped shingles. However, most patients report that monolaurin will cause “die off” (Herxheimer-like) reactions. Some fibromyalgia patients have reported an increase of pain on even very low doses of Lauricidin. Other side effects include acid reflux and a general “sick” feeling.
AVAILABILITY AND COST. Patients recommend purchasing pure monolaurin (Lauricidin). An 8-oz container of Lauricidin pellets can be purchased for around $30 on amazon.com. Ecological Formulas markets two monolaurin
518
combinations (one with magnesium, and one with lysine) for roughly $13 for a 90-capsule bottle (through PureFormulas.com online).
FURTHER READING
A Review of Monolaurin and Lauric Acid. Shari Lieberman and Harry Preuss. http://www.easihealth.co.za/wordpress/wp-content/uploads/downloads/2011/02/trials/Monolaurin.pdf
Patient thread on monolaurin: http://www.prohealth.com/me-cfs/blog/boardDetail.cfm?id=428991
Manufacturer's information on Lauricidin: http://lauricidin.com/tech_data/
RESEARCH
Preuss HG, Echard B, Enig M, Brook I, Elliott TB. “Minimum inhibitory concentrations of herbal essential oils and monolaurin for gram-positive and gram-negative bacteria.” Mol Cell Biochem. 2005 Apr;272(1-2):29-34.http://www.ncbi.nlm.nih.gov/pubmed/16010969 (Abstract)
Zhang H, Wei H, Cui Y, Zhao G, Feng F. “Antibacterial interactions of monolaurin with commonly used antimicrobials and food components.” Journal of Food Science. 2009 Sep;74(7):M418-21. http://www.ncbi.nlm.nih.gov/pubmed/19895490 (Abstract)
MUSHROOM EXTRACTS
LEM (shiitake), Maitake, Cordyceps
Mushroom extracts have become increasingly popular in recent years for their broad medicinal properties. Research has shown that mushroom extracts have anticancer, anti-diabetes, antibacterial, antifungal, and immune stimulating properties. Although many varieties of mushroom extracts are currently marketed for their medicinal effects, the two mushroom extracts most widely used for CFS/ME are the shiitake (LEM) and maitake.
In 2002 Dr. Peter R. Rothschild conducted a 120-day study to observe therapeutic responses to RM-10 (a combination of 10 mushroom extracts) for the reduction of symptoms in 33 CFS/ME patients. The researchers found that 60% of the participants reported a reduction of symptoms by 40%, with 33% totally asymptomatic by the end of the trial period. All participants reported some degree of improvement. Dr. Rothschild stated, "We had highly significant results with the multi-mushroom formula, brand named RM-10 [TM]. For affected patients, there was a remarkable percentage of remissions and a quite noticeable improvement in symptomology overall.”
FURTHER READING
Good general information about mushroom extracts. http://www.nammex.com/MedicinalMushroomBooks.html
519
Report on RM-10 mushroom extract administered to CFS/ME patients. http://findarticles.com/p/articles/mi_m0ISW/is_2002_August-Sept/ai_90794449/
Description of RM-10: http://www.healthfoodemporium.com/garden-of-life/rm_10.html
SHIITAKE (LEM)
DESCRIPTION. LEM (Lentinus edodes mycelium) is an extract made from the immature shiitake mushroom.
BACKGROUND. Although shiitake mushrooms have long been used in the East for culinary purposes, they have recently gained attention for their medicinal value. Numerous studies, mostly conducted in Japan, have demonstrated that LEM increases immune system function by stimulating production of lymphocytes and macrophages, the immune system's defense against bacteria, viruses, and tumor cells. LEM may also interfere with the action of reverse transcriptase (an enzyme that aids in viral replication) and block cell receptor sites of viruses. Owing to these properties alone, LEM shows promise in treating cancer, diseases related to immune system dysfunction, and viral infections.
USES IN CFS/ME. Most patients with CFS/ME use LEM as a general treatment for lethargy, weakness, and exhaustion, three primary symptoms of CFS/ME. A number have reported improvement in stamina, energy, and strength, decreased diarrhea, and increased white blood cell count after taking LEM.
PROTOCOL. Shiitake extract is usually sold in liquid or tablet form. The suggested dose is 40 drops of liquid, taken twice daily. Up to eight tablets may be taken a day. As with other medications, patients with CFS/ME should start with smaller doses and gradually increase to the full dose.
PROS AND CONS. LEM is one of the few botanical products that affects CFS/ME as a whole. A number of patients report general improvement and lessening of some of their worst symptoms. LEM may provoke a severe allergic reaction in patients with allergies to mushrooms, molds, and other fungi. Those with recurring yeast infections, athlete's foot, or thrush should probably delay trying LEM until these problems are resolved.
AVAILABILITY AND COST. Shiitake extracts are widely available in health food stores and through internet suppliers. Vitacost sells a 2-oz bottle of pure shiitake extract made by Planetary Herbals for $12. Source Naturals markets a bottle of 40 tablets for about $15.
FURTHER READING
“Mushroom Extracts: Exciting News for Good Health.” Neenyah Ostrom's article on LEM and CFS/ME. http://www.immunesupport.com/news/93fal003txt.htm
Sloan Kettering's very thorough review of shiitake extract: http://www.mskcc.org/cancer-care/herb/shiitake-mushroom
MAITAKE EXTRACT
BACKGROUND. The maitake (Grifola frondosa) is a large mushroom that resembles Elizabethan neck ruffles. It grows in clusters at the base of oak trees in
520
Japan and North America. Maitake mushrooms are used in Asian cuisine, and because of their size (up to 50 pounds) are known as the “king” of mushrooms. Maitake mushrooms are rich in nutrients, including B vitamins, magnesium, potassium, and calcium.
In the late 1980s an active constituent in maitake, a beta-glucan compound, was found to enhance immune activity. Studies have shown that whole maitake also has the ability to regulate blood sugar and blood pressure, as well as insulin, lipids and cholesterol. Recent research has shown that maitake also has antioxidant and anticancer properties.
USES IN CFS/ME. People with CFS/ME use maitake extract as an immune system stimulator, particularly of NK (natural killer) cells. (Low NK cell activity has been well documented among CFS/ME patients.)
PROTOCOL: Maitake capsules should be taken on an empty stomach. The standard dose for 300 mg capsules is one to three capsules taken twice daily.
AVAILABILITY AND COST. Iherb.com markets a full spectrum maitake extract made by Mushroom Science for $24 for a bottle of 90 capsules.
FURTHER READING
Extensive list of many maitake extracts: http://www.vitasprings.com/maitake.html
RESEARCH
Yeh JY, Hsieh LH, Wu KT, Tsai CF. “Antioxidant properties and antioxidant compounds of various extracts from the edible basidiomycete Grifola frondosa (Maitake).” Molecules. 2011 Apr 15;16(4):3197-211. http://www.ncbi.nlm.nih.gov/pubmed/21499220 (Abstract)
CORDYCEPS
BACKGROUND. Cordyceps is a fungus that grows on the larvae of the caterpillar, Hepialus armoricanus Oberthuer, found in China and Tibet. (Traditionally, the product contains both the fungus and its caterpillar host.) Cordyceps has been used in China to treat a wide range of conditions including fatigue, sexual dysfunction, and coughs. It is an adaptogen and immune stimulant.
Cordyceps has also been found to increase red blood cells, and to stimulate the production of testosterone (which is perhaps why it is used for sexual dysfunction). Research conducted primarily in China has also found cordyceps beneficial in increasing cellular oxygen absorption, protecting the liver, enhancing the immune system (by increasing natural killer cell activity), and improving shortness of breath and fatigue in patients suffering from chronic heart failure.
PROS AND CONS. CFS/ME patients have reported that cordyceps gives them a boost. It also reduces “air hunger” and increases stamina.
MORE INFORMATION
Sloan-Kettering's page on cordyceps: http://www.mskcc.org/cancer-care/herb/cordyceps
521
“Dr Oz: Chronic Fatigue Syndrome, Cordyceps & D5 Ribose Sweetener.” http://www.drozfans.com/dr-ozs-advice/dr-oz-chronic-fatigue-syndrome-cordyceps-d5-ribose-sweetener/
“Cordyceps Chinensis.” Everything you could possibly want to know about Cordyceps. http://mdidea.com/products/herbextract/cordyceps/data06.html
“Mushroom remedy 'makes you fit' A Chinese mushroom improves the fitness of middle-aged and elderly people, research suggests.” http://news.bbc.co.uk/2/hi/health/3638543.stm
NAC (N-acetylcysteine )
DESCRIPTION. N-acetylcysteine (NAC) is a derivative of cysteine, an amino acid.
BACKGROUND. NAC acts as an antioxidant, and is a precursor to glutathione. Clinically, it has been used to treat acetaminophen (paracetamol in Britain) overdose. It has also been used to reduce the viscosity of mucus in pulmonary conditions such as pneumonia, bronchitis, emphysema and tuberculosis. NAC is commonly used in patients with renal impairment. It is being explored as a possible treatment for both schizophrenia and bipolar disorder. NAC's ability to counteract glutamate hyperactivity in the brain also make it a good candidate for treating obsessive-compulsive disorder. NAC is also a chelating agent for mercury, and can be used for mercury toxicity.
USES IN CFS/ME. NAC can inhibit muscle fatigue after exercise. Reid et al, in a 1994 study, showed that pre-treatment with NAC improved performance of muscles during exercise. They suggested that “oxidative stress plays a causal role in the fatigue process” and that NAC “may be useful clinically.”
Research on NAC has shown that it is effective in reducing depletion of glutathione. People with CFS/ME are demonstrably low on glutathione. However, direct supplementation with glutathione is problematic because glutathione is rapidly broken down in the gut. Taking glutathione precursors, such as NAC, allows the body to synthesize glutathione on its own.
PROTOCOL. Martin Pall has speculated that because NAC rapidly releases cysteine, it may cause neural excitotoxicity. He recommends using NAC at low doses.
PROS AND CONS. NAC is generally well tolerated. However, in those who are sensitive to stimulants, it can cause insomnia and headaches. NAC is contraindicated for people with kidney stones.
AVAILABILITY AND COST. NAC is available at health food stores and from online suppliers. It is inexpensive. A 60-capsule bottle of Carlson NAC (500 mg) costs about $8 (through Vitacost).
FURTHER READING
Kelly GS. “Clinical applications of N-acetylcysteine.” Altern Med Rev. 1998 Apr;3(2):114-27. http://www.ncbi.nlm.nih.gov/pubmed/9577247 (Abstract)
522
Kerksicki, Chad and Darryn Willoughby. “The Antioxidant Role of Glutathione and N-Acetyl-Cysteine Supplements and Exercise-Induced Oxidative Stress.” Journal of the International Society of Sports Nutrition 2005, 2:38-44. http://www.jissn.com/content/2/2/38 (This is a review of research into glutathione and NAC in exercise-induced muscle fatigue.)
Reid MB, Stokić DS, Koch SM, Khawli FA, Leis AA. “N-acetylcysteine inhibits muscle fatigue in humans.” J. Clin. Invest. 1994 Dec;94(6):2468-74. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC330079/
NADH (ENADA)
DESCRIPTION. NADH is the reduced form of nicotinamide adenine dinucleotide (NAD), also called ubiquinone reductase. It is found in all living cells.
BACKGROUND. NADH was first discovered in the 1930s by an American scientist who observed that NADH played an essential role in the energy production of cells. It was not until more than 60 years had passed, however, that Dr. Georg Birkmayer, a biomedical researcher from Vienna, Austria, developed a stable oral form of NADH. Since then, a growing body of research has documented that NADH not only acts as a driving force in the production of cellular energy, but also is a potent antioxidant, is a key component of DNA repair and cellular regeneration, and stimulates the production of the neurotransmitters dopamine, noradrenaline, and serotonin. Ongoing research in the United States and abroad may help define the role of NADH in treating such degenerative neurological conditions as Alzheimer's disease and Parkinson's disease.
USES IN CFS/ME. NADH may be of great benefit in treating CFS/ME. When NAD is oxidized (NAD+) in the cell's mitochondria, energy is released. This energy is preserved in the form of adenosine triphosphate (ATP), a substance required by all energy-absorbing processes in the body.
Researchers have proposed that NADH may help correct the metabolic defect in CFS/ME that inhibits the production of ATP. Because low ATP production means less energy, clinicians believe NADH may alleviate CFS/ME-related exhaustion and may also improve cognitive function. The three neurotransmitters stimulated by NADH serve critical functions in the central nervous system: dopamine is important for short-term memory; noradrenaline contributes to alertness; and serotonin has a pronounced effect on mood and regulates sleep.
In 1999 Forsyth et al conducted a trial of NADH (as ENADA, a stable, bioavailable form of NADH) on 26 CFS/ME patients. Thirty-six percent of the CFS/ME patients taking NADH responded favorably, as opposed to 8% on placebo. No adverse effects were noted. In a longer term, open-label phase of the study, Birkmayer reports that “72% of the patients continued to report an improvement of their symptoms after six months of taking 10 mg ENADA daily. After approximately one year of taking ENADA the research doctors are reporting up to 81 percent of the patients continue to benefit from ENADA. These findings suggest that long-term ENADA therapy can lead to continued improvements, especially in energy and mental/ cognitive status.”
523
While these results looked promising, there has been little follow-up on the initial trial with ENADA. Dr. Myhill lists ENADA as one of the CFS treatments “not worth trying” (along with graded exercise, CBT, and cold baths). As Dr. Myhill puts it, “It is the old story - single interventions are highly unlikely to result in worthwhile improvements because CFS is a complex problem - it is the combined approach that gets the results.”
PROTOCOL. Although Forsyth et al used 10 mg a day, the suggested starting dosage of NADH is 5 mg/day, (though some people report taking as much as 15 mg). The dosage is dependent on weight. Heavier people will need a higher dose to see an effect. NADH should be taken first thing in the morning on an empty stomach (about 20 minutes before your first meal).
Dr. Lapp recommends NADH in combination with acetyl-L-carnitine for his patients with severe “brain fog.” He observes that it can take three to six months to produce a response. Dr. Lapp recommends a dosage of 10 to 20 mg per day.
Patients note that sublingual NADH tablets are more effective than oral forms.
PROS AND CONS. Some patients report that NADH is moderately to mildly helpful, "making bad days somewhat less bad and good days somewhat better" (CFIDS Chronicle, Summer 1996). The majority of patients who take NADH note that it helps with cognitive symptoms more than fatigue.
AVAILABILITY AND COST. NADH is classified as a supplement and therefore does not require a prescription. Source Naturals sells a 60-tablet bottle of reduced Enada-NADH (5 mg) for $40 through Vitacost. PureFormulas.com sells a 30-tablet (10 mg) pack made by Physiologics for $38.50. Vitacost's own brand of sublingual NADH (10 mg) costs $20 for a packet of 30 tablets. A 30-tablet box of 5 mg ENADA costs $22.25 through the official ENADA website.
MORE INFORMATION
The official ENADA site, containing product and brand information: http://www.enada.com/
FURTHER READING
Dr. Birkmayer's review of ENADA, including summaries of trials, and recommended dosage. http://www.encognitive.com/node/5059
Patient thread on NADH. Includes references to several studies, responses and dosage. http://forums.phoenixrising.me/archive/index.php/t-5096.html
RESEARCH
Forsyth LM, Preuss HG, MacDowell AL, Chiazze L Jr, Birkmayer GD, Bellanti JA. “Therapeutic effects of oral NADH on the symptoms of patients with chronic fatigue syndrome.” Ann Allergy Asthma Immunol. 1999 Feb;82(2):185-91. http://www.ncbi.nlm.nih.gov/pubmed/10071523 (Abstract)
PROBIOTICS
524
DESCRIPTION. Probiotic bacteria, primarily Lactobacillus acidophilus and Bifidobacterium bifidus, aid in many digestive processes and help maintain balance in the intestines.
BACKGROUND. Digestive tract bacteria (intestinal flora) have evolved within humans to aid in completing the breakdown and absorption of many foods. Without the thousands of "friendly" bacteria that inhabit the intestines, malnutrition would develop no matter how much food was eaten. These bacteria not only aid in digestion, but are responsible for manufacturing many nutrients that are essential to survival, such as the B vitamin complex. Some bacteria, such as bifidus, live in the large intestine; others, such as acidophilus, live in the small intestine.
As long as the intestinal flora are working well, a minimum of digestive problems can be expected. However, once the function of friendly flora is upset, harmful bacteria can proliferate, causing bloating, stomach upset, poor digestion, constipation, gas, and malabsorption problems. The most common sources of flora upset are recurrent use of antibiotics, oral contraceptives, aspirin, corticosteroids, poor diet, stress, and Candida infections. In these cases, it may be necessary to use a probiotic supplement to reestablish a healthy balance of intestinal flora.
A number of studies have shown that intestinal flora are effective for treating intestinal problems. In a review of probiotic treatments for diarrhea, Guandalini found that several strains of probiotics, including Lactobacillus GG, Lactobacillus acidophilus, Lactobacillus casei, Bifidobacterium ssp, Streptococcus ssp, and the yeast Saccharomyces boulardii, were effective in combating diarrhea due to antibiotics, C. difficile and viruses. Two strains, Lactobacillus GG and Saccharomyces boulardii were particularly effective. Researchers have also found probiotics helpful in treating irritable bowel syndrome and inflammatory bowel disease, suggesting a possible link between these two conditions.
USES IN CFS/ME. Patients with gastrointestinal symptoms or recurring yeast infections, or who regularly take antibiotics, nonsteroidal anti-inflammatory drugs (NSAIDs), oral contraceptives, or cortisone are advised to use a probiotic supplement. Products that contain bifidus seem to help with leaky gut.
Generally, people with CFS/ME appear to suffer from a deficiency in friendly flora. According to a study by Butt et al in Australia, the colonic bacterial population in CFS/ME patients is deficient in Bifidobacterium and E. Coli. In contrast, the lactic acid bacteria, Enterococcus, is significantly higher – 28.7% of the total aerobic flora in CFS/ME patients – than in the healthy subjects (3-5%).
Remarkably, the researchers found that specific changes in gastrointestinal flora were associated with CFS/ME symptoms. A high enterococcal count positively correlated with neurological and cognitive functions: nervousness, memory loss, forgetfulness, confusion, and “mind going blank.” Similarly a high aerobe/anaerobe ratio significantly correlated with poor colonic functions, poor digestion, and malabsorption of the gastrointestinal tract. The implications of this study are that the composition of bacterial flora has a significant impact on both digestion and the nervous system, and that in people with CFS/ME the two are linked.
525
In an interesting paper published in 2003, Logan et al proposed that probiotics might serve to enhance immune function in people with CFS/ME. The authors pointed out that people with CFS/ME have marked alterations in intestinal flora as well as oxidative stress. They state that “lactic acid bacteria (LAB) have the potential to influence the immune system in CFS patients by supporting . . . cellular immunity and may decrease allergies. In addition LAB are strong antioxidants, may improve EFA status, can enhance absorption of micronutrients by protecting the intestinal epithelial barrier.” The authors suggested that lactic acid bacteria might have a therapeutic role in the treatment of CFS/ME.
Probiotics may be useful for other reasons as well. Due to disruptions in the balance of neurotransmitters which are responsible for maintaining gut motility, people with CFS/ME often have motility problems. When motility is slowed, the bacteria from the large intestine can travel upward, where they colonize the small intestines. This leads to a condition known as SIBO (small intestinal bacterial overgrowth). Once established in the small intestines, the bacteria interfere with the breakdown of fats and carbohydrates. According to Dr. Cheney, a significant percent of the CFS/ME population suffers from SIBO. The standard treatment for SIBO is antibiotics, which, ironically, are also the primary cause of SIBO. Many gastroenterologists recommend treatment with probiotics, in particular Lactobacillus GG for SIBO in order to restore beneficial flora after antibiotic treatment.
PROTOCOL. Probiotics are sold in different forms. Each should be taken according to directions. Enteric-coated tablets, for example, need to be taken only once a day and can be taken with food, because the enteric coating protects the bacteria from being destroyed by stomach acids. Patients with altered intestinal flora as a result of taking antibiotics need to take a probiotic supplement for a least two weeks after finishing the treatment to repopulate the intestines. Single-strain varieties are reported to be more effective than multiple strains.
PROS. Most patients with CFS/ME who regularly take probiotics report easing of gastrointestinal symptoms (especially gas and bloating) and overall improvement in digestion. One of the main advantages of probiotics is that they can be taken daily for months, or even years, without causing any adverse effects or loss of benefits. They rarely cause side effects and are safe for children.
CONS. Probiotics are not without risk. There is some concern in the medical community about the safety of probiotic supplements (which is why it is important to purchase reputable brands). Probiotics should be used to caution in individuals with an abnormal gastrointestinal mucosal barrier (leaky gut), due to the risk of the bacteria penetrating the intestinal wall. Some people with CFS/ME who have been diagnosed with SIBO sometimes report experiencing flares and “brain fog” after taking probiotics, especially if the initial infection has not been eradicated.
AVAILABILITY AND COST. Many good brands of probiotic supplements can be purchased from health food stores and vitamin catalogs. Vitacost sells a package of 30 capsules of Culturelle (Acidophilus GG) for $15. Vitacost sells a 50-capsule bottle of Saccharomyces boulardii made by Allergy Research Group for about the same price.
Acidophilus can also be found in foods such as yogurt and kefir, although these are more effective at maintaining intestinal balance once it has been corrected. Foods such as miso and tofu can enhance bifidus growth, as can a number of vegetables that provide intestinal substrate (fructo-oligosaccharides (FOS) and inulin) in which the bacteria can flourish.
FURTHER READING
CFS/ME forum discussing some of the risks of probiotics. http://forums.phoenixrising.me/archive/index.php/t-8976.html
“Intestinal Flora.” Very good website with research and specific information on intestinal flora. http://www.probiotic.org/intestinal-flora.htm
"Probiotics in Clinical Practice: An Update." Good general information about the clinical use of probiotics: http://www.ecologyhealthcenter.net/node/839
“An Emerging Trend of High Dose Probiotic Use in Clinical Practice- A Brief Survey.” October 2011. http://www.pointinstitute.org/resources/Point+Inst.+High+Dose+Probiotics+Oct.+2011.pdf
Hibberd, Patricia L., Lisa E. Davidson. “Safety of probiotics.” http://chemistry-today.teknoscienze.com/pdf/HIBBERD%20AGRO4-08.pdf
Taylor C Wallace, Francisco Guarner, Karen Madsen, Michael D Cabana, Glenn Gibson, Eric Hentges, Mary Ellen Sanders. “Human gut microbiota and its relationship to health and disease.” Nutrition Reviews, Volume 69, Issue 7, pages 392–403, July 2011. http://onlinelibrary.wiley.com/doi/10.1111/j.1753-4887.2011.00402.x/full
RESEARCH
Butt H. L., Dunstan R. H., McGregor N. R., Roberts T. K. “Bacterial colonosis in patients with persistent fatigue.” Proceedings of the AHMF International Clinical and Scientific Conference; 2001 Dec 1–2; Sydney, Australia. http://www.ahmf.org/01access/01butt.html
Gibson GR, Beatty ER, Wang X, Cummings JH. “Selective stimulation of bifidobacteria in the human colon by oligofructose and inulin.” Gastroenterology. 1995 Apr;108(4):975-82. http://www.ncbi.nlm.nih.gov/pubmed/7698613 (Abstract)
Guandalini S. “Probiotics for prevention and treatment of diarrhea.” J Clin Gastroenterol. 2011 Nov;45 Suppl:S149-53. http://www.ncbi.nlm.nih.gov/pubmed/21992955 (Abstract)
Logan, Alan C., A. Venket Rao, Dinaz Irani. “Chronic fatigue syndrome: lactic acid bacteria may be of therapeutic value.” Medical Hypotheses (2003) 60(6), 915–92. http://www.cfids-cab.org/cfs-inform/Hypotheses/logan.etal03.pdf
527
Ku WH, Lau DCY, Huen KF. “Probiotics Provoked D-lactic Acidosis in Short Bowel Syndrome: Case Report and Literature Review.” HK J Paediatr (New Series) 2006;11:246-254. http://hkjpaed.org/details.asp?id=577&show=1234
PIRACETAM (Nootropil, Lucetam)
DESCRIPTION. Piracetam is a derivative of GABA (gamma-aminobutyricacid), the brain's primary neuroinhibitory amino acid.
BACKGROUND. Piracetam is a nootropic, or “smart drug.” It has been used for a wide range of neurological impairments, including seizures, dementia, focal lesions in the brain, and concussions. There is also evidence that it can enhance cognitive performance among the healthy. In a study by Dimond and Brouwers, administration of piracetam for 14 days improved verbal memory in a group of college students. Piracetam appears to work not just by acting on cholinergic receptors, but by decreasing the viscosity of blood, which, in turn, enhances the delivery of oxygen to the brain.
USES IN CFS/ME. Piracetam is used more widely in Europe than in the U.S., where the FDA has determined that because it is not a vitamin, mineral, amino acid, herb, botanical, or other dietary substance, it is therefore not a supplement. Nor is it approved as a drug, which puts piracetam in the odd category (along with galantamine) of having no clinical status. As a consequence, there has not been a great deal of research done on piracetam for CFS/ME.
There is, however, a small but significant body of research that seems to indicate that piracetam would be appropriate for the treatment of cognitive impairment in CFS/ME patients. In one such study, researchers in Brazil found that piracetam protected the hippocampus (the part of the brain associated with the formation of new memories) during alcohol withdrawal. It has been widely noted that CFS/ME patients have difficulty forming new memories, which is crucial to learning.
Of even greater interest to CFS/ME patients is a study conducted in 2002 by Gabryel et al, in which piracetam was shown to protect the brain against hypoxic injury. Not only did the drug prevent cell damage, it stimulated mitochondrial function, increasing intracellular ATP. Given the growing body of evidence that people with CFS/ME not only experience lowered oxygenation of brain tissues, but loss of brain matter, this finding could point the way to effective treatment.
PROTOCOL. Dr. Teitelbaum recommends 1200 mg twice a day for 2 weeks, and then 2400 mg twice a day for 2 weeks to treat brain fog. He recommends that piracetam be taken with hydergine, a dopamine-stimulating nootropic. CFS/ME patients may wish to start with the recommended dosage, which is 400-800 mg a day. Those with insomnia and sensitivities to stimulants should begin at an even lower dose – 50 mg.
PROS AND CONS. There are very few reported side effects, but large doses can cause headache, restlessness and insomnia. Patients report good effects at very low doses (50 mg a day). Effects are similar to caffeine – a feeling of alertness, greater focus, and “being awake.”
528
AVAILABILITY AND COST. Piracetam is available online. Amazon.com sells 60-capsule bottle of piracetam (800 mg) for $23.42. This amounts to roughly $1 for 2 grams. If the product works for you, bulk purchase is much less expensive.
FURTHER READING
“Living With Chronic Fatigue Syndrome” blog entry on piracetam. http://livingwithchronicfatiguesyndrome.wordpress.com/2011/04/04/piracetam-for-mecfs/
Patient experiences with piracetam http://forums.phoenixrising.me/archive/index.php/t-9408.html
RESEARCH
Brandão F., M.M. Paula-Barbosa, A. Cadete-Leite. “Piracetam impedes hippocampal neuronal loss during withdrawal after chronic alcohol intake.” Alcohol, Volume 12, Issue 3, May–June 1995, 279–288. http://www.ncbi.nlm.nih.gov/pubmed/7639963 (Abstract)
Dimond SJ, Brouwers EM. "Increase in the power of human memory in normal man through the use of drugs." Psychopharmacology. 1976 49 (3): 307–9. https://www.ncbi.nlm.nih.gov/pubmed/826948 (Abstract)
Gabryel B, Adamek M, Pudełko A, Małecki A, Trzeciak HI. "Piracetam and vinpocetine exert cytoprotective activity and prevent apoptosis of astrocytes in vitro in hypoxia and reoxygenation". Neurotoxicology 2002, 23 (1): 19–31. https://www.ncbi.nlm.nih.gov/pubmed/12164545
Waegemans T, Wilsher CR, Danniau A, Ferris SH, Kurz A, Winblad B. "Clinical efficacy of piracetam in cognitive impairment: a meta-analysis." Dementia and geriatric cognitive disorders. (2002)13 (4): 217–24. https://www.ncbi.nlm.nih.gov/pubmed/12006732 (Abstract)
Winblad, B. "Piracetam: a review of pharmacological properties and clinical uses." CNS Drug Reviews (2005)11 (2): 169–82. www.ncbi.nlm.nih.gov/pubmed/16007238 (Abstract)
ROYAL JELLY
DESCRIPTION. Royal jelly is a thick, milky substance secreted by young nurse honeybees to nourish the young larvae in a colony, especially the queen larvae.
BACKGROUND. Royal jelly is one of nature's most potent foods. It is rich in B vitamins (especially pantothenic acid), biotin, folic acid, and inositol. It also contains vitamins A, C, D, and E, seven minerals, 18 amino acids, fatty acids, enzymes and hormones, and is the only natural source of acetylcholine, the neurotransmitter that aids in memory. Health-enhancing properties attributed to royal jelly range from reducing cholesterol levels to healing skin disorders.
In 2011 a group of researchers found that royal jelly exerted a protective effect on the liver and kidneys of rats which had been given cisplatin, a cytotoxic agent used for chemotherapy. The beneficial effects of royal jelly were attributed to
529
a reduction of oxidative stress and apoptosis (cell death). Oxidative stress and increased cell apoptosis are commonly found in CFS/ME patients. Further research has indicated that royal jelly may be effective in reducing inflammation.
USES IN CFS/ME. Although CFS/ME doctors do not routinely prescribe royal jelly, it has been used by CFS/ME patients for decades. Royal jelly is a natural source of acetylcholine, a neurotransmitter some researchers believe is deficient in CFS/ME, which may be why it is effective in reducing muscle weakness some patients. Its anti-inflammatory properties make it well suited to mitigating pain. Royal jelly also provides an easily tolerated form of B vitamins. Many patients with CFS/ME who need B vitamins cannot tolerate yeast-based vitamin B products.
Steve Wilkinson, author of Chronic Fatigue Syndrome: A Natural Healing Guide, claims that royal jelly can help provide increased stamina and energy, greater mental alertness, and relief from muscle problems. He states that in his case the improvement in muscle pain was "dramatic" after just a few weeks of taking royal jelly.
In a pilot study conducted in England with ME patients, approximately 40 of the participants noted an improvement in energy and stamina. Twelve patients reported a decrease in muscle and joint pain. Another forty noted a decrease in depression. Eighty of the 109 participants said that royal jelly was beneficial.
PROTOCOL. Y&S Eco Bee Farms recommends taking ¼ teaspoon of royal jelly once or twice daily on an empty stomach, followed by a small amount of chilled water. Royal jelly can be taken for months. Some patients need two to three months before its benefits can be felt. Pure royal jelly (not mixed with honey) requires refrigeration because it spoils easily. Royal jelly should not be mixed into or consumed with anything hot.
PROS. Royal jelly is a safe, inexpensive supplement that provides some necessary nutrients, as well as acting as immune modulator. As the only natural source of acetylcholine (ACh), it is one of the safer treatments for the ACh deficiency posited in CFS/ME patients.
CONS. Allergic reactions to royal jelly are not unknown. Patients with a history of pollen allergies should be cautious in using royal jelly. Patients with allergies should be sure the royal jelly has not been mixed with other products (ginseng, bee pollen, honey) to avoid possible allergic reactions to these additives.
AVAILABILITY AND COST. Pure royal jelly is available as a thick liquid or in capsules. Ebeehoney.com sells a 2 oz jar of pure royal jelly for $13. (Shipped with an ice pack.) Because royal jelly loses its potency when improperly handled or processed, it may be worthwhile to buy the purest form available. The refrigerated section of health food stores usually contains the most potent royal jelly products.
FURTHER READING
A pilot study of Irena Royal Jelly conducted on 109 ME patients: http://www.irenesteinrj.com/files/ME%20REPORT.pdf
Suppliers of Y&S pure royal jelly: http://www.yahwehsaliveandwell.com/ysroyaljelly.html
530
Online site for purchasing pure royal jelly: http://www.ebeehoney.com/royaljelly.html
RESEARCH
Harada S, Moriyama T, Tanaka A. [Two cases of royal jelly allergy provoked the symptoms at the time of their first intake]. Arerugi. 2011 Jun;60(6):708-13. http://www.ncbi.nlm.nih.gov/pubmed/21709438 (Abstract)
Karadeniz A, Simsek N, Karakus E, Yildirim S, Kara A, Can I, Kisa F, Emre H, Turkeli M. “Royal jelly modulates oxidative stress and apoptosis in liver and kidneys of rats treated with cisplatin.” Oxid Med Cell Longev. 2011;2011:981793. http://www.ncbi.nlm.nih.gov/pubmed/21904651 (Abstract)
Kohno K, Okamoto I, Sano O, Arai N, Iwaki K, Ikeda M, Kurimoto M. “Royal jelly inhibits the production of proinflammatory cytokines by activated macrophages.” Biosci Biotechnol Biochem. 2004 Jan;68(1):138-45. http://www.ncbi.nlm.nih.gov/pubmed/14745176 (Abstract)
Yanagita M, Kojima Y, Mori K, Yamada S, Murakami S. “Osteoinductive and anti-inflammatory effect of royal jelly on periodontal ligament cells.” Biomedical Research. 2011;32(4):285-91. http://www.ncbi.nlm.nih.gov/pubmed/21878736 (Abstract)
SAMBUCOL
DESCRIPTION. Sambucol is an extract made from the fruit of the European black elder tree (Sambucus nigra L), a member of the Adoxaceae family.
BACKGROUND. Black elderberry berries have long been used in Europe to make jams, jellies, soft drinks, and aromatic wines. In addition to its pleasant taste, elderberry is valued as a rich source of B vitamins and bioflavonoids, as well as minerals such as calcium and phosphorus. Medicinal use of black elderberry has been documented as early as the fifth century BC, when the ancient Greeks described it as a remedy for colds, flu, and upper respiratory tract infections. In the mid-1980s, researchers found that two of the active ingredients in elderberry inhibited the replication of the influenza virus by preventing the virus from entering cells.
In a continuation of that research, in 1992 a group of Israeli scientists and physicians formulated a black elderberry syrup that acted successfully against the influenza virus in a laboratory setting. Soon afterward, a double-blind, placebo-controlled study was conducted in patients with influenza in southern Israel. The results of that study indicated that black elderberry effectively reduced the duration and severity of influenza infections. Flu symptoms (fever, cough, and muscle pain) significantly improved in 20% of the patients within 24 hours, compared with 8% of the control group. Within three days, more than 90% of the patients were symptom free, compared with six or more days for the control group.
In 2011 a group of researchers from the Institute of Medical Biology in Germany found that standardized extract of elderberry inhibited viral replication of influenza A and influenza B. They also found that the extract possessed
531
antimicrobial activity against both gram-positive and gram-negative bacteria in liquid cultures. Another group of researchers in Austria found that a fraction of elderberry produced broad anti-inflammatory effects and supported “the traditional use of extracts and preparations of Sambucus ebulus L., rich in ursolic acid, for the treatment of chronically inflammatory processes.” Results of further studies have also shown that elderberry extract can act against herpes virus and Epstein-Barr virus.
USES IN CFS/ME. The fact that Sambucol has such a wide range of antiviral effects may make it particularly useful for the many patients with CFS/ME who have frequent colds and flu. It may also be valuable for those who demonstrate reactivation of Epstein-Barr virus and other latent viruses, the effects of which can lead to many of the symptoms typical of CFS/ME. Many CFS/ME patients taking Sambucol have noted overall improvement (Mass CFS/ME Update, Fall 1995).
PROTOCOL. The recommended dosage of Sambucol syrup is 4 tablespoons daily in adults and 1 tablespoon daily in children younger than 12 years. Patients with CFS/ME should probably start with a smaller dose to check for tolerance. Sambucol should be taken on a full stomach. Dairy products should be avoided for 30 minutes before and after to avoid stomach upset. The manufacturers recommend refrigeration after opening.
PROS. Sambucol is an all-natural product, which is an advantage for patients with chemical and drug sensitivities. There are no reported side effects or contraindications associated with its use. Those who have tried it claim that it hastens recovery from flu and colds, and lessens general malaise. Sambucol is also safe for children, which is good news for parents of children with CFS/ME, because so few effective pediatric medications are currently available.
CONS. Some patients report allergy-type reactions (congestion, headache, dizziness) to elderberry. As fresh elderberry leaves and bark are poisonous (but not the berries), always purchase processed elderberry extracts with high flavonoid content from a reputable company. Do not make your own tea.
AVAILABILITY AND COST. Sambucol is currently marketed in the United States, Europe, Israel, and South Africa through health food stores and drugstores. The liquid extract contains glucose and honey for sweetening and raspberry extract to enhance flavor. If a glucose-free product is desired, Sambucol is available in lozenge form and as a liquid sweetened with sorbitol. Vitacost sells 4 oz bottle of liquid Sambucol for between $10 and $15. Lozenges in packs of thirty cost about $7. Prices at retail outlets are generally considerably higher.
FURTHER READING
Complete information about the composition, effects and clinical research of elderberry extract. http://www.drugs.com/npp/elderberry.html
RESEARCH
Konlee, M. “A new triple combination therapy.” Posit Health News. 1998 Fall;(No 17):12-4. http://www.ncbi.nlm.nih.gov/pubmed/11366542 (Abstract)
532
Krawitz C, Mraheil MA, Stein M, Imirzalioglu C, Domann E, Plechka S, Hain T. “Inhibitory activity of a standardized elderberry liquid extract against clinically-relevant human respiratory bacterial pathogens and influenza A and B viruses.” BMC Complement Altern Med. 2011 Feb 25; 11:16. http://www.ncbi.nlm.nih.gov/pubmed/21352539 (Abstract)
Schwaiger S, Zeller I, Pölzelbauer P, Frotschnig S, Laufer G, Messner B, Pieri V, Stuppner H, Bernhard D. “Identification and pharmacological characterization of the anti-inflammatory principal of the leaves of dwarf elder (Sambucus ebulus L.).” J Ethnopharmacol. 2011 Jan 27;133(2):704-9. http://www.ncbi.nlm.nih.gov/pubmed/21040770 (Abstract)
Zakay-Rones Z, E Thom, T Wollan, and L Wadstein. “Randomized Study of the Efficacy of and Safety of Oral Elderberry Extract in the Treatment of Influenza A and B Virus Infections.” The Journal of International Medical Research. 2004; 32: 132-140. http://www.jimronline.net/content/full/2004/47/0445.pdf
SAMe
DESCRIPTION. SAMe (S-Adenosyl methionine), is a primary methyl group donor that is involved in the synthesis of neurotransmitters.
BACKGROUND. SAMe (pronounced “Sammy”) was first discovered in Italy in 1952. It is a cornerstone in the methylation cycle, which is the biochemical process through which amino acids are transformed into neurotransmitters. (SAMe's contribution of its methyl group (CH2) is what converts an amino acid into a neurotransmitter.) It should not come as a surprise that SAMe plays a key role in mood, nervous system regulation, and maintaining energy levels, since all of these are regulated by neurotransmitters.
The first studies of SAMe's use in depression were conducted in Italy in the 1970s. Because SAMe is a primary methyl group donor, the authors concluded that depression could be linked to the methylation cycle. Since that time, there have been dozens of studies confirming the efficacy of SAMe in treating depression.
USES IN CFS/ME: Rich Van Konynenburg has proposed that in CFS/ME there is a partial block of the methylation cycle. This would cause a depletion of ATP, as well as reductions in neurotransmitters, detoxing agents such as glutathione, and impairment of normal immune system function. Because SAMe is a vital component of the methylation cycle, Dr. Myhill recommends it as an all-round support.
PROTOCOL. SAMe should be taken on an empty stomach. Low doses, ranging from 50 to 100 mg/day are recommended. (Ray Sahelian advises taking half of a tablet, and storing the rest for the next day.) Because SAMe can produce insomnia, it is best taken in the morning. SAMe is highly unstable, and should be stored in a cool, dry place to prevent deterioration. SAMe should be taken with vitamin B6, B12 and folic acid as adjuncts.
PROS AND CONS. SAMe appears to have few side effects. But as with any product that affects the central nervous system (even indirectly), care should be exercised. While most people feel an immediate improvement in mood and focus,
533
some sensitive individuals can experience side effects typical of stimulants (jitters, insomnia, headache, anxiety). SAMe raises levels of all neurotransmitters, so it is difficult to predict how any individual person may respond.
AVAILABILITY AND COST. SAMe is available in health food stores and from online suppliers. A package of 20 foil-wrapped enteric-coated tablets (200 mg) costs $10 through Vitacost.
SEE: Van Konynenburg/Yasko Methylation Protocol
FURTHER READING
Ray Sahelian on SAMe: http://www.raysahelian.com/sam-e.html
Dr. Myhill discusses the methylation cycle: http://drmyhill.co.uk/wiki/CFS_-_The_Methylation_Cycle
RESEARCH
Kagan BL, Sultzer DL, Rosenlicht N, Gerner RH. “Oral S-adenosylmethionine in depression: a randomized, double-blind, placebo-controlled trial.” Am J Psychiatry. 1990 May;147(5):591-5. http://www.ncbi.nlm.nih.gov/pubmed/2183633 (Abstract)
Mischoulon, David and Maurizio Fava. “Role of S-adenosyl-L-methionine in the treatment of depression: a review of the evidence.” Am J Clin Nutr. 2002;76(suppl):1158S–61S. http://www.ajcn.org/content/76/5/1158S.full.pdf
VITAMINS
Vitamin A, Beta-Carotene, Vitamin B12, Vitamin B6, Vitamin B Complex, Vitamin C, Vitamin D, Vitamin E and Tocotrienols
DESCRIPTION. Vitamins are organic (carbon-containing) substances needed in tiny amounts to promote biochemical reactions within living cells.
BACKGROUND. Vitamins, as independent biochemical agents, were discovered around the turn of the century when an English biochemist proposed that diseases such as rickets and scurvy were most likely caused by a lack of "accessory food factors" in the diet. After observing that these diseases could be corrected by adding certain foods (whole rice, which is high in vitamin B, to cure rickets; and oranges, an easy source of vitamin C, to cure scurvy), scientists began to search for chemical compounds in these foods that could produce such extensive changes in the body. When these accessory food factors were finally isolated in food, the name "vita-mine" was proposed (from the Latin vita, necessary for life, and amine, a chemical substance containing nitrogen). Later, when it was discovered that not all vitamins were amines, the final "e" was dropped.
There are thirteen known vitamins, all of which act as catalysts, or more specifically, coenzymes; that is, they initiate or speed chemical reactions in cells while remaining unchanged themselves. They accomplish their task mainly by
534
combining with a protein-containing apoenzyme (vitamins contain no protein) to form a complete enzyme. The completed enzyme performs the role of biochemical catalyst, enabling most of the body's vital cell functions to occur in an orderly and efficient manner. Without vitamins, many essential cell functions would cease, resulting in any number of vitamin deficiency-related diseases and problems. Most vitamins must be obtained from food because the body rarely manufactures them in adequate amounts (vitamin K is the exception).
USES IN CFS/ME. Most CFS/ME physicians and clinicians include vitamin supplementation as a part of a general treatment protocol. The reasons vitamin supplementation is considered such a central part of CFS/ME treatment are threefold. First, the ill body consumes vitamins much faster than the healthy body. Patients, particularly those with long-term illnesses, need vitamins in amounts that exceed those which can be derived from food, especially when (as in CFS/ME) the illness causes certain metabolic defects.
Second, at least 50% of patients with CFS/ME have absorption problems (leaky gut, low stomach acid production, or other gastrointestinal difficulties). When food is improperly digested, vitamins are not extracted efficiently, necessitating some kind of supplementation.
Third, as has been pointed out by a number of researchers, the particular nature of CFS/ME immune system activation prevents some vitamins from working properly. The excess cytokine production that blocks vitamin C function, for example, is justification enough for supplementation.
The most frequently recommended vitamin supplements are vitamin C and B12, but general wide-spectrum supplements are also important. Benefits of vitamin supplementation generally are not apparent for several weeks, but some undernourished patients notice significant effects within a few hours. Many CFS/ME patients report an overall improvement in vitality, energy level, and stamina with vitamin supplementation. Few report any adverse effects (and these are usually remedied by switching brands).
AVAILABILITY AND COST. Vitamins are easily obtained from supermarkets, health food stores, pharmacies, and online suppliers. Vitacost markets a good multi-vitamin/mineral supplement made by Carlson for $8.50 (90 gelcaps).
Care should be taken to purchase high-grade vitamins because the excessive heat and poor handling to which low-grade vitamin products are exposed often cause fat-soluble vitamins to become rancid and can considerably reduce the efficacy of water-soluble vitamins. Excess filler also makes some cheaper vitamins difficult to dissolve. (A good test for vitamin tablets is to place one in a small glass of lemon juice. If it doesn't dissolve in the lemon juice, it won't dissolve in your stomach.) With the exception of vitamin E, synthetic vitamin preparations are as effective as natural vitamins.
In addition to a wide-spectrum vitamin supplement, many CFS/ME physicians recommend taking extra amounts of specific vitamins for the purposes of
535
providing added antioxidant protection, for immune system enhancement, or to compensate for the functional deficits common to the illness.
FURTHER READING
General information about vitamins (and other) supplements for CFS/ME patients. http://www.cfids.org/archives/2004/2004-1-article04.asp
VITAMIN A
DESCRIPTION. Vitamin A (retinol) plays a variety of roles in human metabolism. It helps maintain the health of the skin and all mucous linings of the body (stomach, intestines, bladder, mouth, nose, throat, windpipe, and other air passages). It is essential for vision. Vitamin A also increases resistance to infections and is involved in the maintenance of the adrenal cortex, where cortisol is formed.
USES IN CFS/ME. Vitamin A is primarily used to help maintain mucous membranes, which are often compromised in CFS/ME. Patients prone to intestinal, respiratory, or ear infections also take vitamin A to boost immune system efficiency. There have been attempts in the past to redefine vitamin A as an "anti-infective agent." However, because its protective capacity is limited to bacterial infections of the mucous membranes, these have been abandoned.
The recommended daily allowance for vitamin A is 5000 IU a day. Because vitamin A is fat soluble, it can be stored in the liver, which means it can be taken less frequently in larger doses. A physician or nutritionist should be consulted before taking larger doses, however, to prevent possible overdosing. Loss of appetite, irritability, widespread itching, headaches, and mouth ulcers are all signs of vitamin A toxicity. People with low thyroid function must take vitamin A supplements, as the thyroid is responsible for converting beta-carotene into vitamin A.
AVAILABILITY AND COST. Vitamin A is available from health food stores, many pharmacies, and some supermarkets. The form of vitamin A most easily absorbed is micellized A, a liquid suspension sold in health food stores. The best natural sources of vitamin A are animal products (liver, whole milk, butter, and cheese). Fish liver contains huge amounts of vitamin A (200,000 to 1 million IU, depending on the type). Pregnant women should not take more than 5000 IU of vitamin A, because higher doses have been associated with birth defects.
BETA-CAROTINE
DESCRIPTION. Beta-carotene is the precursor to vitamin A. When foods containing beta-carotene (yellow or orange vegetables) are ingested, the liver converts the beta-carotene to vitamin A. However, unlike vitamin A it cannot be stored in the body and therefore entails far fewer risks of toxicity, although its function remains largely the same. Like vitamin A, beta-carotene strengthens mucous membranes. It also helps protect against skin and lung cancer and improves the functioning of the thymus gland (where T cells are produced). There is no recommended daily allowance for beta-carotene, but people who take large
536
amounts often notice that certain areas of their skin, particularly the palms and around the fingernails, turn yellowish orange. This condition is called carotenemia and, while benign, is a sign that too much beta-carotene is being consumed. Patients with diabetes or hypothyroid conditions should avoid taking beta-carotene because they cannot convert it to vitamin A.
USES IN CFS/ME. Beta-carotene is one of the vitamins mentioned by clinicians as having particular value in CFS/ME. Dr. Burke Cunha proposed that one of the chief benefits of beta-carotene for CFS/ME patients lies in its ability to stimulate the production of natural killer cells (CFIDS Chronicle, Fall 1993). He found that among the majority of his patients who tested low in natural killer cells, high doses of beta-carotene resulted in an increase in the number of these cells. He also found less fatigue in these patients. (Patients with normal numbers of natural killer cells before therapy showed less improvement, however.)
Dr. Cunha postulated that by increasing natural killer cell production, beta-carotene may serve as an effective antiviral agent. He recommended a high dose (25,000 to 50,000 IU/day, depending on the patient's needs), but cautioned that high doses of beta-carotene should not be taken for more than three weeks to prevent carotenemia and vitamin A toxicity. Most clinicians recommend a daily dose of 5000 to 10,000 IU in combination with other antioxidants to prevent carotenemia.
FURTHER READING
Dr. Cunha on beta-carotene supplementation for CFS/ME patients. http://www.immunesupport.com/94wtr007.htm
CFS/ME patient ratings of beta-carotene: http://www.revolutionhealth.com/drugs-treatments/rating/beta-carotene-for-chronic-fatigue-syndrome-cfs-cfids-me
VITAMIN B12
DESCRIPTION. Vitamin B12 (cobalamin) is a member of the B vitamin complex. It is naturally found in animal products and is required for proper digestion, food absorption, protein synthesis, metabolism of carbohydrates and fats, myelin synthesis, nerve function, and activation of folic acid (used in the formation of red blood cells). Its name is derived from cobalt, the mineral to which this vitamin is bound. When cobalamin is ingested, contact with stomach enzymes splits it apart, freeing it to join with a special protein called "intrinsic factor," which is secreted by the stomach lining. Only when vitamin B12 combines with intrinsic factor – which converts the cobalamin into methylcobalamin – can it be absorbed by the body. Because vitamin B12 is highly unstable outside the body, cyanocobalamin, a synthetic form of B12, is normally used in supplements. Oral vitamin B12 cannot be absorbed in malabsorptive states such as pernicious anemia.
USES IN CFS/ME. Although the traditional use for vitamin B12 injections has been limited to the treatment of anemia, Dr. Charles Lapp and Dr. Paul Cheney have observed that such injections are highly beneficial to their CFS/ME patients, even in the absence of vitamin B12 deficiency or any sign of anemia. They report
537
that some 50% to 80% of their patients demonstrate improved stamina and energy with vitamin B12 therapy (CFIDS Chronicle, Fall 1993).
Dr. Cheney was first motivated to include vitamin B12 in his general treatment plan after seeing evidence that vitamin B12 injections had been helpful in a number of nonanemic neuropsychiatric patients. These patients had demonstrated some of the symptoms common to CFS/ME (paresthesia, sensory loss, loss of coordination, and mood swings), all of which improved with vitamin B12 injections. Dr. Cheney theorized that vitamin B12 injections work so well among CFS/ME patients because the elevated rate of cytokine production in CFS/ME may be effectively blocking vitamin B12 function in the body. In this case, massive amounts of vitamin B12 would be needed to overcome the functional deficiency brought about by excess cytokine production.
Vitamin B12 may also help correct the red blood cell abnormalities in CFS/ME patients discovered by New Zealand researcher Dr. Leslie O. Simpson (CFIDS Chronicle, Fall 1995). Dr. Simpson observed that hydroxocobalamin injections corrected this defect by increasing production of disc-shaped cells. About 50% of the patients in this group felt better with B12 injections.
Dr. Myhill, in her explanation of the benefits of B12 in CFS/ME patients, observes that B12 is a powerful free radical scavenger, particularly of nitric oxide. (People with CFS/ME have high levels of nitric oxide.) In addition to mitigating the harmful effects of nitric oxide, B12 also helps correct one of the immune system abnormalities found in CFS/ME patients. According to Dr. Cheney, CFS/ME patients experience a shift from Th1 (cellular) to Th2 (humoral) immunity. In essence, the immune system is skewed in favor of B cells (which search for pathogens in the bloodstream) rather than searching for pathogens within cells. This imbalance allows for the proliferation of viruses within cells. According to Dr. Bell, vitamin B12 is one of the most effective means of re-orienting the immune system back to Th1 (cellular) immunity.
PROTOCOL. The dosage Dr. Cheney recommends is 2000 to 5000 ug/ml (in a 0.5 to 1.0 cc syringe) administered subcutaneously or intramuscularly every two or three days. Other physicians generally recommend 1000 to 2000 ug (1 to 2 cc syringe) one to three times a week. Dr. Myhill starts with ½ mg (500 mcgms) daily by subcutaneous injection. Dr. Lapp says that to obtain a “continuous and satisfactory level of improvement,” 3000 mcg of cyanocobalamin every two to three days should be administered.
High doses of vitamin B12 must be accompanied by a multivitamin that includes the entire vitamin B complex to avoid B vitamin imbalances. This dosage can be tolerated over long periods, although benefits can wane. In that case, a short period without vitamin B12 injections (1 to 2 weeks) is usually enough to reestablish its efficacy. Most physicians prefer cyanocobalamin to hydroxocobalamin because it is the most stable form of vitamin B12. However, some patients who cannot tolerate cyanocobalamin prefer the more bioavailable, and longer acting, hydroxocobalamin.
538
PROS. Most patients who take vitamin B12 injections report favorable results. Common benefits include increased energy, mental clarity, and stamina, usually lasting for several days after a single administration. Because benefits may not be felt for the first three to six weeks, a month's trial is generally recommended.
CONS. Although vitamin B12 is fairly innocuous, some patients report side effects. The most common side effect is lassitude. Some patients also report local rashes, which diminish when dosage is reduced, and various allergic reactions (including diarrhea) to the preservatives used in the solution. To avoid potential allergic reactions, a patch test should be performed first. Administration of the first injection in a physician's office is also recommended in highly allergic individuals.
AVAILABILITY AND COST. The most effective form of B12 is injectable vitamin B12, available by prescription. After injections, the most easily absorbed form of B12 is via nasal spray, also available by prescription. For those who do not have a doctor willing to prescribe B12, there are both sublingual and oral spray forms that are fairly well absorbed. (Don't waste your money on oral tablets and capsules. They are very poorly absorbed.) Perque markets activated sublingual hydroxocobalamin (2000 mcg) for about $30 (100 lozenges). (Take one a day.) PureFormulas.com markets B12 spray (with B6 and folic acid) made by NOW for $12.59.
FURTHER READING
Dr. Lapp's B12 recommendations: http://www.cfids.org/archives/1999/1999-6-article03.asp
Dr. Myhill's excellent explanation of why B12 works in CFS/ME patients. http://www.drmyhill.co.uk/wiki/B12_-_rationale_for_using_vitamin_B12_in_CFS
B12 Basics – very detailed: http://forums.phoenixrising.me/showthread.php?11522-Active-B12-Protocol-Basics/
Informative patient thread on the uses of B12 for treating CFS/ME. http://www.prohealth.com/fibromyalgia/blog/boardDetail.cfm?id=1318273
RESEARCH
van Asselt, D Z B, F W H M Merkus, F G M Russel, and W H L Hoefnagels. “Nasal absorption of hydroxocobalamin in healthy elderly adults.” Br J Clin Pharmacol. 1998 January; 45(1): 83–86. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1873990/
VITAMIN B6
DESCRIPTION. Vitamin B6 (pyridoxine, pyridoxal, and pyridoxamine), is one of nature's busiest vitamins. It is involved in more than one hundred essential chemical reactions in the body, including making amino acids and neurotransmitters, metabolizing energy, balancing hormones, and supporting the immune system. High doses of B6 have been shown to decrease colorectal cancer rates. Vitamin B6 is also used to prevent heart disease by lowering cholesterol, to
539
treat the nausea and vomiting associated with morning sickness, and, because of its importance in nervous system function, to treat various CNS conditions, including depression, schizophrenia and ADD.
USES IN CFS/ME. A study published in 1999 by a group of British researchers found that CFS/ME patients had reduced functional status of B vitamins, particularly B6. Because B6 is vital to so many neuroendocrine reactions, a deficiency can result in impaired sleep (due to B6's role in converting glutamate to GABA), hypoglycemia (due to the role of B6 in neoglucogenesis), and neuropathy (damage to the peripheral nervous system). A classic sign of vitamin B6 deficiency is skin eruptions resembling seborrheic dermatitis, a common symptom in acute stages of CFS/ME. CFS/ME patients have found that B6 is useful for treating pain, especially carpal tunnel syndrome.
PROTOCOL. As high doses can cause imbalances in other B vitamins, a low dose is recommended. The minimum requirement is 1.5 mg. (The maximum dose is 100 mg.) The active, and therefore most effective, form of B6 is pyridoxal phosphate (also known as P5P). P5P is well tolerated and is easily absorbed in oral form. High doses of B6 (200 mg) can cause symptoms of nerve damage (loss of feeling in the legs, loss of balance). These effects are reversible once the dosage is lowered. Supplementation with zinc is advised if there is a deficiency of either B6 or zinc, as B6 cannot be utilized without zinc.
FURTHER READING
The University of Maryland's informative page on vitamin B6. http://www.umm.edu/altmed/articles/vitamin-b6-000337.htm
RESEARCH
Heap LC, Peters TJ, Wessely S. “Vitamin B status in patients with chronic fatigue syndrome.” J R Soc Med. 1999 Apr;92(4):183-5. http://www.ncbi.nlm.nih.gov/pubmed/10450194 (Abstract)
VITAMIN B COMPLEX
DESCRIPTION. Many patients with CFS/ME benefit from taking a vitamin B complex formulation, either in accompaniment to single B vitamins (to prevent imbalances) or alone. CFS/ME patients have reported improvement in energy levels, symptoms of premenstrual syndrome (PMS), mood, and sleep disorders after taking vitamin B complex. Most vitamin B complex formulations include vitamins B1 (thiamine), B2 (riboflavin), B3 (niacin), B5 (pantothenic acid), B6 (pyridoxine, pyridoxal, and pyridoxamine), B7 (biotin), B9 (folic acid), and B12 (cobalamin). People with allergies, Candida infection, or digestive symptoms should avoid yeast-based formulations, which may be poorly tolerated.
AVAILABILITY AND COST. Nature's Life and Source Naturals both sell a 100-capsule yeast-free bottle of B complex for about $7 (available online). Vitacost sells its in-house brand of yeast-free liquid vitamin B complex for $15 (will last three months).
540
VITAMIN C
DESCRIPTION. Vitamin C (ascorbic acid) is a water-soluble antioxidant found in most raw fruits and vegetables. It serves a number of vital functions in the body, including connective tissue repair (especially collagen), maintaining healthy teeth and bones, promoting the synthesis of anti-inflammatory hormones in the adrenal glands, helping to produce the neurotransmitters serotonin and norepinephrine, healing wounds, maintaining capillaries, healthy adrenal glands, and ovaries, absorbing iron into the bloodstream, promoting efficient white blood cells, and maintaining cholesterol balance. It is widely touted as a preventive for the common cold, perhaps because vitamin C increases the production of interferon, an antiviral cytokine.
Animal experiments have shown that vitamin C has other immune system-enhancing effects as well, increasing the body's ability to fight off bacterial infections and promoting general immunity. Patients with allergies may want to take special note of vitamin C's function as a natural antihistamine. A research team led by the co-discoverer of vitamin C, Professor Charles Glen King of Columbia University, demonstrated as early as 1940 that it can both prevent and moderate allergy symptoms. In addition to its other beneficial properties, vitamin C is also a natural chelator, helping to remove heavy metals and toxins from the body.
Vitamin C is not stored in the body, as are fat-soluble vitamins, and thus must be constantly replenished. Smoking, drinking (alcohol), illness, and physical or emotional stress all cause rapid depletion of vitamin C.
USES IN CFS/ME. Vitamin C is the most widely used of all vitamins for CFS/ME patients, not just because of its role as an antioxidant and free radical scavenger, but also because of the numerous other vital functions it performs. Of particular relevance to patients with CFS/ME is the role of vitamin C in maintaining healthy capillaries. A number of researchers have remarked on the poor circulation in patients with CFS/ME, resulting in corollary illnesses such as Reynaud's phenomenon. Even more critical in CFS/ME is reduced blood flow to the brain, which is especially dependent on capillary action for its blood supply. This function alone helps to place vitamin C at the forefront of any vitamin therapy. However, its role in collagen formation and tissue repair, its importance in immune system function, and its place as an adrenal gland support do much to explain why it is one of the most frequently recommended CFS/ME nutritional treatments.
PROTOCOL. Most nutritionists recommend taking vitamin C to tolerance; that is, until the patient begins experiencing diarrhea or burning urine. Considering the broad spectrum of sensitivities among CFS/ME patients, tolerance can vary considerably. CFS/ME clinicians generally recommend anywhere from 2000 – 6000 mg/day (taken in small divided doses) up to tolerance.
Dr. Martin Pall recommends doses on the order of 500 to 1000 mg/day, taken several times per day. Vitamin C can act to regenerate tetrahydrobiopterin (BH4) and, therefore, may act to lower oxidative stress. High doses of vitamin C can be
541
useful in scavenging peroxynitrite (ONOO‾), the most central element in his NO/ONOO‾ cycle hypothesis.
For those who are intolerant to vitamin C, it is worthwhile to administer it topically. It is very easy to make an ointment. Put a small amount of hand lotion into a small bowl (only as much as you intend to use). Add 1/8 teaspoon of pure ascorbic acid powder (about 500 mgs) to the lotion. Mix with your finger and apply immediately to the skin. The mixture cannot be stored, so be sure not to make too much. About 10% of the vitamin C you use can be absorbed via this method. (Over a period of time, the mixture will yellow your nails. This is because the vitamin C turns yellow when exposed to moisture. The effect goes away when you stop topical applications.)
PROS AND CONS. Vitamin C is inexpensive, easy to take and usually well-tolerated. Patients report that on low doses (500 – 1000 mg), they catch fewer colds. Some CFS/ME patients are quite sensitive to vitamin C and can only tolerate small amounts.
AVAILABILITY AND COST. Vitamin C is one of the least expensive vitamins and is widely available at most pharmacies, health food stores, online suppliers, and supermarkets. Unfortunately, vitamin C is quite unstable. It degrades quickly when exposed to light and heat, and has a short shelf life, which means most commercial tablets and pills contain very little usable vitamin C. In addition, Vitamin C degrades when exposed to moisture, which means drinks with added vitamin C share the same drawbacks as tablets.
The best form of Vitamin C is pure vitamin C powder (ascorbic acid). Because it is a powder, it can be titrated (taken in very small doses). Ascorbic acid is very sour, so most people prefer mixing it with a bit of juice. Allergy Research sells a 120-gm bottle of pure ascorbic acid powder for roughly $10 through Vitacost. At ½ teaspoon a day (2000 mg) a bottle will last two months.
For those with gastrointestinal symptoms, acid-free C powder may be more tolerable. Ascorbic acid can be buffered with magnesium carbonate, calcium carbonate and/or potassium carbonate to reduce acidity. Oral buffered vitamin C in small doses is extremely safe, with virtually no side effects.
Intravenous (IV) drip is another form of vitamin C therapy used in CFS/ME. Administering vitamin C directly into the bloodstream not only increases the rate at which it is absorbed but enhances its role as a chelating agent. A number of health care practitioners use vitamin C as an essential component of CFS/ME therapy.
Intravenous drip therapy should not be administered daily and requires monitoring by a physician. The charge for an intravenous drip is $70 to $125, depending on locale. Insurance usually does not cover the cost.
FURTHER READING
Good overview of vitamin C supplements. http://www.electroherbalism.com/Naturopathy/Therapies/Supplements/Vitamins/VitaminC/index.htm
542
Detailed overview of the Krebs cycle and its role in CFS/ME. http://www.nutritionreview.org/library/krebs.php
CFS/ME patient ratings of vitamin C: http://www.revolutionhealth.com/drugs-treatments/rating/vitamin-c-ascorbic-acid-for-chronic-fatigue-syndrome-cfs-cfids-me
VITAMIN D
DESCRIPTION. Vitamin D is a unique vitamin in that the body can synthesize it when exposed to sunlight. There are two forms of vitamin D, ergocalciferol (D2) and cholecalciferol (D3). The difference between the two forms is that D2 is derived from ergosterol (a chemical compound produced by phytoplankton, invertebrates, and fungi) while D3 is produced by ultraviolet light irradiation.
Vitamin D has come under increasing scrutiny over the past few years due to its functions in bone maintenance and immune system function. Physicians have known for decades that cod liver oil is an effective treatment for rickets, a childhood condition in which bones and teeth become soft. Ultimately, it was discovered that rickets was caused by a deficiency of vitamin D. As a consequence, vitamin D is added (actually, produced via exposure to ultraviolet light) to all milk. Aside from rickets, deficiencies in vitamin D have been linked to gingivitis, inflammatory bowel disease, depression, fatigue, and heart disease. Vitamin D is also recommended for women at risk for osteoporosis.
Vitamin D's role in the immune system is no less important. One of its most important functions is to activate T cells, in particular the T cells that identify and attack invading pathogens. Without vitamin D, T cells remain dormant or “naive.”
USES IN CFS/ME. In a 2009 study, Berkovitz et al found that vitamin D levels were moderately to severely low in CFS/ME patients as compared to the general population. The researchers recommended vitamin D supplementation. More recently, in 2011 a group of pediatric researchers at the Mayo Clinic discovered that adolescents with CFS/ME and orthostatic intolerance (OI) had low levels of both ferritin (a protein that stores and releases iron) and vitamin D.
The question for some researchers is whether low vitamin D levels are a cause of the illness or a result of it. CFS/ME is characterized by a shift from Th1 (cellular) to Th2 (humoral) immunity. Basically, the immune system in a person with CFS/ME spends too much effort identifying and attacking foreign invaders (Th2) and too little effort focusing on pathogens within cells (Th1). This allows for a proliferation of viruses that multiply within cells. The argument is that Vitamin D, because it is crucial for the production of macrophages (the immune system components that “eat” extracellular pathogens), may become depleted as a result of the shift to Th2.
PROTOCOL. In the presence of low serum D levels, dosage is determined by the physician. For those who wish to supplement, and who are getting adequate sun exposure, low doses are advised (1000 – 2000 IU).
543
AVAILABILITY AND COST. Vitamin D is inexpensive and widely available at any health food store, supermarket, drug store and from online distributors. It is a fat-soluble vitamin, so gelcaps or drops are more easily assimilated. But, for those who are sensitive to gelcaps, there are dry forms of vitamin D as well. (Although some form of oil or fat must be in the intestines for proper absorption.) If you are already taking fish oil, supplementation with vitamin D may not be necessary.
TESTING: There are two tests for determining blood levels of vitamin D. The most commonly used test is for 1,25 (OH)2 vitamin D (1,25 dihydroxy vitamin D). This test measures a form of vitamin D that has a long half life (about three weeks) and therefore will only give your doctor an overall picture of your votamin . A more specific test, 25OH vitamin D (25-hydroxy vitamin D ), will tell your doctor how much vitamin D is currently in your bloodstream. Of the two tests, the second is more useful for determining actual vitamin D levels.
FURTHER READING
List of articles concerning vitamin D deficiency: http://www.vitamindcouncil.org/about-vitamin-d/vitamin-d-deficiency/
CFS/ME patient reviews of vitamin D: http://www.revolutionhealth.com/drugs-treatments/rating/vitamin-d-for-chronic-fatigue-syndrome-cfs-cfids-me
RESEARCH
Antiel RM, Caudill JS, Burkhardt BE, Brands CK, Fischer PR. “Iron insufficiency and hypovitaminosis D in adolescents with chronic fatigue and orthostatic intolerance.” South Med J. 2011 Aug;104(8):609-11. http://www.ncbi.nlm.nih.gov/pubmed/21886073 (Abstract)
Berkovitz S, Ambler G, Jenkins M, Thurgood S. “Serum 25-hydroxy vitamin D levels in chronic fatigue syndrome: a retrospective survey.” Int J Vitam Nutr Res. 2009 Jul;79(4):250-4. http://www.ncbi.nlm.nih.gov/pubmed/20209476 (Abstract)
VITAMIN E
DESCRIPTION. Vitamin E (tocopherol) is a fat-soluble vitamin found in butterfat, meats, vegetable oils, and particularly wheat germ oil, from which this vitamin was first isolated in 1936. It is made up of four tocopherols (alpha, beta, gamma, delta) and four tocotrienols (alpha, beta, gamma, delta). Like other antioxidants, vitamin E serves to protect cell linings from damage caused by oxidation. It helps to maintain red blood cell membranes and other cell tissues (even the walls of the tiny structures within cells), ensures normal muscle metabolism, and protects essential unsaturated fatty acids and vitamin A from destruction from oxidation. Vitamin E has protective activity against methyl mercury toxicity and increases the activity of glutathione. Zinc is needed to maintain proper levels of vitamin E in the blood; thus, zinc deficiency can lead to low vitamin E levels.
USES IN CFS/ME. In a 2003 study conducted in Italy, researchers found that CFS/ME patients exhibited significantly lower antioxidants (vitamin E among others) in serum samples as compared to controls. The CFS/ME group also had lower pain thresholds than controls in all muscle sites tested. The researchers
544
correlated levels of vitamin E concentration to the degree of muscle pain — the lower the vitamin E levels, the greater the pain. While the researchers did not offer treatment suggestions, their findings indicate that supplementation would be beneficial.
In 2009 Miwa and Fujita also found low serum levels of vitamin E in CFS/ME patients. They concluded that the reduction in vitamin E was due to oxidative stress. In a later study, Miwa and Fujita found that low serum levels of vitamin E in CFS/ME patients correlated with flares. They concluded that the “low level of serum alpha-tocopherol was ameliorated during the remission phase as compared with the exacerbation phase in the patients with chronic fatigue syndrome, suggesting that increased oxidative stress may be involved in the pathogenesis of chronic fatigue syndrome and might also be directly related to the severity of the symptoms of chronic fatigue syndrome.” This conclusion is very much in line with research demonstrating oxidative stress in people with CFS/ME, and leads to a specific course of supplementation. Vitamin E reduces oxidative stress by mitigating the effects of lipid peroxidation. Vitamin E can also reduce chronic inflammation by down-regulating the NF-kappaB inflammatory pathway.
In keeping with these findings, and numerous other studies linking oxidative stress to CFS/ME symptoms, vitamin E is used chiefly for its properties as an antioxidant. Its ability to strengthen cell walls and protect other vitamins and fats from destruction makes it highly desirable as an adjunct to other vitamin therapies.
PROTOCOL. Because it is fat-soluble, only minimal amounts are needed to produce antioxidant benefits. The optimal dosage, 200 IU of natural vitamin E (mixed tocopherols), taken daily with the largest meal is usually recommended for patients with CFS/ME. Vitamin E acts as a blood thinner, so do not take it with other blood thinners, or before surgery.
Recently, research has been focused on tocotrienols, which are closely related to the tocopherols. Tocotrienols, like tocopherols, are found in some vegetable oils, wheat germ, barley, saw palmetto, and certain varieties of nuts and grains. The reason for the high interest generated by tocotrienols is that they have been shown to protect against brain cell damage and cardiovascular disease, prevent cancer, reduce cholesterol and combat oxidative stress to the skin produced by UV exposure. Dr. Pall has pointed out that tocotrienols can penetrate tissues with saturated fatty layers more efficiently than tocopherols, making tocotrienols, particularly delta tocotrienols, powerful antioxidants.
AVAILABILITY AND COST. Vitamin E is available at any drug store, health food store, and from online suppliers. Look for a good brand of natural Vitamin E. Vitacost sells natural vitamin E for between $8 and $17 a bottle. Delta tocotrienols are available in health food stores and online through PureFormulas.com and Vitacost for roughly $13 to $25 a bottle.
FURTHER READING
CFS/ME patient reviews of vitamin E: http://www.revolutionhealth.com/drugs-treatments/rating/vitamin-e-for-chronic-fatigue-syndrome-cfs-cfids-me
545
RESEARCH
Kim S, Lee EH, Kim SH, Lee S, Lim SJ. “Comparison of Three Tocopherol Analogs as an Inhibitor of Production of Proinflammatory Mediators in Macrophages.” J Pharmacol Sci. 2012 Feb 3. http://www.ncbi.nlm.nih.gov/pubmed/22302019 (Abstract)
Miwa K, Fujita M. “Increased oxidative stress suggested by low serum vitamin E concentrations in patients with chronic fatigue syndrome.” Int J Cardiol. 2009 Aug 14;136(2):238-9. http://www.ncbi.nlm.nih.gov/pubmed/18684522 (Abstract)
Miwa K, Fujita M. “Fluctuation of serum vitamin E (alpha-tocopherol) concentrations during exacerbation and remission phases in patients with chronic fatigue syndrome.” Heart Vessels. 2010 Jul;25(4):319-23. http://www.ncbi.nlm.nih.gov/pubmed/20676841 (Abstract)
Rezk BM, Haenen GR, Van Der Vijgh WJ, Bast A. “The extraordinary antioxidant activity of vitamin E phosphate.” Biochim Biophys Acta. 2004 Jul 5;1683(1-3):16-21. http://www.ncbi.nlm.nih.gov/pubmed/15238215 (Abstract)
Vecchiet, Jacopo, Francesco Cipollone, Katia Falasca , Andrea Mezzetti, Eligio Pizzigallo, Tonino Bucciarelli, Silvana De Laurentis, Giannapia Affaitati, Domenico De Cesare, Maria Adele Giamberardino. “Relationship between musculoskeletal symptoms and blood markers of oxidative stress in patients with chronic fatigue syndrome.” Neuroscience Letters, Volume 335, Issue 3, January 2, 2003, Pages 151-154. http://www.sciencedirect.com/science/article/pii/S0304394002010583 (Abstract)
Yam ML, Abdul Hafid SR, Cheng HM, Nesaretnam K. “Tocotrienols suppress proinflammatory markers and cyclooxygenase-2 expression in RAW264.7 macrophages.” Lipids. 2009 Sep;44(9):787-97. http://www.ncbi.nlm.nih.gov/pubmed/19655189 (Abstract)
WHEY PRODUCTS
Colostrom, Undenatured Whey, Probioplex
COLOSTRUM
DESCRIPTION. Colostrum is the first milk produced by the mother in late pregnancy and just after birth.
BACKGROUND. Because babies are born with immature digestive systems, colostrum delivers important nutrients – proteins, vitamins, and sodium – in a concentrated form. Colostrum also helps the newborn to clear excess bilirubin from its system, which prevents jaundice. Most important, colostrum contains antibodies, such as IgA, IgG, and IgM, three major components of the immune system. Colostrum also contains cytokines, interleukins, and tumor necrosis factor as well as a number of growth factors. The antibodies in colostrum provide immunity, while growth factors stimulate the development of the GI system, which together provide the newborn with its first protection against pathogens.
546
USES IN CFS/ME. Gut problems (including leaky gut, small intestine bacterial overgrowth (SIBO), irritable bowel, and motility problems) are endemic in CFS/ME patients. Colostrum may be beneficial for all these conditions. Many allergists believe that colostrum helps food intolerance and allergies.
PROTOCOL. Dr. Teitelbaum recommends three capsules of colostrum three times a day for six to nine months. Then stop, or use the lowest dose needed for symptoms. If nausea or indigestion occurs, lower the dose to a comfortable level for one or two weeks until symptoms pass. Take first thing in the morning on an empty stomach.
PROS AND CONS. Some patients report increased energy after taking colostrum for a few weeks. As with other milk-based products, however, many patients are sensitive to colostrum.
AVAILABILITY AND COST. Colostrum is available from health food stores and from online distributors. Symbiotics sells a 60-capsule bottle of Colostrum Plus (950 mg) for around $10 through Vitacost. Jarrow and Source Naturals also market colostrum capsules for roughly the same price.
FURTHER READING
Colostrum and leaky gut: http://www.carttonic.com/files/file_download.php?fi_id=684
RESEARCH
Hanson LA, Ahlstedt S, Andersson B, Carlsson B, Fällström SP, Mellander L, Porras O, Söderström T, Edén CS. “Protective factors in milk and the development of the immune system.” Pediatrics. 1985 Jan;75(1 Pt 2):172-6. http://www.ncbi.nlm.nih.gov/pubmed/3880886 (Abstract)
UNDENATURED WHEY
DESCRIPTION. Undenatured, or non-denatured, whey is a form of whey (the liquid part of milk after it has curdled) which has not been subjected to high temperatures.
BACKGROUND. Undenatured whey has been used primarily for protein supplementation. It contains all the amino acids in their natural unoxidized forms. Undenatured whey helps control unfriendly bacteria in the gut, and supports the immune system. The unoxidized cysteine is easily absorbed by the liver, and can be used to make glutathione.
In 1991 Bounous and Gold found that when mice were fed undenatured whey, their glutathione levels rose. (These findings were confirmed by later studies by Pacheco et al.) Further research has shown that undenatured whey's effect on glutathione levels can ameliorate liver disease, asthma, and diabetes.
USES IN CFS/ME. In CFS/ME patients, undenatured whey has been used to increase glutathione levels in patients who do not respond to direct glutathione supplementation. Dr. Cheney found that in his patients, results with reduced glutathione and with glutathione precursors (e.g., NAC) were “modest.” He began
547
using a weakly hydrolyzed whey protein and noted positive results. This prompted Dr. Cheney to embark on a six-month trial using ImmunoPro on a small subset of patients. At the end of the study, the patients were tested for bacterial and viral titers. He found that chlamydia pneumoniae, mycoplasma incognitus, and mycoplasma penetrans were eradicated after six months. Dr. Cheney did not find similar results with viral levels, but cautions that the study was not large enough to draw conclusions.
PROTOCOL. Dr. Cheney's study patients were given two packs a day (10 mg, or 1.75 tablespoon per pack) of undenatured whey (ImmunoCal), but he reports that patients can take more as results are dosage dependent. (The higher the dose, the greater the effect.) Undenatured whey should be taken on an empty stomach with a bit of water or milk (not juice).
PROS AND CONS. Those who respond to undenatured whey report a marked increase in energy. Unfortunately, a number of CFS/ME patients report “die-off” type reactions (sore throats, swollen glands and flu-like symptoms) at even the smallest doses. According to Richard Van Konynenburg, the lack of tolerance could be due to a reaction to casein, or (and this is most likely) to the fact that when glutathione is raised, it stimulates the immune system. Immune system stimulation is often mistaken for “die-off.”
AVAILABILITY AND COST. ImmunoPro, the brand Dr. Cheney currently recommends, can be purchased from online distributors. Amazon.com markets a 10.6-oz (300 gm) container for $33. At one scoop a day, the container will last for two months. Swanson and ProHealth sell good quality undenatured whey for a similar price.
FURTHER READING
Patient thread on nondenatured whey, including an excellent explanation of how these products work by Rich Van Konynenburg http://forums.phoenixrising.me/showthread.php?9596-Whey-powder-any-CFS-issues-benefits
Information about whey and lactoferrin: http://www.wellwisdom.com/pages/Whey-Facts.html
Dr. Cheney talks about whey protein and glutathione http://www.wellwisdom.com/pages/Whey-Facts.html#10tharticle
Carol Sieverling's article about whey, Cheney and glutathione. http://www.prohealth.com/library/showarticle.cfm?libid=8874
Detailed information on whey and glutathione http://www.nutritionadvisor.com/glutathione.html
RESEARCH
Bounous G, Gold P. “The biological activity of undenatured dietary whey proteins: role of glutathione.” Clin Invest Med. 1991 Aug;14(4):296-309. http://www.ncbi.nlm.nih.gov/pubmed/1782728 (Abstract)
548
Chitapanarux T, Tienboon P, Pojchamarnwiputh S, Leelarungrayub D. “Open-labeled pilot study of cysteine-rich whey protein isolate supplementation for nonalcoholic steatohepatitis patients.” J Gastroenterol Hepatol. 2009 Jun;24(6):1045-50. http://www.ncbi.nlm.nih.gov/pubmed/19638084 (Abstract)
Pacheco MT, Sgarbieri VC. “Effect of different hydrolysates of whey protein on hepatic glutathione content in mice.” J Med Food. 2005 Fall;8(3):337-42. http://www.ncbi.nlm.nih.gov/pubmed/16176144 (Abstract)
PROBIOPLEX
DESCRIPTION. Probioplex is a whey-derived product that concentrates the active globulin (immune) proteins in cow milk.
BACKGROUND. Probioplex is a source of secretory IgA, the immunoglobulin found in mucosal secretions. Secretory IgA is produced in the mucous lining of the intestines and is essential both for maintaining the gut barrier and for "tagging" unfriendly organisms in the gastrointestinal tract. It is used in the treatment of leaky gut, ulcers, and damage to gut mucosa. Secondary benefits include increased immune system efficiency, reduction of yeast overgrowth, and control of enteric viral and bacterial infections.
USES IN CFS/ME. Probioplex is recommended for treating digestive tract problems, particularly leaky gut, irritable bowel syndrome, gas, and food sensitivities. It may serve as a substitute for L-glutamine for those who cannot tolerate amino acids, as it performs a similar function. Probioplex also stimulates the growth of helpful bacteria in the intestines, making it a useful corollary treatment for Candida overgrowth, which is common in CFS/ME. The secondary benefits of improving immune system function are also highly relevant for patients with CFS/ME.
PROTOCOL. Probioplex is a powder that can be mixed with water or juice. Nutritionists recommend ½ teaspoon two to three times a day for 3 to 4 weeks. After that, the dosage should be reduced to ¼ teaspoon once or twice a day and discontinued when benefits are no longer noticeable. Reported benefits include reduced abdominal pain due to gas, reduced bloating, relief of constipation, reduced food reactivity, and improved sleep.
PROS AND CONS. Probioplex is safe, easy to use, relatively inexpensive, and is available without prescription. It resists digestion in the stomach and small intestine and so may be taken with meals. However, because it is a whey product, persons with milk allergies or sensitivities may not be able to tolerate it. Probioplex also contains rice maltodextrin, which may limit its value for those with rice allergies.
AVAILABILITY AND COST. Probioplex is available from specialized vitamin stores and from online suppliers. A 90-gm container (a one-month supply) costs about $30 from PureFormulas.com.
549
ACUPRESSURE
DESCRIPTION. Acupressure (or G-Jo) is a Chinese technique for the immediate treatment of minor ailments based on the same principles as acupuncture (see Acupuncture).
BACKGROUND. Acupressure was developed to provide a fast remedy for various symptoms and ailments. Much like acupuncture, it relies on stimulation of certain points on the surface of the body to release chi, or life energy. Instead of needles, the fingertips are used to apply pressure. Usually, light pressure is exerted for only a few seconds with the tip of the thumb. Most points are located by placing the fingers along easily identifiable body landmarks. Distance between points is measured in finger widths. The technique is easy to learn and requires relatively little exertion.
USES IN CFS/ME. Acupressure can be used for short-term relief of mild to moderate CFS/ME symptoms, such as minor aches and pains, insomnia, anxiety, shortness of breath, nausea, headache, eyestrain, and tension.
FOR NAUSEA, INSOMNIA, INDIGESTION, AND NERVOUSNESS
Inner Wrist Point (P6)
Place your three middle fingers crosswise along the inside of your wrist. The third finger should align with the first crease that separates your hand from your wrist. The inner wrist point is located directly under the index finger, in the middle of your arm.
FOR INDIGESTION
Bottom Of Abdomen (CV6)
CV6 is two finger widths under the belly button. Wait for two hours after eating before using this points. Do not massage for longer than two minutes.
FOR GERD
Midline Of The Body (CV12)
The point CV12 is on the midline of the body, halfway between your breastbone's base and your belly button. CV6 is two finger widths under the belly button. CV12 specifically treats heartburn. Wait for two hours after eating before using this point. Do not massage for longer than two minutes.
FOR SHORTNESS OF BREATH, CHEST TENSION, COUGHING, AND CONGESTION
550
Inner Shoulder Point
This point is located on the outer part of the chest near the shoulder, four finger widths above the armpit and one finger width toward the chest.
FOR GENERAL MUSCLE TENSION, ANXIETY, LEG SPASMS, AND INSOMNIA
This point is located at the base of the spine, approximately at the top of the hip bone, four finger widths from the spine.
FOR FATIGUE, WEAKNESS, AND PAIN
Foot Points
The Chinese believe that the lines of chi, which run throughout the body, end in the feet. For this reason, the feet are a rich source of acupressure points for all kinds of problems. Many people with CFS/ME find that exerting pressure with the tip of the thumb over the entire bottom of the foot provides relief from generalized achiness.
FURTHER READING
General information about acupressure, including pressure points: http://www.acupressure.com/
Acupressure points for GERD: http://www.livestrong.com/article/191417-acupressure-point-for-gerd/
Video showing acupressure point for anxiety, panic attacks and palpitations. (There are several youtube videos demonstrating acupressure points.): http://www.youtube.com/watch?v=7ZTHjjGtuDA
Acupressure point finder. http://pointfinder.org/
BOOK
Blate, Michael. The Natural Healer's Acupressure Handbook. Falkynor Books, 1983.
ACUPUNCTURE
DESCRIPTION. Acupuncture is a therapeutic technique in which small needles are inserted under the skin at chi points to promote the repair and healing of major organs, regulate body metabolism, and correct physical ailments that result from imbalances in the flow of chi.
BACKGROUND. The Chinese invented acupuncture sometime in the third millennium BC, but it was not systematized until 200 BC, when the Hungdi Neiging Suwen (The Yellow Emperor's Classic of Internal Disease) was written. Acupuncture is based on the concept of chi, which is life energy. In the Chinese conceptual system, chi flows along channels throughout the body, which can be felt
551
at specific points. When a person is ill, these points become tender. The acupuncturist can discern the nature of the illness and treat it by finding the tender points and stimulating them with small needles inserted just under the surface of the skin. Many years of rigorous training, as well as considerable talent, are required to be able to locate these acupuncture points.
Because the concept of vital energy, or "life force," is entirely absent in European conceptions of illness, it is difficult to say how acupuncture works. The system of meridians does not correspond to the central nervous system (CNS) or any other physiological system, insofar as anatomists can determine. There has been speculation that some of the effects produced by acupuncture may result from localized stimulation of cortisol or perhaps a kind of "distraction" of the CNS utilizing electrical fields or endorphins; the mechanism, however, is still not readily explained using the European model of the body.
Acupuncture produces distinct effects in about 80% of patients, whereas 20% note no effect. In China, acupuncturists use acupuncture to treat any condition that is reversible. They also use it to block pain. Since the late 1950s, more than 600,000 operations have been performed in China using acupuncture analgesia. Acupuncture has also been used successfully to treat animals.
USES IN CFS/ME. Several dozen studies investigating the use of acupuncture for CFS/ME have been published. Unfortunately for non-Chinese speakers, most of these have not been translated. (Although the abstracts of many of them can be viewed on PubMed.) The vast majority of these studies have shown that CFS/ME patients experience a reduction in symptoms, particularly pain, fatigue, and brain fog.
PROTOCOL. During acupuncture, the patient lies on a table while the acupuncturist places small sterile needles under the skin. (Needle insertion is painless.) Usually, the acupuncturist will first "pulse" you, that is, measure the flow of chi. The effectiveness of the treatment is determined by the size of the bore of the needle, how long it is left in place, the depth of penetration, how much it is moved, and how often the treatment is repeated. Sometimes one treatment is all that is needed to achieve the desired effect. For complicated or severe problems, sessions may be needed two or three times a week.
Acupuncturists are also trained in Chinese herbal medicine. Certain Chinese herbs may be recommended as part of the acupuncture therapy. Moxa (herbal incense) is also used to provide localized heat. Many people with CFS/ME, particularly those with chemical sensitivities, cannot tolerate the odor of Moxa. Be sure to discuss any sensitivities with your acupuncturist before Moxa treatments.
PROS. Acupuncture provides an alternative to drug treatment. Patients note improvements in generalized pain, eye pain, overall well-being, mental clarity, and energy. Positive results are most often obtained when the treatment focuses on specific problems, such as pain, insomnia, loss of appetite, or nausea.
CONS. Negative results in many cases are due to the acupuncturist's mistaken idea that people with CFS/ME have depressed immune systems and, as a
552
consequence, require immune system stimulation. In severely ill CFS/ME patients, immune system stimulation can cause a profound exacerbation of symptoms.
AVAILABILITY AND COST. Acupuncture is available in most urban centers in the United States and is becoming increasingly more so. Fees vary, but most acupuncturists charge $70 to $95 per treatment. Insurance in some states covers the cost, especially if the acupuncturist is also a physician. Make sure to check the acupuncturist's credentials, how long he or she has been practicing acupuncture, and whether he or she has any experience with CFS/ME. If possible, talk to another person with CFS/ME who has been a patient.
FURTHER READING
This is a good general article about acupuncture for CFS/ME: http://www.cfids.org/archives/1999/1999-5-article03.asp
Acupuncturists talk about treating CFS/ME. The article includes specific points and meridians. http://www.chirofind.com/mpacms/at/article.php?id=30188
Detailed summary of several acupuncture studies performed in China. Results are analyzed and discussed: http://findarticles.com/p/articles/mi_m0ISW/is_265-266/ai_n15688805/
RESEARCH
Chen XH, Li LQ, Zhang W, Yang J, Dai YS, Xu DH, Tang CZ. [Randomized controlled study on acupuncture treatment for chronic fatigue syndrome]. Zhongguo Zhen Jiu. 2010 Jul;30(7):533-6. http://www.ncbi.nlm.nih.gov/pubmed/20862932 (Abstract)
Marshall R, Paul, L and Wood L. “The search for pain relief in people with chronic fatigue syndrome: a descriptive study.” Physiother Theory Pract. 2011 Jul;27(5):373-83 http://www.ncbi.nlm.nih.gov/pubmed/21039301 (Abstract)
Wang JJ, Song YJ, Wu ZC, Chu XO, Wang XH, Wang XJ, Wei LN, Wang QM. [A meta analysis on randomized controlled trials of acupuncture treatment of chronic fatigue syndrome]. Zhen Ci Yan Jiu. 2009 Dec;34(6):421-8. http://www.ncbi.nlm.nih.gov/pubmed/20209981 (Abstract)
AROMA THERAPY
DESCRIPTION. Aroma therapy involves use of the distilled essential oils naturally found in plants for healing and cosmetic purposes.
BACKGROUND. For centuries, aromatic oils have been recognized for their medicinal properties. In biblical times, oil of myrrh, which is a powerful antiseptic, was revered for its power to quickly heal surface wounds (hence the significance of the gift of the Magi). When Tutankhamen's tomb was opened in 1922, scent pots of frankincense were found. The range of uses for essential oils appears limitless.
Essential oils can be used to induce sleep (e.g., jasmine), calm the nerves (e.g., valerian, clary sage), clean wounds (e.g., lavender), reduce aches and pains (e.g., rosemary), relieve gas pains (e.g., peppermint), and open respiratory airways (e.g., basil). The mode of action of aromatic oils is complex. A single oil can produce
553
a number of different, and even opposing, effects. Lavender, for example, sedates in small quantities but stimulates in larger quantities.
It is not known how plant oils produce these effects in people, but it has been theorized that smell, our most primordial sense, stimulates a complex set of central nervous system (CNS) reactions that can culminate in emotional and physiological changes. It is well known that the ketones, esters, aldehydes, and alcohols found in plant oils can serve as insect repellents, fungicides, and bactericides. Many oils also have hormone-like properties (for example, hops, fennel, and anise contain estrogens).
Production of essential oils is a long, arduous process involving oil-based extraction and repeated distillation (alcohol is never used). It takes many pounds of flowers, leaves, or bark to produce 1/3 oz of concentrated essential oil, which is why only a drop or two produces the desired effect.
USES IN CFS/ME. Aroma therapy may hold promise for the alleviation of some CFS/ME symptoms, because odors readily cross the blood-brain barrier. Because the olfactory bulbs tie in directly to the limbic system (that part of the brain that processes emotion), essential oils may be useful in alleviating emotional symptoms such as anxiety, anger, and fear. Essential oils can also be effectively used to relieve insomnia and muscle aches. A number of patients who have tried aroma therapy have reported good results in treating anxiety, "jitters," and insomnia, with no negative side effects.
To relieve chronic, severe stress, Valerie Worwood, author of The Complete Book of Essential Oils and Aromatherapy, recommends use of hypnotics such as narcissus for hyperactivity, jonquil for anxiety, jasmine for depression, carnation or valerian for insomnia, and vanilla for general stress. Oils that can help relieve muscle fatigue include rosemary, thyme, and marjoram. To treat insomnia, a blend of sandalwood, clary sage, lemon, and chamomile may be helpful. Lavender has been shown to act as an anticonvulsant.
In Chronic Fatigue Syndrome: A Natural Healing Guide, Steve Wilkinson recommends the following oils to treat symptoms of CFS/ME: lavender (for tension), lemon (to calm the mind, night sweats), peppermint (for fever, night sweats, digestive disorders), basil or orange (to lift the spirit), rosemary (for lethargy), clary sage (for invigoration), and geranium (for sluggishness and emotional upset).
PROTOCOL. Essential oils are always used by the drop. Measurements are precise, so you should have a "recipe." (See some of the sites below.) The oils are not meant to be taken internally. They can be rubbed on the skin (after thorough cleansing), inhaled, or floated in a bath. When applied directly to the skin, they must be mixed with vegetable oil. To make a rub for the skin, slightly warm two tablespoons of pure vegetable oil (corn, safflower, sunflower, peanut, or soy oils are all readily obtained and make good mediums) and add four or five drops of essential oil (or one each of several oils if you are making a blend).
You can also add the oils to bathwater before getting into the tub. One or two drops of lavender is all you need for a relaxing bath. To treat insomnia, try placing one or two drops of clary sage, jasmine, or any of the hypnotics on a handkerchief
554
and place it near your pillow. The oils are strong, so not much is needed. Breathing the vapor from a single drop of peppermint oil floated in a cup of hot water can relieve gas pain instantly, and help clear the sinuses, too!
PROS AND CONS. Essential oils are benign when used externally and in small amounts. Aroma therapy can prove particularly useful for treating gastrointestinal disturbances because the oils are not processed through the GI tract. Oils can be a good therapy option for those who are sensitive to synthetic chemicals, because they generally do not provoke reactions. Because the oils work synergistically, you may want to do some investigation online for the most effective blends. Follow your nose to choose the oils that are best for you. (If it smells bad to you, don't buy it.) Those with MCS, multiple allergies or hypothyroidism may not be able to tolerate essential oils.
AVAILABILITY AND COST. Essential oils can be purchased at health food stores and online. They are usually sold in 1/3-oz bottles. Given the tiny doses, one bottle can last for years. Aura Cacia is one of the better known suppliers. The common oils are not expensive. A bottle of peppermint oil costs about $4.
FURTHER READING
Essential oil blends for enhancing mood: http://www.aromatherapy.com/mood_blends.html
Comprehensive aromatherapy recipes: http://www.aromaweb.com/recipes/default.asp
Aromatherapy for CFS/ME (with recipes): http://www.dreamingearth.com/chronicfatigue.html
Excellent list of essential oils useful for CFS/ME patients. http://aboutmecfs.org.violet.arvixe.com/Trt/AromatherapyEssentialOils.aspx
RESEARCH
Woelk H, Schläfke S. “A multi-center, double-blind, randomised study of the Lavender oil preparation Silexan in comparison to Lorazepam for generalized anxiety disorder.” Phytomedicine. 2010 Feb;17(2):94-9. http://www.ncbi.nlm.nih.gov/pubmed/19962288 (Abstract)
BACH REMEDIES
DECRIPTION. Bach remedies are herbal essences principally derived from flowers used to remedy specific physical or psychological complaints.
BACKGROUND. Bach remedies were devised by Dr. Edward Bach, a British bacteriologist, in the 1930s. In the 1920s, he proposed the theory that altered mental and emotional states were brought about by disharmonies that could be corrected with the use of plant essences. Dr. Bach collected these essences, at first, by gathering the dew that had collected on the underside of leaves and flower petals. Because this method proved arduous, he later tried putting plant parts in a bowl of pure spring water, which he left in the sun for a few hours. He then preserved the water in alcohol. To make his remedies, he took a few drops from the
555
bottled essence and added them to an ounce of pure water. He administered four drops in a little water four times a day.
By the time of Dr. Bach's death in 1936, he had discovered 38 such herbal remedies. Dr. Bach claimed that his flower remedies cured various common physical ailments, but primarily the remedies were used to treat emotional problems. For example, he treated fearfulness with mimulus, obsessional thoughts with white chestnut, lack of faith with gentian, and general ailments with a blend of five of the essences, which he called "Rescue Remedy."
USES IN CFS/ME. Although there is no scientific evidence proving the effectiveness of Bach remedies, some people with CFS/ME report good results. Aspen is reputedly effective for fear. Patients report success using scleranthus to control night sweats. Given the low risk associated with Bach remedies, scleranthus might be worth trying if night sweats are severe or resistant to other treatment. Rescue Remedy, a blend of several essences that alleviates many symptoms simultaneously, is popular among those who use Bach remedies to relieve stress and improve sleep.
PROTOCOL. Standard dosage is three to seven drops placed under the tongue, or in a small glass of water, taken four times a day.
PROS AND CONS. Bach remedies are generally well tolerated. Patients who are highly reactive, severely ill, or have multiple allergies may wish to start with one drop. Keep in mind that the more essences you use, the less effective the mixture will be. Try to focus on one or two problems rather than several.
AVAILABILITY AND COST. Bach remedies can be purchased at most health food stores and online. They generally cost about $7 a bottle.
FURTHER READING
A list of all Bach Flower remedies and what they are used for. http://www.bachcentre.com/centre/remedies.htm
BED REST
DESCRIPTION. Bed rest is lying down, with your eyes shut, and resting.
BACKGROUND. Resting was an integral part of daily life until the last generation. The Spanish siesta, the dinner hour, teatime, the evening cigar, and afternoon snooze all acknowledged the need to take a break from long periods of activity. Rest charges our batteries, so to speak. Bed rest was an essential part of treatment for every illness until the middle part of the twentieth century. Conscientious physicians, and mothers, have recognized throughout the ages that the body needs adequate rest to recover from daily wear and the insults of infectious disease. Given the frequent occurrence of serious infectious diseases that characterized life in the earlier part of this century, the sickbed was a place where everyone would no doubt spend time at some point during a lifetime.
Since the discovery of antibiotics, however, we have become overconfident. When we get sick, we take a pill and keep going. In contemporary society, resting is regarded as a luxury rather than a necessity, much to the detriment of our health.
556
We seem to have forgotten that the human body is fundamentally material and, like any material object, it wears down with continual use.
USES IN CFS/ME. Views on bed rest in CFS/ME are somewhat divided. More than a few (misguided) physicians are under the impression that resting makes CFS/ME patients more tired. This attitude reflects what one might call the “buck up and take it like a man” school of treatment. However, virtually every CFS/ME physician recommends bed rest as an essential part of coping with the illness, as do nearly all patients. As one patient points out, "Nothing cures better than rest." Resting seems obvious when you are tired, but all too many times we ignore what our bodies are telling us. Patients with CFS/ME learn very quickly that pushing past their limits exacerbates symptoms. Both those who are well into recovery and those who are recently ill learn this lesson over and over again: Rest is essential to recovery.
PROTOCOL. There is a method to resting. Simply lying down is not enough. In order for your body to rest, your mind must rest, too. No single part of the human body consumes more calories than the brain. If you use your rest time to study, or do taxes, or some other task, you will not reap the benefits of rest.
When you rest, lie as comfortably as you can. Listen to soothing music or do relaxation exercises. Breathe. Do nothing else. The important thing is to allow your body some time for self-repair. Resting may be considered "doing nothing" in our achievement-oriented world, but as far as your body is concerned, it is "work." Your body needs rest to reestablish a normally functioning metabolism and immune system. If you are severely ill or relapsed, you will need to rest all the time. Even if you are nearly fully recovered, include rest time during the day. Remember: Rest time is not wasted time; it is healing time.
FURTHER READING
How to pace your energy with rest: http://cfidsselfhelp.org/library/3-reducing-symptoms-with-planned-rest
More on pacing: http://www.cfidsselfhelp.org/library/4-nurture-yourself-with-pre-emptive-rest
Michael Sharpe and Simon Wessely's infamous advice to “buck up.” http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1112768/
BIOFEEDBACK
DESCRIPTION. Biofeedback is a technique in which physiological processes are monitored by a computer to enable a person to exercise control over previously unconscious body functions.
BACKGROUND. Biofeedback is a relatively new technique, although the concept of using the mind to control the body is an ancient one. Tibetan lamas and Indian yogis achieve tremendous control over unconscious functions through the practice of simple meditation techniques. In biofeedback, the patient actually sees or hears a representation of brain waves using a computer. Different brain wave patterns can be represented by fish swimming, abstract designs, or music. The
557
object is to change the pattern—make it grow or shrink, make the fish swim faster, make the music play louder— through the power of concentration.
Biofeedback has been a topic of great interest in the medical community since the 1950s. Biofeedback devices have been used to help patients regulate heartbeat, eliminate migraine headaches, and control elevated blood pressure. Ultimately, any medical problem that is affected by stress hormones can be influenced by biofeedback techniques. In CFS/ME, biofeedback may be useful in reducing symptoms exacerbated by a dysregulation of the hypothalamus-pituitary-adrenal axis because adrenal hormones are sensitive to brain wave output.
USES IN CFS/ME. There is no doubt that the nervous system plays an important role in generating, or exacerbating, the fatigue and cognitive impairment experienced by CFS/ME patients. A number of studies have reported abnormalities in EEG (brain wave) patterns in CFS/ME patients.
In 1997, researchers at the University of West Florida compared the EEGs of a group of 28 CFS/ME patients with age- and gender-matched controls. They found that the CFS/ME subjects displayed greater impairment than non-controls in that they generated higher microvoltage activity in the lower frequencies (5-7 Hz, the stage of light sleep, also known as theta waves). The authors concluded that “the increased microvolt levels found in the lower frequencies in CFS subjects may be indicative of deficits in information processing speed, psychomotor activity, attention, retrieval of information from semantic memory, and logical reasoning.” Basically, this means CFS/ME patients are functionally asleep while in the waking state.
More recently, in 2011 Duffy et al used EEG patterns to differentiate between patients with CFS/ME, patients with depression and healthy controls. The researchers found that EEGs correctly identified unmedicated patients with CFS/ME and healthy control subjects without misclassifying depressed patients as having CFS/ME. This study provides concrete evidence that CFS/ME patients demonstrate brain physiology that is not observed in healthy normals or patients with major depression.
In 1993, Michael Tansey, a researcher in Somerville, New Jersey, successfully used neurofeedback techniques to reduce cognitive confusion, pain, headaches, and cold extremities in a CFS/ME patient who had had severe symptoms for 2 ½ years (CFIDS Chronicle, Fall 1993). He placed sensors along the top of the skull, just above the supplemental motor area (SMA) of the brain, with the idea that because that area controls limbic outflow and the flow of sensory information, resolution of abnormal brain waves in the SMA would result in cessation of cognitive, verbal, and motor control problems.
Three years later, James and Folen, two psychologists in Hawaii, published a case report in which they measured a CFS/ME patient's response to neurofeedback using a standardized tool (the Wechsler Adult Intelligence Scale). The results revealed improvements in the patient's cognitive abilities, functional skill level, and quality of life.
558
Myra Preston, Ph.D., a biofeedback therapist practicing in Charlotte, North Carolina, has patented a neurofeedback technique that in some patients has resulted in a significant decrease in cognitive problems (CFIDS Chronicle, Winter 1996). She uses the basic biofeedback apparatus together with an EEC to correct the excess delta wave (slow wave) anomaly found in people with cognitive difficulties. Dr. Preston argues that when the brain wave pattern reverts to normal, many central nervous system (CNS) symptoms will recede, including difficulty in concentrating, headaches, and insomnia.
Preston's theories were supported by a study published in 2001, in which a young woman with sudden onset CFS/ME was treated with neurofeedback and self-hypnosis. Her EEG showed excessive theta wave activity (characteristic of light sleep) in the left frontal lobe. After being treated with neurofeedback and self-hypnosis, the patient experienced considerable improvement in fatigue, vigor, and confusion. Most important, the majority of the changes were maintained at five-, seven-, and nine-month follow-up testing.
PROS AND CONS. As a treatment modality, biofeedback is completely safe. Patients with CFS/ME have successfully used biofeedback to treat cognitive problems, headache, anxiety, cold hands, and for general relaxation. Because the technique is noninvasive and seems to address one of the core CFS/ME problems, it may hold great promise for those with severe CNS and cognitive problems. The main drawback of biofeedback is that it requires frequent training sessions and daily practice. Many of the more seriously ill CFS/ME patients may not feel up to the time commitment.
AVAILABILITY AND COST. Biofeedback has become so popular in recent years that finding a clinician who uses it is not difficult. In general, clinicians who use the technique are psychologists. To find a certified specialist check the Association of Applied Psychophysiology and Biofeedback's website. The cost of biofeedback depends on the hourly fees charged by the practitioner. Sometimes insurance covers the cost, but check with your carrier first.
FURTHER READING
“Neurotherapy: Rehabbing the CFS/ME brain.” Winter 2003 CFIDS Chronicle article discussing the benefits of neurotherapy for CFS/ME: http://www.cfids.org/archives/2003/2003-1-article07.asp
The Association of Applied Psychophysiology and Biofeedback maintains a very useful consumer section. The section contains a list of disorders, information on how biofeedback works, efficacy information, research and how to find a provider: http://www.aapb.org/consumers.html
Biofeedback Research Institute's website. Click on “What is Biofeedback” for a detailed description of a biofeedback session: http://www.7hz.com/
A very thorough account of one patient's experience with biofeedback. Includes photos. http://fibrofriends.typepad.com/fibro_friends/2010/05/biofeedback-therapies-for-cfs-fms.html
Myra Preston's site: http://www.siberimaging.com/index.html
559
RESEARCH
Billiot, Katherine M.. M.A., Thomas H. Budzynski, Ph.D., and Frank Andrasik, Ph.D. “EEG Patterns and Chronic Fatigue Syndrome.” Journal of Neurotherapy. 1997, (2-2)4. http://www.kbcsolutions.co/uploads/chronicfatigue.pdf
Duffy, Frank H, Gloria B McAnulty, Michelle C McCreary, George J Cuchural, and Anthony L Komaroff. “EEG spectral coherence data distinguish chronic fatigue syndrome patients from healthy controls and depressed patients-A case control study.” BMC Neurology. 2011, 11:82 http://www.biomedcentral.com/1471-2377/11/82/abstract
Hammond DC. “Treatment of chronic fatigue with neurofeedback and self-hypnosis.” NeuroRehabilitation. 2001;16(4):295-300. http://www.ncbi.nlm.nih.gov/pubmed/11790917 (Abstract)
James LC, Folen RA. “EEG biofeedback as a treatment for chronic fatigue syndrome: a controlled case report.” Behav Med. 1996 Summer;22(2):77-81. http://www.ncbi.nlm.nih.gov/pubmed/8879459 (Abstract)
CHELATION THERAPY
DESCRIPTION. Chelation therapy involves use of intravenous EDTA (ethylene diaminete tra-acetic acid) to bind and remove metal molecules from the body.
BACKGROUND. Chelation was developed in the late 1940s to treat lead poisoning. It had been discovered about a decade earlier that EDTA, a synthetic amino acid compound, had the ability to bind with calcium. (As a consequence, EDTA is classified as a calcium channel blocker.) The resulting calcium combinations then bind with heavy metals in the bloodstream and remove them by way of the kidneys and bladder. Although the only approved use of chelation in the United States is to treat heavy metal poisoning (chiefly lead, arsenic and iron), chelation therapy has also been used to treat chronic degenerative diseases such as diabetes, stroke, cataracts, senility, Parkinson's disease, and osteoporosis. Currently, chelation is being tested for treatment of coronary artery disease.
USES IN CFS/ME. Not many CFS/ME physicians have included chelation in their protocols, though, in theory, chelation could offer considerable benefit to patients in whom CFS/ME was triggered by exposure to pesticides or other toxic chemicals. In these cases, chelation would remove toxins and heavy metals which continue to cause symptoms and exacerbate immune system irregularities.
In 1994 Dr. Boergman of South Africa reported a 100% improvement rate in 16 CFS/ME patients using EDTA chelation (CFIDS Chronicle, Summer 1994). One of Dr. Boergman's patients recovered totally after 10 infusions. The others reported 60% to 90% recovery from physical and mental symptoms. However, it is important to note that Dr. Boergman's study was quite small and has not been replicated. Other physicians have not substantiated Dr. Boergman's findings.
560
There is a subset of health practitioners who believe that mercury amalgams are responsible for CFS/ME. They routinely advise patients to have the amalgams replaced, followed up by chelation therapy to remove mercury from the body. While some people have gone through this costly process, most have not found relief from CFS/ME symptoms.
PROTOCOL. EDTA chelation can be administered by intravenous drips, suppositories, and orally. The recommended frequency of treatment is once a week. Daily chelation is not advised. The main chelating ingredient used in IV therapy is EDTA, but other chelators such as vitamin C, vitamin A, heparin, and selenium may be added to the infusion to boost the chelating power of the mixture. Suppositories can be taken up to three times a week. A less expensive, and less risky, form of chelation can be accomplished orally with natural chelating agents such as vitamin C (4000 mg/day) and lipoic acid.
PROS AND CONS. Side effects of chelation include decreased blood pressure, hypoglycemia, joint pain, fatigue, weakness (due to potassium depletion), and peeling of the skin (due to decreased zinc and vitamin B6 levels). Because the chelated compounds are excreted through the kidneys, chelation can damage those organs. Chelation is contraindicated in patients with a history of kidney, liver, or bladder disease (such as interstitial cystitis).
Chelation also depletes the body of vitamin B6 and minerals such as potassium, zinc, magnesium, calcium, and chromium. In patients with low concentrations of these vitamins and minerals, a long course of chelation therapy can cause considerable damage. Before starting chelation therapy, nutritional status should be checked and corrected if necessary. In any case, nutritional supplementation is necessary during chelation therapy. (Be sure your physician is familiar with the American College of Advancement in Medicine protocol before chelation therapy is started.) Chelation can cause sudden cardiac arrest resulting from hypocalcemia. At least thirty deaths have been attributed to chelation therapy.
AVAILABILITY AND COST. Each chelation treatment costs around $100, depending on where it is performed (costs are higher on the east and west coasts) and whether other supporting therapies are included. With additional tests and supporting treatments, an entire course of treatment may cost well over $2000. Insurance companies usually require a predetermination for this treatment to establish "medical necessity," so check with your carrier first. Suppositories are less expensive at $8 a day, but like IV chelation, should be supervised by an experienced physician.
FURTHER READING
This is a commercial site, but it contains a good summary of different forms of chelation. http://www.chelationhealthproducts.com/why_kelatox_suppositories.php
CDC report of deaths related to chelation therapy. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5508a3.htm
561
"Why the NIH Trial to Assess Chelation Therapy (TACT) Should Be Abandoned." http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2438277/
This is a lengthy, well-documented report written by a team of doctors about the hazards of chelation therapy. It reports 30 deaths resulting from chelation therapy.
CHIROPRACTIC
DESCRIPTION. Chiropractic is the technique of manipulating the spinal column and body joints to alleviate back or joint pain.
BACKGROUND. Although hands-on manipulation of the joints and spine was practiced in ancient Egypt and Assyria, the technique was not popularized in the United States until the late 1800s, when D. D. Palmer founded the practice. The central premise of traditional chiropractic is that subtle deviations of the spinal column, called subluxations, can interfere with nerve transmissions, causing various health problems. The chiropractor, by manipulating the vertebrae back into their normal position and giving recommendations about exercise and posture improvement, can remove irritation to the nerves that may be causing pain.
USES IN CFS/ME. Chiropractic is normally used to treat back and joint pain, although it also helps alleviate a broad range of related symptoms such as insomnia, headaches, and sciatica.
PROTOCOL. Most chiropractors prefer to see their patients two or three times a week. It may take up to 12 sessions to note improvement.
PROS AND CONS. Results in CFS/ME are mixed. Some patients claim relief from headaches and muscle pain, which, in turn, has helped them sleep. An equal number say chiropractic worsens their pain. The muscles and other tissues surrounding the spine are exquisitely sensitive. The traditional form of chiropractic, in which the spine is abruptly "popped" with a sharp hand movement, may place too much strain on these tissues, causing injury. (Neck manipulations carry the risk of stroke, and should be avoided.) The pain generated by such treatment may last for days, sometimes weeks. Patients interested in trying chiropractic for the first time might want to try a more gentle form of chiropractic, such as Network Chiropractic.
AVAILABILITY AND COST. Chiropractic adjustments average $65 per visit. Initial visits, which may include taking a history and x-ray examination, may cost more. Many insurance companies cover the cost of chiropractic treatment.
MORE INFORMATION
The Association for Network Chiropractic website. http://www.associationfornetworkcare.com/whatisnsa.shtml
Database for locating chiropractors: http://www.chirofind.com/mpacms/dc/locator/home.php
COGNITIVE BEHAVIORAL THERAPY (CBT)
DESCRIPTION. Cognitive Behavioral Therapy (CBT) is a psychotherapeutic approach used by psychologists to treat dysfunctional behaviors.
562
BACKGROUND. In a departure from traditional psychotherapy, which focuses on events of the past, CBT focuses on present behaviors and problems and seeks practical solutions.
CBT was primarily developed through an integration of behavior therapy, a form of therapy that utilizes behavioral conditioning, and cognitive therapy, a form of therapy developed in the 1960s that helps patients overcome dysfunctional beliefs. CBT is primarily used for psychological disorders that are rooted in the patient's basic concepts, ones that he or she may not be aware of. Through a partnership with the therapist, the patient learns to recognize and eliminate ideas which are contributing to dysfunctional behaviors.
CBT is best used for conditions in which dysfunctional behavior has a psychological or cognitive basis, such as bulemia, phobias, obsessive-compulsive disorder, post traumatic stress disorder, social phobia, generalized anxiety, and some forms of depression. It is particularly effective for eating disorders. CBT has not been shown to be effective for schizophrenia, bipolar disorder, addictions, or major depression.
USES IN CFS/ME. According to its proponents, CBT is a safe, effective treatment because “patients gradually shift their fixed ideas that they are helpless against the fatigue that dominates their lives and move to the perception that fatigue is only one negative experience among many positive ones.” Because CFS/ME is classed as a mental illness in the U.K., CBT has been officially endorsed as a CFS/ME treatment in Great Britain. Numerous studies, conducted primarily in the U.K., have appeared to support the efficacy of CBT for treating CFS/ME. However, these studies have not been replicated elsewhere.
In a special edition of the Journal of Chronic Fatigue Syndrome (Vol 11, (1) 2003), an article written by a panel of eleven CFS/ME physicians discussed the results of several CBT studies. The authors concluded that the U.K. studies were inherently flawed. According to the Oxford case definition of CFS/ME (which was the case definition used in most of the British CBT studies), the only criterion for CFS/ME is six months of unexplained fatigue. None of the other symptoms specified by the U.S. and Canadian case definitions (sore throats, sleep disturbance, pain, exercise intolerance, etc.) are required.
This very broad case definition allows patients with other disorders, such as depression, to be included under the designation of CFS/ME. The authors of the article noted that “a systematic review of prognosis studies show that the less stringent the clinical criteria, the better the prognosis.” In short, studies demonstrating the efficacy of CBT for CFS/ME patients tend to yield much better results when subjects without CFS/ME are included. The authors concluded that “to ignore the demonstrated biological pathology of this illness, to disregard the patient's autonomy and experience and tell them to ignore their symptoms, all too often leads to blaming patients for their illness and withholding medical support and treatment.”
Even in the face of rising criticism, the proponents of CBT have maintained their position. But in 2008 a meta-analysis of 15 studies (1043 CFS/ME
563
participants) conducted by Price et al found that CBT might be more effective in reducing fatigue symptoms only when compared with other psychological therapies. The researchers noted that there were very few follow-up studies, and these showed inconsistent findings. The authors concluded that “there is a lack of evidence on the comparative effectiveness of CBT alone or in combination with other treatments.”
A year later, two Dutch researchers, Twisk and Maes, reviewed CBT and GET (graded exercise therapy) as treatments for CFS/ME/ME. The authors determined that the success claim for CBT was “unjust” and that CBT was hardly more effective than no care at all. They concluded that “it is unethical to treat patients with ME/CFS with ineffective, non-evidence-based and potentially harmful "rehabilitation therapies," such as CBT/GET.”
Finally, in 2011 a randomized controlled trial comparing CBT/GET with usual care (exercise counseling and pharmacological treatment) conducted by Núñez et al found that after twelve months the CBT/GET group showed no improvement in health-related quality of life and actually declined in physical function and bodily pain.
PROTOCOL. A typical CBT course consists of between twelve and sixteen hour-long sessions. (Note that a therapist's “hour” is 50 minutes.) A typical cognitive therapy program may involve keeping an “energy diary” in which the patient reports any psychological or social factors, such as losing a job, which might be making the fatigue worse. Patients also use the diary to track peaks and troughs in energy levels. After reviewing the diary, patients adjust their schedules in order to rest during low-energy periods, while reserving high-energy times for important activities. Because energy peaks and troughs are unpredictable, patients are encouraged to be flexible and to prioritize, dropping the least important tasks while focusing on the tasks that are essential. Patients are encouraged to set limits, manage impaired concentration, and to accept relapses. Throughout this re-training of the mind, patients are taught to reverse “negative beliefs.”
PROS AND CONS. Although many patients find some form of counseling helpful, there appears to be no evidence supporting the use of CBT as a CFS/ME treatment. Dr. Myhill has included CBT on her list of treatments “not worth trying,” noting that it makes her patients feel worse. It might be of benefit to mildly ill patients, but that group has not been included in CBT studies, and the moderately ill cohort in well-structured studies appears to suffer a decline after treatment. In a survey conducted by the 25% Severe ME Group (for severely ill CFS/ME patients), 93% of the respondents indicated that CBT was not helpful.
AVAILABILITY AND COST. CBT is practiced by many psychologists. The cost is the practitioner's hourly rate. Insurance usually covers.
FURTHER READING
Basic information about CBT in CFS/ME: http://www.cfids.org/resources/patient-ed-cbt-fsheet.asp
“Cognitive behavioural therapy for ME/CFS sufferers: How strong is the evidence?” http://www.meresearch.org.uk/research/reviews/cbt.html
564
Historical review of all CBT studies. http://www.mecfsforums.com/wiki/Cognitive_Behavioral_Therapy
RESEARCH
Carruthers, Bruce M., Anil Kumar Jain, Kenny L. De Meirleir, Daniel L. Peterson, Nancy G. Klimas, A. Martin Lerner, Alison C. Bested, Pierre Flor-Henry, Pradip Joshi, A. C. Peter Powles, Jeffrey A. Sherkey, and Marjorie I. van de Sande. “Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Clinical Working Case Definition, Diagnostic and Treatment Protocols.” Journal of Chronic Fatigue Syndrome, Vol. 11(1) 2003. http://www.cfids-cab.org/MESA/ccpc-1.html
Núñez M, Fernández-Solà J, Nunez E, Fernandez-Huerta JM, Godás-Sieso T, Gomez-Gil E. “Health-related quality of life in patients with chronic fatigue syndrome: group cognitive behavioural therapy and graded exercise versus usual treatment. A randomised controlled trial with 1 year of follow-up.” Clin Rheumatol. 2011 Mar;30(3):381-9 http://www.ncbi.nlm.nih.gov/pubmed/21234629 (Abstract)
O'Dowd H, Gladwell P, Rogers CA, Hollinghurst S, Gregory A. “Cognitive behavioural therapy in chronic fatigue syndrome: a randomised controlled trial of an outpatient group programme.” Health Technology Assessment. 2006 Oct;10(37):iii-iv, ix-x, 1-121. http://www.ncbi.nlm.nih.gov/pubmed/17014748 (Abstract)
Price JR, Mitchell E, Tidy E, Hunot V. “Cognitive behaviour therapy for chronic fatigue syndrome in adults.” Cochrane Database Syst Rev. 2008 Jul 16;(3):CD001027. http://www.ncbi.nlm.nih.gov/pubmed/18646067 (Abstract)
Maes M, Twisk FN. “A review on cognitive behavioral therapy (CBT) and graded exercise therapy (GET) in myalgic encephalomyelitis (ME) / chronic fatigue syndrome (CFS): CBT/GET is not only ineffective and not evidence-based, but also potentially harmful for many patients with ME/CFS.” Neuro Endocrinol Lett. 2009;30(3):284-99. http://www.ncbi.nlm.nih.gov/pubmed/19855350 (Abstract)
EXERCISE/GET
DESCRIPTION. Exercise includes any systematic program of body movement that is designed to strengthen, tone, or stretch muscles.
BACKGROUND. Exercise has been an important component of school health programs since the early 1960s when President Kennedy called for a new era of "vigor." Since then, exercise has become a perpetual preoccupation for health-conscious Americans, many of whom incorporate jogging, running, swimming, and regular visits to a health club into busy work schedules. Moderate exercise produces many health benefits, such as increased strength and sense of well-being, lowered risk for heart disease, reduced arthritic pain, increased mental alertness, and improvements in digestion and metabolism. For most people, exercise is indeed "good for what ails you."
565
The three basic types of exercise are aerobic, subaerobic, and anaerobic. Aerobic exercise induces systemic changes. In concrete terms, aerobic exercise is any exercise that lasts at least 12 minutes, involves deep breathing, and uses major muscle groups (thighs and buttocks). Jogging and hiking are good examples of aerobic exercise because they affect heart rate and breathing, and utilize major muscle groups. Some metabolic changes that occur as a direct result of aerobic exercise are increased utilization of oxygen, increased production of ATP (adenosine triphosphate), and increased utilization of the Krebs cycle (tricarboxylic, or citric acid cycle).
Subaerobic exercise, such as walking, golfing, nonstrenuous hiking, light weight lifting, and swimming, is what most clinicians mean by "gentle" exercise. All of these can be done without pushing the heart rate past 50% of its maximum capacity. None of these forms of exercise will produce metabolic changes unless the person is out of shape or is ill. However, they help build muscle strength and endurance. Subaerobic exercise also elevates mood, improves cognition, enhances immune system function, and improves circulation.
Anaerobic exercise is any form of aerobic exercise that pushes heart rate to its limit. A runner who reaches a point of breathlessness is exercising anaerobically. Metabolic changes induced by anaerobic exercise include increased production of lactic acid (causing burning pain in muscles), lowered ATP production, and decreased dependence on the Krebs cycle.
USES IN CFS/ME. One of the ongoing debates among CFS/ME clinicians, as well as their patients, is whether exercise is good or bad for patients with CFS/ME. The Centers for Disease Control and Prevention (CDC) maintains that patients with CFS/ME need to maintain a steady, low-impact exercise regimen to avoid becoming deconditioned. Indeed, some physicians recommend exercise as one of their chief CFS/ME therapies. Other clinicians disagree, noting that exercise is contraindicated in viral illnesses (e.g., poliomyelitis). They point out that exercise intolerance is a hallmark symptom of CFS/ME and that symptoms invariably worsen after any form of exercise.
According to Dr. Charles Lapp, exercise is the proverbial "double-edged sword." On the positive side, people mention that exercise increases their strength and helps keep them mentally alert. It also seems to have beneficial effects on the immune system. Some physicians believe gentle exercise can help reverse some of the immune system malfunction of chronic CFS/ME. Dr. Benjamin Natelson, of the New Jersey CFS Center, points out that natural killer cells decline with inactivity (CFIDS Chronicle, Winter 1996). He contends that with a "very, very gentle training program," immune markers may improve.
On the negative side, single-photon emission computed tomographic (SPECT) scans have shown that in CFS/ME patients who exercise, brain blood volume is reduced one to three days after exercising. In patients who are acutely or seriously ill, this could have profoundly deleterious effects on immune and endocrine system regulation. In patients with CFS/ME, exercise also lowers cortisol levels, which makes it more difficult for the body to control inflammation.
566
In addition, exercise in this population increases erratic breathing and leads to a rapid progression to anaerobic metabolism, which produces ammonia and lactic acid. (These results are the opposite of what would normally be expected in a healthy population.) Given the results of the Peckerman studies on cardiac insufficiency in CFS/ME patients, it would be quite risky for those who are severely ill to embark on any kind of exercise program.
In short, a simple answer to the exercise question is: if you are severely or acutely ill, exercise will only make matters worse. The time to discuss an exercise program with your physician is when clear signs of recovery are noted.
PROTOCOL. Most CFS/ME clinicians advise a very gradual reintroduction of exercise. Subaerobic exercise, that is, exercise that does not cause the body to heat up or increase heart rate, is often recommended once a patient is showing a return of overall health. (On a scale of 1-10, this would be a 5.) This form of exercise helps keep muscles conditioned, increases stamina, and helps with blood circulation. It also puts little strain on ATP production, making it appropriate for people with CFS/ME-induced metabolic disturbances. Walking and swimming are probably the best forms of exercise for this purpose.
A good measure of readiness to exercise is when daily household activities (e.g., sweeping, washing dishes, doing laundry) are no longer a challenge. Once you can function normally in your home, you can begin to walk. The amount of time spent walking can be increased in gradual increments over weeks or months (not days). When you are able to walk for six or seven minutes without feeling short of breath, you can consider gentle stretching, yoga or "weightless" weight training to strengthen specific sets of muscles. (Some CFS/ME patients have had success using weight-lifting equipment set at zero to help tone muscles.)
Once you begin to exercise, it is important to remember that you are not in a contest. How fast you go, how many laps you swim, how many blocks you walk, or how much weight you lift is not only irrelevant, but can be counterproductive. As Dean Anderson, a former ski racer put it, "Most important was learning to enjoy exercise without succumbing to the urge to 'train,' which meant I had to give up on any idea of progressing—of doing more push-ups or of jogging farther or faster . . . Had I set training goals, as healthy people do, I would have invited not only a succession of relapses, but also discouragement and perhaps demoralization" (CFIDS Chronicle, Winter 1996). In other words, learn your limits, which may very well fluctuate from day to day, and stick to them.
PROS AND CONS. As with most treatments, CFS/ME patients respond differently to exercise. But, in this case, the sub-groups sort out rather neatly. Those who are severely ill invariably get much worse from exercise, while those who are mildly ill seem to benefit. The moderately ill group (on a 1 to 10 scale: 5-7) seems to do well with gentle stretching, swimming and walking. While a number of physicians promote the idea that prolonged lack of exercise will worsen CFS/ME by leading to “deconditioning” there is little evidence to support this. In fact, research suggests the opposite.
567
In one of the few longitudinal studies of CFS/ME patients, Matthews and Komaroff found that physical capacity was not only undiminished, but had improved in 99 CFS/ME patients over a 10-year period. There is plenty of anecdotal evidence from CFS/ME patients themselves that even long periods of inactivity do not worsen the illness, and that once recovery is under way the body regains its strength fairly quickly.
SEE: Cardiovascular symptoms
FURTHER READING
General information about CFS/ME and exercise: http://www.cfids.org/archives/2000rr/2000-rr4-article02.asp
Interesting article about responses to exercise in CFS/ME patients. http://www.research1st.com/2011/06/02/exercise-challenge-reveals-potential-cfs-biomarkers/
RESEARCH
Matthews, Rosalind M., Anthony L. Komaroff. “Changes in Functional Status in Chronic Fatigue Syndrome Over a Decade: Do Age and Gender Matter?” Journal of Chronic Fatigue Syndrome, Vol. 14(1) 2007
GET (GRADED EXERCISE THERAPY)
DESCRIPTION. GET is a training program that increases exercise in small increments on a day-to-day basis. It is usually accompanied by CBT (cognitive behavioral therapy), a psychotherapeutic program designed to correct “illness beliefs.”
USES IN CFS/ME. GET was developed in Great Britain as a therapy for CFS/ME. It is based on the idea that CFS/ME is fundamentally a psychological condition that manifests itself as an avoidance of activity. The underlying concept of GET is that maintaining the habit of avoidance perpetuates CFS/ME symptoms.
Needless to say, the GET program has been met with a great deal of criticism. Both patient groups and researchers have pointed out that exercise intolerance is the hallmark symptom of CFS/ME and that a program of systematic exercise will inevitably cause relapse. Researchers who have investigated the mitochondrial defects and resultant cardiac insufficiencies that are common in CFS/ME patients have added that it may, in fact, be dangerous to force severely ill CFS/ME patients into any kind of exercise regime.
The supporters of GET answered this flood of criticism with an extensive randomized trial comparing GET, CBT, Pacing and specialist medical care in 641 CFS/ME patients. Predictably, the PACE trial, as it was called, concluded that GET and CBT could be added to specialized medical care to improve outcomes, but that Pacing (which limits physical activity and requires resting) is not effective.
Almost immediately after the PACE trial publication, the CFIDS Association of America responded with a five-page analysis, in which they pointed out that the
568
cohort selected for the study was skewed. The PACE Group selected their subjects on the basis of the Oxford Criteria for CFS/ME, which only requires six months of fatigue for a diagnosis. This allows for the inclusion of patients with depression and other disorders.
In addition, the CFIDS Association pointed out that the conclusions drawn by the PACE study were biased, not just in the diagnostic criteria used, but on the basis of patients selected. The PACE study excluded severely ill or homebound patients. Nor did it include patients who had been ill longer than six years. In addition, the cohort was relatively young, with a mean age of 38. After a careful analysis, the CFIDS Association concluded that the only concrete result of the study was that a program of graded exercise might be somewhat beneficial to young, moderately or mildly ill patients with non-specific “fatigue” of short duration.
While the heated debate surrounding GET and CBT has most often centered on the basic argument of whether CFS/ME is a biological (American camp) or psychological ailment (British camp), one cannot help but wonder whether the bottom line in the GET debate isn't the bottom line. CBT and GET are cheap to implement. Doubtless, there is strong economic incentive in Great Britain, where medical care comes out of the national budget, for cutting corners on diagnosing CFS/ME (which in the U.S. requires many specialized tests), as well as for treating such a long, costly illness.
PROTOCOL. Typically GET begins with active stretching, followed by range-of-motion contractions and extensions, done for only a few minutes a day for a completely inactive individual. Exercise is increased daily following a schedule until normal activity is resumed.
PROS AND CONS. According to the 2010 treatment survey conducted by the M.E. Association, GET is one of the least successful, if not directly harmful, CFS/ME treatments. While CFS/ME doctors in the U.S. encourage gentle exercise in patients who are well on the road to recovery, they do not endorse graded exercise programs. In addition, most (non-British) studies have concluded that GET has a negative impact on CFS/ME patients. Numerous CFS/ME patients have reported relapses, flares, and a general worsening of symptoms after starting the GET program.
FURTHER READING
Review of GET studies: http://www.mecfsforums.com/wiki/Graded_Exercise_Therapy
“Falling Off the PACE.” An analysis of the PACE trial by the CFIDS Association of America. http://www.cfids.org/pdf/lancet-analysis.pdf
101 Reasons why it is wrong to provide CBT and GET to ME patients. http://niceguidelines.blogspot.com/2011/08/101-reasons-why-it-is-wrong-to-provide.html
RESEARCH
569
Bjørkum T, Wang CE, Waterloo K. [Patients' experience with treatment of chronic fatigue syndrome]. Tidsskr Nor Laegeforen. 2009 Jun 11;129(12):1214-6. http://www.ncbi.nlm.nih.gov/pubmed/19521443 (Abstract)
Núñez M, Fernández-Solà J, Nunez E, Fernandez-Huerta JM, Godás-Sieso T, Gomez-Gil E. “Health-related quality of life in patients with chronic fatigue syndrome: group cognitive behavioural therapy and graded exercise versus usual treatment. A randomised controlled trial with 1 year of follow-up.” Clin Rheumatol. 2011 Mar;30(3):381-9. http://www.ncbi.nlm.nih.gov/pubmed/21234629 (Abstract)
White P D, K A Goldsmith, A L Johnson, L Potts, R Walwyn, J C DeCesare, H L Baber, M Burgess, L V Clark, D L Cox, J Bavinton, B J Angus, G Murphy, M Murphy, H O'Dowd, D Wilks, P McCrone, T Chalder, M Sharpe. “Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): a randomised trial.” The Lancet, Volume 377, Issue 9768, Pages 823 - 836, 5 March 2011 http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(11)60096-2/fulltext
HOMEOPATHY
DESCRIPTION. Homeopathy (from the Greek homeos, similar, and pathos, suffering) is a system of medicine based on the principal that "like cures like"; that is, substances that produce symptoms similar to those manifested by the illness will act as remedies for that illness.
BACKGROUND. The basic principles of homeopathic medicine date from the fourth century BC, when Hippocrates first articulated the idea that a remedy which produces specific symptoms in a healthy person will cure the same symptoms in a sick person. It was not until 1810, however, that homeopathic remedies achieved wide popularity in Europe and America.
In the early part of the nineteenth century a young German physician, Dr. Samuel Hahnemann, discovered that chinchona bark gave him malaria-like symptoms. What surprised him was that chinchona bark was used to treat malaria. Over the years, Dr. Hahnemann experimented with a number of other plant extracts, drugs, and chemicals that produced symptoms of various illnesses. He discovered that minute quantities of these substances served to cure the illnesses whose symptoms they mimicked. Larger quantities of these plants were poisonous, so Hahnemann devised a system of repeated dilutions, or titrations, to preserve effectiveness without injury to the patient.
Homeopathic remedies are so diluted as to leave no perceivable trace of the original plants from which they are derived. The effectiveness of the substance, even in molecular traces, is due to its ability to stimulate the body's natural healing mechanisms along certain specific lines, the symptoms produced by the remedy acting as a set of instructions to the immune system.
An exploratory study performed in Great Britain in 2006 attempted to isolate the active ingredients of homeopathic remedies. The researchers found that about
570
one-third of patients experienced a major improvement in their health over the study period, a third had some improvement and a third had no improvement. However, given the extensive consultations, the in-depth investigation of patient complaints, and the empathy provided by homeopaths themselves, it was impossible to separate the influence of the homeopathic remedies from the positive effects of lengthy consultations with empathetic practitioners.
USES IN CFS/ME. In 2004 a group of researchers from the University of Sheffield in Great Britain studied the effects of homeopathy on a group of 92 CFS/ME patients. The researchers found that homeopathic remedies scored slightly higher than placebo. However, the study used the Oxford Criteria (which defines CFS/ME simply as fatigue lasting for six months) for establishing their patient cohort. As a consequence, the results cannot be considered applicable to the general population of CFS/ME patients.
In a study performed twelve years earlier using the modified Holmes criteria (which includes symptoms other than fatigue), six CFS/ME patients were treated with homeopathic remedies and herbs for three weeks. The researchers found that homeopathy did not affect any of the immunological markers characteristic of CFS/ME patients. The researchers acknowledged that larger studies would be required to verify the effectiveness of herbal and homeopathic remedies, but did not think they were warranted.
PROTOCOL. Classical homeopathic remedies are usually taken either all at once or over a short time. Because they are incompatible with allopathic, or pharmaceutical, remedies, you must make a choice as to which approach you think will work best for you. Homeopathic remedies and drugs cannot be taken at the same time, although they can be taken serially. The decision as to which remedy is best is based on careful, lengthy evaluation of symptoms by a homeopath, who must choose wisely, because in classical homeopathy only a single remedy is prescribed. Often the remedy will provoke a "healing crisis" or worsening of symptoms, after which the homeopath will reassess the situation and recommend a different remedy if necessary.
Although classical homeopathy includes only a limited number of remedies (about 20), "eclectic" homeopathy can make use of hundreds of solutions. Homeopathic blends and remedies for specific problems can also be purchased in health food stores. (Although these tend to be less reliable than consulting a homeopath.) The dosage is usually "as needed" or as indicated on the package. This type of homeopathic remedy may be taken in conjunction with pharmaceutical agents, which is an advantage for patients who must take certain medications on a regular basis. Homeopathic remedies are taken on an empty stomach in pill, liquid, or sublingual form.
PROS AND CONS. Although homeopathic remedies have come under fire by physicians, many CFS/ME patients have found them effective, particularly for treating specific or acute problems such as headache, sinusitis, or insomnia. Homeopathic remedies are generally less expensive (especially single-dose remedies) than drugs and are usually regarded as having fewer side effects.
571
(Homeopaths refer to these remedies as "suggestions" that the body may take or ignore.) The drawback is that classical homeopathy requires patients to discontinue pharmaceuticals. Because many CFS/ME patients rely on pharmaceuticals to manage their symptoms, even a short lapse can make symptoms worse. Consult with a trained homeopath before embarking on this type of therapy.
AVAILABILITY AND COST. Homeopathic remedies range from $6 to $15, although imported remedies (usually German) can cost more. Office visits are comparable to those to a physician and sometimes include the cost of the remedy. As some homeopaths are also M.D.s, insurance may cover the cost of a consultation.
FURTHER READING
Good general guide to homeopathy: http://nccam.nih.gov/health/homeopathy/
A critical, but fair examination of homeopathy: http://www.skepdic.com/homeo.html
RESEARCH
Leyton, Edward and Hugh Pross. “Chronic Fatigue Syndrome Do herbs or homeopathy help?” Can Fam Physician. 1992 September; 38: 2021–2026. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2145466/
Thompson TD, Weiss M. “Homeopathy--what are the active ingredients? An exploratory study using the U.K. Medical Research Council's framework for the evaluation of complex interventions.” BMC Complementary and Alternative Medicine. 2006 Nov 13;6:37. http://www.ncbi.nlm.nih.gov/pubmed/17101037 (Abstract)
Weatherley-Jones E, Nicholl JP, Thomas KJ, Parry GJ, McKendrick MW, Green ST, Stanley PJ, Lynch SP. “A randomised, controlled, triple-blind trial of the efficacy of homeopathic treatment for chronic fatigue syndrome.” J Psychosom Res. 2004 Feb;56(2):189-97. http://www.ncbi.nlm.nih.gov/pubmed/15016577 (Abstract)
HYDROTHERAPY
CAUTION: Some naturopathic physicians use hot water hydrotherapy to artificially create a fever (102 degrees). This form of hydrotherapy is contraindicated in CFS/ME patients. Most CFS/ME patients have some form of dysautonomia, which will only be made worse by exposure to heat. In addition, those patients with upregulated immune systems run the risk of relapse by inducing a fever. Patients with tachycardia or any other cardiac symptoms should avoid all forms of heat exposure as heat places a strain on the heart.
DESCRIPTION. Hydrotherapy is the use of water for healing.
BACKGROUND. The idea of using water to heal the body is not new. For centuries, people have immersed themselves in therapeutic baths as a means to prevent and cure illness. The ancient Romans and the Incas built sumptuous tiled baths, which to this day stand as proofs of the importance these civilizations placed
572
on the restorative powers of water. Healing waters can be found all over the world, from Lourdes in France to the Ganges River in India. Spas and hot springs have long been popular in the United States as well. Saratoga Springs, New York, and Hot Springs, Arkansas, still enjoy a reputation for restoring health and vigor.
Although spas are no longer as popular as they were a century ago, the effects of water on the body should not be underestimated. The human body is, after all, 70% water. Water, in one form or another, supplies most of the nutrients our bodies need to maintain life. Our permeable skin allows substances in mineral-rich water to pass into our bodies. And various water temperatures and pressures can have a profound effect on the way our metabolism and immune system function.
USES IN CFS/ME. Warm-water baths can help reduce pain associated with lactic acid buildup in muscle tissues. This is the pain so often experienced by patients with fibromyalgia symptoms. The water temperature should be at about body temperature. Many people have reported that warm-water baths help loosen tight muscles, reduce leg pains, and in general create a feeling of relaxation.
Immersion in cold water has been beneficial for some patients. One woman reported that a daily 20-minute bath at a very cool 61° F (16° C) helped her feel better overall. The effectiveness of this strategy is most likely due to the fact that the body, when immersed in cold water, automatically shuts down the blood supply to the skin, shunting it instead to vital organs. The additional blood supply to the brain, liver, and other organs affected by CFS/ME could theoretically have a profound impact on reducing symptoms. Dr. Myhill, however, cautions against cold water baths. She theorizes that cold water works because it gives the adrenal glands a huge “kick.” If the adrenal glands are not working properly, as in CFS/ME, then the patient will feel awful. (To avoid the adrenal “kick,” those who wish to try cold water therapy should do so while swimming.)
Both Dr. Paul Cheney and Dr. Charles Lapp have used tepid-water hydrotherapy with good results. Vertical immersion up to the neck in water at about the temperature of a heated swimming pool has reduced symptoms in a number of Dr. Cheney's patients.
The rationale behind this novel form of hydrotherapy is that the increased pressure at the feet forces lymphatic flow to reverse itself, up the body to the thoracic duct (just below the left clavicle), where it is infused into the bloodstream. The presence of the extra lymph tissue signals the immune system that cytokines are already circulating, and the immune system automatically down regulates. In patients experiencing the effects of excess cytokine production, down regulation of immune system chemicals can provide tremendous relief. The increased pressure also forces blood into vital organs.
Whether due to the additional blood supply provided to vital organs or to down regulation of the immune system, this form of hydrotherapy may offer considerable benefits to a number of people with CFS/ME.
PROTOCOL. Dr. Cheney's hydrotherapy protocol requires almost complete immersion in water at 80° to 86° F (swimming pool temperature). For the process to work, it is important that the patient remain vertical and immersed up to the neck,
573
which means a flotation device is necessary. Initially, immersion time is fifteen minutes, increasing slowly to a half hour. The entire treatment plan calls for 16 weeks of hydrotherapy, with three sessions per week.
PROS AND CONS. Dr. Cheney's hydrotherapy program may be a particularly good treatment option for people with pain because it appears to have a positive effect in relieving fibromyalgia symptoms. It seems to have minimal side effects, although some severely ill patients have experienced temporary worsening or relapse of symptoms, no doubt due to the increased concentration of cytokines in the bloodstream. These symptoms decrease over time. Patients who stopped treatment before the 16-week period have had relapses. Once you embark on this treatment, you are committed to finish it. Another problem that could occur is chilling. Dr. Cheney recommends that if you start to shiver, get out of the pool, but do not take a hot shower. If necessary, purchase a wetsuit to help maintain body heat.
AVAILABILITY AND COST. Most forms of hydrotherapy are not expensive. A membership to a facility with a pool (such as a club or a community center) may be necessary to follow Dr. Cheney's hydrotherapy program, however. For his program, you will also need to purchase a flotation device to rest on while you are in the water.
For those who do not have access to a pool, Dr. Lapp finds that a bathtub may be equally effective.
HYPNOSIS
DESCRIPTION. Hypnosis involves inducing a trance-like state, somewhere between sleep and wakefulness, to produce greater suggestibility in a patient.
BACKGROUND. Although the technique of producing physiological and psychological effects by means of deep trances has been used by yogis, mystics, and oracles since earliest times, it was not until the eighteenth century that Europeans regarded the hypnotic trance as useful for medical purposes.
In the 1760s, Franz Anton Mesmer popularized hypnosis in Europe via a series of theatrical demonstrations of what he called "animal magnetism." Mesmer believed that illness was the direct result of an imbalance in animal magnetism and that hypnosis could correct these imbalances. Because Mesmer's subjects did rather silly things while "mesmerized," hypnosis initially acquired the reputation as a form of entertainment rather than as a therapy.
The current practice of hypnosis has discounted Mesmer's theory of animal magnetism and eliminated the theatrical aspects of hypnosis in order to provide a unique means of influencing normally inaccessible physiological functions, namely those controlled by the autonomic nervous system. By accessing the body's ability to produce heat, dilate or constrict blood vessels, speed or slow metabolism, and so forth, the hypnotist can utilize the body's own mechanisms to control pain, reduce anxiety, relieve phobias, and cure addictions.
USES IN CFS/ME. Hypnosis can be beneficial in reducing the effects of anxiety and stress brought on by illness. It can also help alleviate headaches, pain,
574
insomnia, and some cognitive problems. Most people with CFS/ME describe hypnosis as "very relaxing."
PROTOCOL. A standard visit to a hypnotist involves evaluation of a particular problem (e.g., insomnia, pain, anxiety). After assessing the problem, the hypnotist will ask you to sit back in a reclining chair and focus your eyes on a point on the ceiling or a light while he or she speaks to you in a low, monotonous voice. After a short time, your body will relax, and the hypnotist will suggest that you close your eyes. While your eyes are closed, the hypnotist will read from a script specifically designed for your particular problem. After listening, you will be asked to open your eyes on the count of ten and come back to the office setting. The hypnotist may ask you what you felt or "saw." The visit usually lasts one hour.
AVAILABILITY AND COST. Licensed hypnotists generally charge $50 - $95 per hour session, depending on their degree of training. Hypnotherapists holding an advanced degree in psychology may charge more.
FURTHER READING
This site provides a hypnotherapy script for CFS/ME. http://www.brooksidecenter.com/hypnosis_and_chronic_fatigue_syn.htm
MASSAGE
Craniosacral Massage, Lymphatic Drainage, Myofascial Release, Perrin Technique, Reflexology, Shiatsu
CAUTION: Vigorous massage is contraindicated in patients with osteoporosis, hypertension, inflammation, arthritis, varicose veins, thrombosis, aneurysm, skin, muscle, or bone disease, unhealed bone fracture, torn ligaments, tendons, or muscles, diabetes, tumors, frostbite, and in pregnant women.
DESCRIPTION. Massage therapy involves manipulation of soft tissue by rubbing, stroking, kneading, compressing, or vibration.
BACKGROUND. Massage techniques are as old and as varied as the cultures that originally devised them. As a consequence, it is almost impossible to make a general description of massage therapy. Some techniques, such as Swedish massage, are vigorous and cover the entire body. Others, such as shiatsu, apply pressure to specific areas.
All massage techniques share the principle that the body can be healed through mechanical means. Massaging the body can produce profound metabolic changes. A vigorous massage stimulates the sympathetic nervous system, which speeds up the metabolism, increasing blood circulation, heart rate, respiration, and surface temperature. A light massage, especially over the lower back, stimulates the parasympathetic nervous system, decreasing heart rate and blood pressure and increasing digestive action. Any relaxation of muscle knots and spasms enhances the ability of the vascular system to cleanse the lymphatic system and to clear
575
stagnant tissue fluid, toxins, and the excess lactic acid buildup that causes acidosis and muscle pain.
USES IN CFS/ME. Most CFS/ME patients use massage to relieve muscle pain, headaches, and muscle spasms. A number of patients have reported that a firm massage of the soles of the feet has a profound beneficial effect throughout the body.
PROS AND CONS. While it may seem like the logical therapy for pain, a vigorous massage can paradoxically make pain worse. The reason for the aggravation of pain is probably due to the practice of placing excessive pressure on nerve endings to relieve knotty muscles. Nerve compression only exacerbates the pain created by an already irritated nervous system. Vigorous massage will also release accumulated toxins into the system. According to Dr. Cheney, this may lead to malaise in CFS/ME. On the other hand, gentle massage is often beneficial. Those who want to try massage to treat chronic or severe pain may want to consider starting with some of the gentler techniques.
AVAILABILITY AND COST. Massages generally cost $40 to $60 per hour. If performed by a licensed physical therapist, the cost of massage may be covered by insurance (usually a physician's referral is required).
CRANIOSACRAL MASSAGE
Craniosacral massage (also called cranial osteopathy) is a gentle form of massage focusing on the spinal cord and skull. It was developed in the 1970s by an American osteopath, John Upledger, who noticed that spinal fluid made rhythmic pulsations as it traveled up the spinal column. He speculated that alterations in the pulses could be used for diagnosis and devised a system by which illnesses could be treated by subtle readjustments. Craniosacral massage is used to treat head injuries, migraines, balance disorders, hyperactivity, whiplash, ear and eye problems, fibromyalgia, and temporomandibular joint (TMJ) syndrome.
Although there have not been any studies confirming the clinical efficacy of craniosacral massage, it continues to be employed by CFS/ME and fibromyalgia patients for temporary relief of pain.
FURTHER READING
Website of the Craniosacral Therapy Association (U.K.): http://www.craniosacral.co.uk/
Website of the Biodynamic Craniosacral Therapy Association of North America. http://www.craniosacraltherapy.org/CSTA_home.html
Craniosacral Therapy: http://www.beatcfs.info/osteopathy.html
Hartman, Steve E. and James M. Norton. “Interexaminer Reliability and Cranial Osteopath.” Sci Rev Alt Med 6 (1): 23–34. 2002. http://faculty.une.edu/com/shartman/sram.pdf
LYMPHATIC DRAINAGE
576
The Vodder method of manual lymphatic drainage is a gentle, rhythmic European massage technique designed to increase and accelerate the movement of lymphatic fluid through the body. It was developed in France in the 1930s to treat a variety of conditions that might be caused or aggravated by congested lymph, including sinusitis, acne, edema, inflammation, and arthritis.
Lymphatic drainage uses several techniques. In the first, light circular motions are directed towards the heart to facilitate the return of the lymph to the circulatory system. Therapists may also focus on the face and neck, using the same circular motions. In the “pump technique” the therapist presses the back of the client while moving the fingers and thumbs in slight oval movements towards the heart. At the end of the session, a twisting motion is used to “wring out” the client’s lymph nodes. According to practitioners, when the massage is complete, clients should feel relaxed, with decreased swelling in the lymph nodes.
FURTHER READING
Lymphatic drainage techniques: http://www.mesupport.co.uk/index.php?page=lymph-drainage-massage
General information about lymphatic drainage. http://www.healthguidance.org/entry/11584/1/Lymphatic-Drainage-Massage.html
Worldwide directory of lymphatic drainage specialists: http://www.vodderschool.com/find_a_therapist
MYOFASCIAL RELEASE
DESCRIPTION. Myofascial release is a form of massage that involves exerting sustained pressure. It was originally designed by Andrew Taylor Still, the founder of osteopathy. The basis of osteopathic medicine is that the body is a self-regulating unit with the power to heal itself. Traditional osteopathic techniques involve manipulation of fascia (soft tissue) in order to reduce pain, increase lymphatic drainage, and improve blood flow.
There are two methods of myofascial release. In direct myofascial release practitioners use their knuckles, elbows, or other tools to exert a strong pressure that slowly stretches the restricted soft tissue. The practitioner moves slowly through the layers of soft tissue until the deep tissues are reached.
Indirect myofascial release utilizes a gentle pressure, which allows the fascia to simply “unwind” without causing undue stress on the tissue. The indirect method involves lightly contacting the fascia and slowly stretching the fascia for approximately three to five minutes. The slow stretching results in an increase of blood flow to the affected area, which, in turn, reduces pain.
USES IN CFS/ME. In 2011 a study was conducted on myofascial release for the treatment of fibromyalgia. The researchers found that “immediately after treatment and at 1 month, anxiety levels, quality of sleep, pain, and quality of life were improved in the experimental group over the placebo group.” However, the results were not sustained six months after the cessation of treatment, which
577
suggests that myofascial release, like other forms of massage, provides benefits only in the short term.
FURTHER READING
John Barnes' website for myofascial release. Includes directory of practitioners. http://www.myofascialrelease.com/fascia_massage/public/whatis_myofascial_release.asp
Directory of myofacial release practitioners: http://www.advanced-trainings.com/directory.html
Castro-Sánchez, A.M., Matarán-Peñarrocha, G.A., Granero-Molina, J., Aguilera- Manrique, G., Quesada-Rubio, J.M., Moreno-Lorenzo, C. “Benefits of massage-myofascial release therapy on pain, anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia.” Evid Based Complement Alternat Med. 2011;2011:561753. http://www.ncbi.nlm.nih.gov/pubmed/21234327 (Abstract)
PERRIN TECHNIQUE
The Perrin Technique is a form of lymphatic massage that is practiced in Great Britain, and, to a limited extant, in Europe. It was developed exclusively for treating CFS/ME by Dr. Raymond Perrin, a British osteopath.
According to Dr. Perrin, people with CFS/ME suffer from a build-up of toxins in the fluid around the brain and spinal cord. CFS/ME symptoms are the result of the congestion of these toxins. In the Perrin Technique, the spine is manipulated so that soft tissues in the head, neck, back and chest can direct the toxins out of the lymphatic system and into the blood, where they are eventually detoxified in the liver. Dr. Perrin states that “with no poisons affecting the brain, the sympathetic nervous system begins to function correctly, and providing the patients do not overstrain themselves their symptoms should gradually improve and in time some patients become totally symptom free.”
While claims that the Perrin Technique can actually cure CFS/ME are exaggerated, about 50% of the respondents to the 2010 ME treatment survey in Great Britain reported that the Perrin Technique provided them with some improvement. The other half reported no change or a worsening of symptoms.
FURTHER READING
Website of the Perrin clinic: http://www.theperrinclinic.com/
Patient thread on the Perrin Technique: http://forums.phoenixrising.me/showthread.php?8526-Perrin-lymph-drainage-massage-makes-sense-or-not
Another patient thread on the Perrin Technique: http://forums.phoenixrising.me/showthread.php?11258-The-Perrin-Technique-Does-it-help
Perrin, Raymond N., DO. “Lymphatic Drainage of the Neuraxis in Chronic Fatigue Syndrome: A Hypothetical Model for the Cranial Rhythmic Impulse.” Journal of
578
the American Osteopathic Association. 2007 http://www.jaoa.org/content/107/6/218.full
REFLEXOLOGY
Although foot massage has been practiced for centuries, it wasn't until the early 20th century that it was introduced in the United States as a medical treatment. In 1913 William Fitzgerald, an ear, nose and throat specialist, found that applying pressure on one part of the body produced an anesthetic effect on other areas of the body. In the 1930s, Eunice D. Ingham (1889–1974), a nurse and physiotherapist, expanded on Fitzgerald's observation, identifying the feet and hands as especially sensitive. Ingham then mapped the entire body, identifying corresponding zones on the feet.
Modern reflexology is based Ingham's idea that reflex points (or zones) located on the hands and feet correspond to every organ in the body. Steady, even pressure applied by the fingers to these zones is said to remedy any imbalances in the corresponding organs. Reflexology is supposed to promote improved circulation and contribute to a sense of relaxation and well-being. Because reflexology may be practiced easily on one's own feet and hands, it is an ideal form of self-massage
Several studies have shown that reflexology may be beneficial for some conditions. In 2010 a group of Japanese researchers found that reflexology improved cold intolerance. A 2009 Korean study found that self-administered reflexology improved fatigue, stress and blood circulation.
While there are no systematic scientific studies confirming the efficacy of reflexology in treating any specific medical condition, it remains a very popular form of massage.
FURTHER READING
Ernst E. “Is reflexology an effective intervention? A systematic review of randomised controlled trials.” Med J Aust. 2009 Sep 7;191(5):263-6. http://www.ncbi.nlm.nih.gov/pubmed/19740047 (Abstract)
Jang SH, Kim KH. [Effects of self-foot reflexology on stress, fatigue and blood circulation in premenopausal middle-aged women]. J Korean Acad Nurs. 2009 Oct;39(5):662-72. http://www.ncbi.nlm.nih.gov/pubmed/19901496
Zhang W, Takahashi S, Miki T, Fujieda H, Ishida T. "A pilot study exploring the effects of reflexology on cold intolerance.” J Acupunct Meridian Stud. 2010 Mar;3(1):43-8. http://www.ncbi.nlm.nih.gov/pubmed/20633515 (Abstract)
SHIATSU
Shiatsu is an ancient form of Japanese massage closely related to acupuncture that dates to the third millennium BC. The basic technique consists of the application of pressure by the fingers over some 600 neural trigger points located on lines (meridians) throughout the body. The points are said to be places where lymph vessels tend to congregate. By releasing the point with gentle
579
sustained pressure, energy blocks are removed and the body can better eliminate waste products such as lactic acid that have accumulated in body tissues.
In Japan, where Shiatsu is recognized as a formal branch of medicine, Shiatsu practitioners must undergo a three-year course of training and be licensed with the Ministry of Health and Welfare. Western nations, because they do not recognize Shiatsu as a medical treatment, do not require a license. Nevertheless, Shiatsu is an established form of massage not just in Asia, but in most Western countries.
In 2011 a meta-analysis of 1714 publications regarding acupressure and shiatsu was conducted by members of the Allied Health Sciences Department of London South Bank University. While there was evidence supporting acupressure's efficacy in moderating pain, nausea, and insomnia, the investigators found that research of Shiatsu was too scant to come to an overall conclusion.
As with other forms of gentle massage, CFS/ME patients report that Shiatsu is helpful with managing pain.
FURTHER READING
General discussion of Shiatsu in CFS/ME: http://www.beatcfs.info/shiatsu.html
Robinson N, Lorenc A, Liao X. “The evidence for Shiatsu: a systematic review of Shiatsu and acupressure.” BMC Complement Altern Med. 2011 Oct 7;11:88. http://www.ncbi.nlm.nih.gov/pubmed/21982157 (Abstract)
MEDITATION/AMYDALA RETRAINING PROGRAM
DESCRIPTION. In meditation, a calm state of consciousness is achieved by means of concentration, contemplation, or visualization techniques.
BACKGROUND. Meditation is an ancient practice that has been used throughout the ages to reach an inner state of quiet. Meditation techniques form the backbone of Buddhism, one of the world's major religions. Because meditation was, and still is, practiced to achieve an altered or "higher" state of consciousness (a drawing closer to a divine state of being), the practice of meditating is less a therapy than a way of life.
Meditation is as much a mode of looking at the world as it is a technique, as much a philosophy as a practice. In meditation, the means and the ends are as one. One meditates for its own sake, not to achieve a specific goal but to let go of all goals. In the process of letting go, a different person emerges. A different body may emerge, as well. Those who meditate have been known to achieve lowered blood pressure, relief from pain and migraine headaches, and greater mental clarity and alertness through the simple act of gazing within.
USES IN CFS/ME. In the 2010 M.E. Association's survey of treatment modalities, nearly 54% of respondents indicated that meditation and relaxation techniques were helpful. Those who meditate on a regular basis report an increased feeling of calm and improved outlook on life. Meditation is also effective in controlling the pain generated by an over-reactive nervous system. Like rest, meditation seems to cause no damage and results only in a general sense of
580
improvement. Patients with CFS/ME, especially those who find themselves plagued by depression, anxiety, fear, and anger, can benefit greatly by the practice and philosophy of "letting go."
PROS AND CONS. There is no "right" way to meditate, but some practitioners may try to convince you there is. Of the many meditative traditions, not all are conducive to healing long-term illnesses. Zen, for example, was developed for healthy, young, Japanese monks. Sitting for several hours staring at a blank wall (and getting roused by a sharp rap on the head when you drift off to sleep) is perhaps not the best meditation technique for ill people. When you begin to meditate, especially if you are quite ill, do it your own way. Lie down in the comfort of your own bed, and listen to your favorite relaxing music. Then breathe. Remember, meditation is a state of mind. How you get there is up to you.
AVAILABILITY AND COST. You can meditate at home for free or you can join a meditation group. Classes in meditation and yoga centers are not usually expensive. You can teach yourself to meditate easily and painlessly by listening to various CDs made for that purpose or by reading a book on meditation techniques. There are many videos of guided meditations posted on youtube.
FURTHER READING
For those who wish to understand the philosophy of meditation, anything written by Thich Nhat Hanh will be helpful.
The Mayo Clinic's excellent overview of meditation and its benefits. http://www.mayoclinic.com/health/meditation/HQ01070
Margaret Fergusson's personal account of her recovery from CFS/ME (in which meditation played a prominent role): http://www.cfidsselfhelp.org/library/physical-and-psychological-recovery-cfs
“Meditation and the Course of Chronic Fatigue Syndrome.” William Collinge. http://www.collinge.org/Fri.htm
Living with CFS/ME. “Meditation for Peace of Mind.” CFIDS Chronicle, Summer 2000. http://www.cfids.org/archives/2000/2000-3-article09.asp
Phoenix Rising page on meditation: http://phoenixrising.me/treatments-3/treating-chronic-fatigue-syndrome-mecfs-meditation
AMYGDALA RETRAINING PROGRAM
The Amygdala Retraining Program (ARP) is a combination of meditation, visualization and self-guided therapy techniques developed by Ashok Gupta. Gupta's theory is that CFS/ME is caused by trauma to the amygdala, which is the part of the limbic system most closely associated with learning and fear responses.
According to Gupta, during the acute physical stage of the illness, the amygdala “learns” to be hyper-reactive to any symptoms detected in the body. Once the amygdala become hyper-reactive, it overstimulates the sympathetic nervous system, the hypothalamus, the HPA axis, and the immune system, creating the cascade of symptoms experienced by people with CFS/ME.
581
Ashok Gupta makes the claim that his program is the first world-wide “100% cure for CFS/ME,” which automatically rouses suspicions in most people with the illness. (If there really were a 100% cure out there, you would not be reading this book.) However, many of the methods Gupta employs are based on time-honored meditation techniques. These include halting circular thoughts (which are a sign that the brain is in overdrive), visualizing well-being, breathing exercises, and mindfulness meditation. During the ARP, these techniques are practiced for 30 minutes a day. The entire program takes six months.
The Amygdala Retraining Program is available through Ashok Gupta's clinics in Great Britain and from ARP coaches in France, Germany and Israel. A set of 12 DVDs that will guide you through the program can be purchased for $200 (U.S.) with a full money-back guarantee.
FURTHER READING
ProHealth interview with Ashok Gupta, in which he explains his theory and describes how his program works: http://www.prohealth.com/library/showarticle.cfm?libid=14508
Cort Johnson's interview with Ashok Gupta about controlling the stress response. http://phoenixrising.me/archives/495
Amygdala Retraining from a psychologist's perspective. http://alwayswellwithin.com/2010/05/11/retraining-the-brain-for-cfs-fms-mcs-ptsd-gws/
Detailed critique of Gupta's hypothesis: http://forums.phoenixrising.me/showthread.php?4191-Amygdala-retraining-fact-from-fiction
Informative discussion of the amygdala and fear responses: http://serendip.brynmawr.edu/exchange/node/1749
Ashok Gupta's website: http://www.guptaprogramme.com/default.asp
PACING
DESCRIPTION. Pacing is a system in which CFS/ME patients learn to stay within their limits.
USES IN CFS/ME. At first glance, pacing is no more than the exercise of common sense. It was developed as an extension of the advice CFS/ME doctors usually give their patients: Don't push it. Although this may seem logical, many moderately or recently ill CFS/ME patients are deceived by the waxing and waning pattern of their symptoms. As a consequence, they attempt to resume “life as usual” long before they have recovered. These efforts are almost always followed by a crash. Pacing is merely the formalized means by which a patient learns to find his or her limits.
PROTOCOL. There are three basic tenets of pacing: 1) stay within your envelope – only do 70% of what you think you can do, 2) schedule rest times – even on “good days” lie down for at least 15 minutes, at least twice a day, 3) keep a diary of symptoms – if they follow a pattern (and sometimes they do!), plan your activities
582
accordingly. For example, if you find that you “crash” in the afternoon (many people with CFS/ME slump at that time), schedule meetings, shopping, etc. for the morning. Do one important errand, not four minor ones. If you are doing a task at home, don't try to finish before you lie down. Take breaks and rest frequently during work time. Last of all, procrastinate – never do today what you can put off for tomorrow.
FURTHER READING
A patient discusses how she uses Pacing to manage CFS/ME. http://www.cfidsselfhelp.org/library/how-i-use-pacing-manage-cfs
TENS
DESCRIPTION. TENS (transcutaneous electrical nerve stimulation) is the topical application of an electrical stimulus to a peripheral nerve in order to control pain.
BACKGROUND. The TENS machine was developed after the "gate" model of pain was developed. Pain researchers believed that when nerves are overstimulated, the pain message stops (the assumption being that the brain cannot process sensory input from so many "gates"). The stimulation from TENS is supposed to "drown out" the pain felt in a nerve. Some have also proposed that the reason TENS works is not because the nerve is overstimulated but because the electrical stimulation prompts the release of pain-killing endorphins. Whether the relief is through nerve overstimulation or chemistry, the result is the same—pain is relieved.
Several studies have found that TENS is useful for treating pain in post-operative patients, for arthritis, and chronic back pain. An equal number have not found evidence of efficacy beyond placebo. What needs to remembered is that pain is a purely subjective experience; it cannot be measured by any objective means (e.g., blood tests, CT scans). Moreover, people have varying pain thresholds; what is painful for one person, may not be for the next. This makes it difficult to measure the effectiveness of any pain treatment.
USES IN CFS/ME. TENS has been recommended for patients with fibromyalgia pain, that is, pain generated by trigger points and nerve irritation.
PROTOCOL. The TENS unit is a small machine that generates electrical current which is conveyed along wires to small rubber-tipped electrodes. The unit can be worn on a belt. The electrodes are placed on specific sites on the skin by a physician or physical therapist and are held in place with adhesive tape. The amount of stimulation is regulated by the physician.
PROS AND CONS. TENS is nonaddictive, has no damaging side effects, and, in many cases, is an effective form of pain control. However, it does require a visit to the physician's office and can be expensive if many treatments are required.
AVAILABILITY AND COST. TENS units are expensive to purchase ($650), and rental can cost $50 a month. Inexpensive home units are available for much less, but may not have the capacity of larger units. However, it is best to receive
583
TENS treatments in the office of a health care practitioner who monitor the level of stimulation. The cost of treatment varies, depending on the supervising clinician. When TENS is ordered by a physician, insurance may cover the cost.
FURTHER READING
Detailed explanation of how TENS works: http://www.patient.co.uk/health/TENS-Machines.htm
Bjordal JM, Johnson MI, Ljunggreen AE. “Transcutaneous electrical nerve stimulation (TENS) can reduce postoperative analgesic consumption. A meta-analysis with assessment of optimal treatment parameters for postoperative pain.” Eur J Pain. 2003;7(2):181-8. http://www.ncbi.nlm.nih.gov/pubmed/12600800 (Abstract)
VISUALIZATION AND IMAGERY
DESCRIPTION. Visualization (guided imagery, creative visualization, creative imagery, or mental imagery) is the use of mental images to produce changes in the body.
BACKGROUND. The use of imagery for healing first drew attention in the 1950s when a cancer patient went into remission after visualizing the disappearance of a tumor. This case fueled a great deal of interest in the medical community and eventually led to the development of visualization techniques geared specifically to certain diseases. While visualization has enjoyed a reputation as a "miracle cure," it should be remembered that spontaneous remissions are possible with any illness. Those who question the curative powers of visualization point out that its healing powers are coincidental at best. Despite its limitations, visualization can serve as a useful coping technique.
Visualization is thought to work by mobilizing the immune system, which is not normally under conscious control, through the efforts of higher brain functions. The act of voluntarily creating images (as opposed to hallucinations or dreams) is controlled by the cortex, whereas the immune system is regulated, at least in part, by structures in and around the limbic system, notably the hypothalamus. Since the nerve fibers that connect the limbic system to the cortex flow through the hypothalamus, allowing for a two-way interchange between thought and autonomic nervous system and, hypothetically, immune system function, it is argued that thought can also direct the outcome of illness.
USES IN CFS/ME. Visualization techniques can be helpful in maintaining a sense of calm. This can be useful for patients who are severely ill or are experiencing a relapse. Some have reported that, much like hypnosis and meditation, visualization helps them control pain and anxiety.
PROTOCOL. To visualize, you must begin by relaxing. Get comfortable, take three or four deep breaths (if you practice meditation or self-hypnosis, you can use any of those techniques), and concentrate on the desired images. For CFS/ME, images that have been suggested include the following:
584
Imagine you are surrounded by a bubble of pink light through which nothing can pass. You are completely protected.
Breathe in light through the crown of the head. Feel that the light's energy is going through every cell and every tissue, bringing feelings of love and well-being to every part of your body.
See the light perfectly balancing your immune system and restoring it to the way nature intended.
If "seeing" does not work for you, try kinetic imagery. Kinetic, or motion, imagery techniques are more primal than techniques that rely on vision alone. As a consequence, they may be more useful to patients who are acutely ill or cannot make a visual image. Some patients have imagined they are gently rocking in a boat, floating down a stream, or traveling around a sideways figure of eight. These movement-oriented images are useful to alleviate headaches, panic, vertigo, and episodes of nonlocalized pain.
PROS AND CONS. Visualization is inexpensive – all you need is a book to explain the theory and you can invent your own images – and it may help you feel more in control. Visualization, however, does not seem to work against the disease process itself. Patients who are led to believe that skillful use of imagery will rid them of all their ills are invariably disappointed. However, if your goal is short-term alleviation of pain, anxiety, or stress-related symptoms, guided imagery, like hypnosis or meditation, can serve a purpose.
FURTHER READING
Bruce Campbell's relaxation and visualization techniques: http://www.cfidsselfhelp.org/library/stress-reduction-five-practical-techniques
BOOK
Collinge, William. Recovering From Chronic Fatigue Syndrome. New York: The Body Press/Perigee Books, 1993.
Includes many guided imagery techniques.
Download as complete pdf