Skill Level 5
Relevance:5 Technical Level:3
Page Synopsis: CFS has been described as brain injury, and TBI can lead to CFS. I will have to get full proper testing to find out
page 50 PTBICF
page 49
page 51
pTBIcf is an acronym for post Traumatic Brain Injury Chronic Fatigue
Fatigue After Brain Injury: Why It Occurs and How to Overcome It https://www.flintrehab.com/fatigue-after-brain-injury
Fatigue is one of the most long-lasting and common effects of brain injury. In fact, up to 73% of individuals report fatigue up to 5 years after sustaining their injury.
Various factors can contribute to increased fatigue after TBI. One reason fatigue is so prevalent is because in the early phases following a TBI, the brain focuses most of its energy on healing. While this is essential for stabilizing the brain after injury, it also leaves less energy to be devoted to other tasks.
Another explanation is the coping hypothesis, which suggests that individuals are more likely to experience fatigue after brain injury because the brain must work harder to compensate for impaired functions.
Moreover, feelings of fatigue may not be directly related to brain injury at all. Instead, they can stem from secondary effects of TBI, such as depression, pain, poor-quality sleep, and endocrine dysfunction.
In the following section, we’ll discuss different types of fatigue that an individual may experience after brain injury.
Types of Fatigue That Can Occur After Brain Injury
Everyone experiences the effects of TBI differently. Fatigue may be more severe for some than for others; however, fatigue is not correlated to the severity of TBI. In other words, fatigue is just as common in individuals with mild TBIs as in those with severe TBIs.
It’s important to understand what type of fatigue you’re experiencing to target your specific symptoms and effectively treat them.
There are 3 primary types of fatigue that an individual may experience after brain injury:
Physical fatigue. With this type of fatigue, you feel exhausted after participating in any sort of physical activity. Even the simplest tasks can cause feelings of exhaustion. It usually is most severe in the evening but gets better after you sleep.
Cognitive fatigue. With this type of fatigue, it is challenging to concentrate. For example, you may find that reading a book or trying to listen to someone talk wears you out quickly. As with physical fatigue, mental fatigue is usually worse at the end of the day.
Psychological fatigue. This type of fatigue shares many of the same symptoms as physical and mental fatigue; however, it does not get better after rest.
The type of fatigue you experience after a brain injury will primarily depend on which areas of the brain are affected as well as the types of secondary complications you experience. While it is possible to experience all three types of fatigue after brain injury, most individuals experience cognitive fatigue
Excessive daytime sleepiness (EDS) in OSA is associated with significant changes to the brain
Obstructive sleep apnea (OSA) is associated with reduced gray matter concentration"
Imaging studies in patients with severe OSA showed reduced gray matter concentration in certain brain regions compared with healthy volunteers, including the frontal cortex, anterior cingulate cortex, and thalamus
Excellent article Best Nootropics for Traumatic Brain Injury as PDF, viewed on page 9 or https://nootropicsexpert.com/best-nootropics-for-traumatic-brain-injury

Effort and Fatigue-Related Functional Connectivity in Mild Traumatic Brain Injury
https://www.frontiersin.org/articles/10.3389/fneur.2018.01165/full
Understanding the interplay between mild traumatic brain injury and cognitive fatigue: models and treatments
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6122693
Factors contributing to chronic fatigue after traumatic brain injury
https://pubmed.ncbi.nlm.nih.gov/22190008
Chronic hypopituitarism after traumatic brain injury: risk assessment and relationship to outcome
https://pubmed.ncbi.nlm.nih.gov/18580806
Fatigue and traumatic brain injury https://pubmed.ncbi.nlm.nih.gov/16716438 'Rapid correction
of serum 25-OHD levels can be easily achieved with oral administration of high-dose cholecalciferol'
Injury of the Ascending Reticular Activating System in Patients With Fatigue and Hypersomnia Following Mild Traumatic Brain InjuryInjury of the Ascending Reticular Activating System in Patients With Fatigue and Hypersomnia Following Mild Traumatic Brain Injuryhttps://pubmed.ncbi.nlm.nih.gov/26871783 In conclusion, this study demonstrated injuries of the dorsal and ventral lower portions of the ARAS in patients with fatigue and hypersomnia following mild TBI. We believe that these injuries of the ARAS might be a pathogenetic mechanism of fatigue and hypersomnia in patients with TBI. Conduct of further studies on this topic should be encouraged . We report on patients with posttraumatic fatigue and hypersomnia who showed injury of the lower portion of the ascending reticular activating system (ARAS) between the pontine reticular formation (RF) and the intralaminar thalamic nucleus (ILN) following mild traumatic brain injury (TBI), using diffusion tensor tractography (DTT). Two patients with mild TBI resulting from a car accident were enrolled in this study. Patient 1 was a 51yearold woman showed abnormalities as 6.9 (cut off: 3.7 points) and 18 (cut off: 10) on the Fatigue Severity Scale and the Epworth Sleepiness Scale at 11 months after onset. Patient 2 was a 64yearold woman who revealed abnormalities on the Fatigue Severity Scale and the Epworth Sleepiness Scale with 6.8 and 19 at 3 months after onset. In both patients, the upper ARAS in which the neural connectivity of the ILN to the cerebral cortex did not show significant abnormalities. However, we observed the narrowing of the left dorsal lower ARAS between the pontine RF and the ILN in both patients and the tearing (patient 1) and narrowing (patient 2) of the left ventral lower ARAS between the pontine RF and the hypothalamus. Injuries of the dorsal and ventral lower ARAS were demonstrated in patients with fatigue and hypersomnia following mild TBI. We believe that these injuries of the ARAS might be a pathogenetic mechanism of fatigue and hypersomnia in patients with TBI. INTRODUCTION Before the introduction of diffusion tensor imaging (DTI), accurate evaluation of the ascending reticular activating system (ARAS) in the live human brain was limited. Recently, diffusion tensor tractography (DTT), which is derived from DTI, has enabled 3dimensional reconstruction and estimation of the ARAS in the human brain.1–4 As a result, a few recent studies using DTT have reported on injury of the ARAS in patients with severe traumatic brain injury (TBI).5,6However, no study on injury of the ARAS in patients with mild TBI has been reported. Posttraumatic fatigue and hypersomnia are common sequelae following TBI.7–9 Previous studies have reported close association between fatigue and sleepiness in patients with TBI.7,8 The pathogenetic mechanism of posttraumatic fatigue and hypersomnia has not been clearly elucidated, although several studies have suggested an injury of the brainstem or ARAS.9–11 In the present study, using DTT, we report on patients with posttraumatic fatigue and hypersomnia who showed injury of the dorsal (between the pontine reticular formation [RF] and the intralaminar thalamic nucleus [ILN]) and ventral (between the pontine RF and the hypothalamus) lower portion of the ARAS following mild TBI. CASE REPORT Subjects Two patients were enrolled according to the following inclusion criteria: (1) loss of consciousness (LOC) for 30 min or less, posttraumatic amnesia (PTA) for <24 h and Glasgow Coma Scale (GCS) score of 13 to 15 recorded 30 min postinjury or later upon presentation for health care,12 (2) notify hypersomnia and fatigue since the onset of TBI, (3) no visible lesion on T1weighted, T2weighted, fluid attenuated inversion recovery, and T2weighted gradient recall echo images, and (4) no history of previous head trauma. All patients provided signed, informed consent, and Yeungnam University hospital Institutional Review Board approved the study protocol. Patient 1 was a 51yearold woman who had suffered head trauma resulting from a car accident. While driving her sedan, the driver side of her car collided with a minibus; consequently, her head hit the car seat. The patient showed LOC (5 min) or PTA (10 min) at the time of head trauma, and her GCS was 15 when she arrived at the hospital. At the time of DTI scanning (11 months after onset), she showed abnormalities as 6.9 (cut off: 3.7 points) and 18 (cut off: 10), respectively, on the Fatigue Severity Scale and the Epworth Sleepiness Scale.13–16 Patient 2 was a 64yearold woman who had suffered head trauma resulting from a car accident. While driving in a passenger seat of a sedan, her car was hit from front by a sedan. As a result, her head hit the steering wheel. The patient experienced LOC for ∼5 min without PTA. Her GCS score was 15 when she arrived at the hospital. At the time of DTI scanning (3 months after onset), she showed abnormalities on the Fatigue Severity Scale and the Epworth Sleepiness Scale with 6.8 (cut off: 3.7 points) and 19 (cut off: 10), respectively.13–16 Diffusion Tensor Imaging Diffusion tensor imaging data were acquired at 11 months (patient 1) and 3 months (patient 2) after onset of head trauma using a 1.5 T with 32 noncollinear diffusion sensitizing gradients by singleshot echoplanar imaging. Imaging parameters were as follows: acquisition matrix = 96 × 96; reconstructed to matrix = 192 × 192; field of view = 240 × 240 mm2; TR = 10,398 ms; TE = 72 ms; parallel imaging reduction factor = 2; echoplanar imaging factor = 59; b = 1000 s/mm2; and a slice thickness of 2.5 mm. The Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library was used for analysis of DTI data. Eddy current correction was applied to correct the head motion effect and image distortion. FMRIB Diffusion Software with routines option (0.5 mm step lengths, 5000 streamline samples, curvature thresholds = 0.2) was used for fiber tracking.17 Three portions of the ARAS were reconstructed by selection of fibers passing through region of interest (ROI) as follows:2–4 the dorsal lower ARAS, between the pontine RF (ROI 1) and the ILN (ROI 2),2 the ventral lower ARAS, between the pontine RF (ROI 1) and the hypothalamus (ROI 2),4 and the upper ARAS, in which the neural connectivity of the ILN (ROI 1) to the cerebral cortex was analyzed.3 The tract volume and the narrowest area of dorsal and ventral lower ARAS were measured by counting voxels. In both patients, the upper ARAS in which the neural connectivity of the ILN to the cerebral cortex did not show significant abnormalities. However, we observed the narrowing of the left dorsal lower ARAS between the pontine RF and the ILN in both patients and the tearing (patient 1) and narrowing (patient 2) of the left ventral lower ARAS between the pontine RF and the hypothalamus. The tract volume of the dorsal and ventral lower ARAS were 280/322 (right) and 149/172 (left) voxels in the patient 1, and 320/201 (right) and 185/49 (left) voxels in the patient 2. In addition, compared with the right hemisphere (100%), the narrowest area of left hemisphere in the dorsal and ventral lower ARAS on an axial slice were as follows—the patient 1: 7 voxels (29.2%, right: 24 voxels) and 11 voxels (26.8%, right: 41 voxels), and the patient 2: 15 voxels (33.3%), right: 45 voxels) and 3 voxels (15%, right:20 voxels) (Figure 1). DISCUSSION In the present study, using DTT, we evaluated the 3 portions of the ARAS: the upper ARAS in which the neural connectivity of the intralaminar thalamic nucleus to the cerebral cortex, the dorsal lower ARAS, between the pontine RF and the ILN, and the ventral lower ARAS, between the pontine RF and the hypothalamus. We found that the dorsal and ventral lower ARAS was torn or narrowed in both patients. The posttraumatic fatigue and hypersomnia in these patients might be mainly attributed to the injury of the left dorsal and ventral lower ARAS. Since introduction of DTI, a few studies have reported on injury of the ARAS in patients with TBI.5,6 In 2013, Edlow et al (2013) reported on a patient with coma following severe TBI who showed complete disruption of white matter pathways connecting brainstem arousal nuclei to the basal forebrain and thalamic nuclei, and partial disruption of the pathways connecting the thalamus and basal forebrain to the cerebral cortex.5 Jang et al (2015) recently demonstrated recovery of the injured lower portion of the ARAS between the pontine RF and the ILN in a patient with severe TBI.6 On the other hand, descending reticular activating system, which is involved in the generation of movement using mediating the spinal motoneurons, could also be related to the state of consciousness. In 2013, Tapia et al suggested that arousal state was related to muscular activation which was mediated by the descending reticular activating system.18Therefore, to the best of our knowledge, this is the first study to demonstrate injury of the lower portion of the ARAS between the pontine RF and the ILN in patients with mild TBI. Nevertheless, limitations of this study should be considered. First, because it is a case report, this study is limited; therefore, conduct of further studies comprising a large number of patients would be necessary. Second, despite being a powerful anatomic imaging tool, because regions of fiber complexity and crossing can prevent full reflection of the underlying fiber architecture, DTI may underestimate or overestimate the fiber tracts.19 In conclusion, this study demonstrated injuries of the dorsal and ventral lower portions of the ARAS in patients with fatigue and hypersomnia following mild TBI. We believe that these injuries of the ARAS might be a pathogenetic mechanism of fatigue and hypersomnia in patients with TBI. Conduct of further studies on this topic should be encouraged . 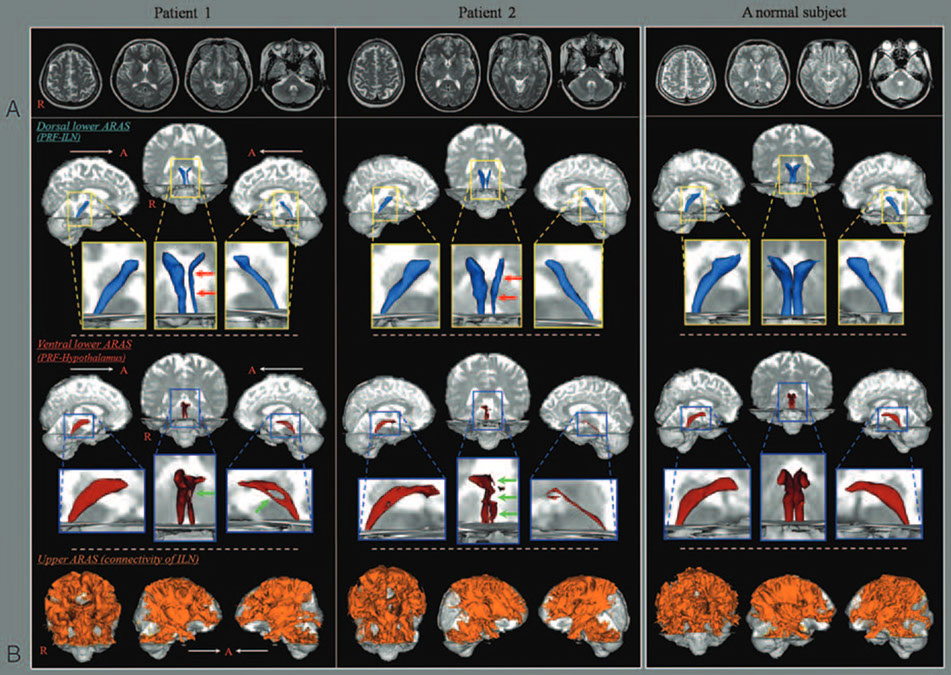
![]() FIGURE 1.(A)T2-weighted brain MR images at 11 months (patient 1) and 3 months (patient 2) after onset show no abnormal lesion.(B)Results of diffusion tensor tractography (DTT). The narrowing (red arrows) of the left dorsal lower ascending reticular activating system(ARAS) between the pontine reticular formation and intralaminar thalamic nucleus in both patients, and the tearing (patient 1, greenarrow) and narrowing (patient 2, green arrows) of the left ventral lower ARAS between the pontine reticular formation and thehypothalamus are observed compared with the right side of each patient and both sides of a normal subject (45 year-old woman).ARAS¼ascending reticular activating system, DTT¼diffusion tensor tractography, ILN¼intralaminar thalamic nucleus, MR¼magneticresonance, PRF¼pontine reticular formationxclick here to close and return to report
FIGURE 1.(A)T2-weighted brain MR images at 11 months (patient 1) and 3 months (patient 2) after onset show no abnormal lesion.(B)Results of diffusion tensor tractography (DTT). The narrowing (red arrows) of the left dorsal lower ascending reticular activating system(ARAS) between the pontine reticular formation and intralaminar thalamic nucleus in both patients, and the tearing (patient 1, greenarrow) and narrowing (patient 2, green arrows) of the left ventral lower ARAS between the pontine reticular formation and thehypothalamus are observed compared with the right side of each patient and both sides of a normal subject (45 year-old woman).ARAS¼ascending reticular activating system, DTT¼diffusion tensor tractography, ILN¼intralaminar thalamic nucleus, MR¼magneticresonance, PRF¼pontine reticular formationxclick here to close and return to report
Hypersomnia due to injury of the ventral ascending reticular activating system following cerebellar herniation: A case report
https://pubmed.ncbi.nlm.nih.gov/28072702
Recovery of Hypersomnia Concurrent With Recovery of an Injured Ascending Reticular Activating System in a Stroke Patient: A Case Report
https://pubmed.ncbi.nlm.nih.gov/26765455
Aggravation of excessive daytime sleepiness concurrent with aggravation of an injured ascending reticular activating system in a patient with mild traumatic brain injury
https://pubmed.ncbi.nlm.nih.gov/28121943
Sleep wake disturbances after traumatic brain injury
https://pubmed.ncbi.nlm.nih.gov/26067127
Traumatic brain injury: neuropathological, neurocognitive and neurobehavioral sequelae
https://pubmed.ncbi.nlm.nih.gov/30929221
Difference in the Ascending Reticular Activating System Injury Between Mild Traumatic Brain Injury and Cerebral Concussion
https://pubmed.ncbi.nlm.nih.gov/31098319
Chronic Upregulation of Cleaved-Caspase-3 Associated with Chronic Myelin Pathology and Microvascular Reorganization in the Thalamus after Traumatic Brain Injury
https://pubmed.ncbi.nlm.nih.gov/30322151
Excessive Daytime Sleepiness and Injury of the Ascending Reticular Activating System Following Whiplash Injury
https://pubmed.ncbi.nlm.nih.gov/29896079
![]()
Hyperbaric Treatment (HBOT
stem cell trials and stem cell precursor
TRT and HRT
Cortisol https://bra.in/5jMQre
Cerebrolysin https://bra.in/8j4AaG
x
click here to close and return to report

click for full size, click 'x' button to close
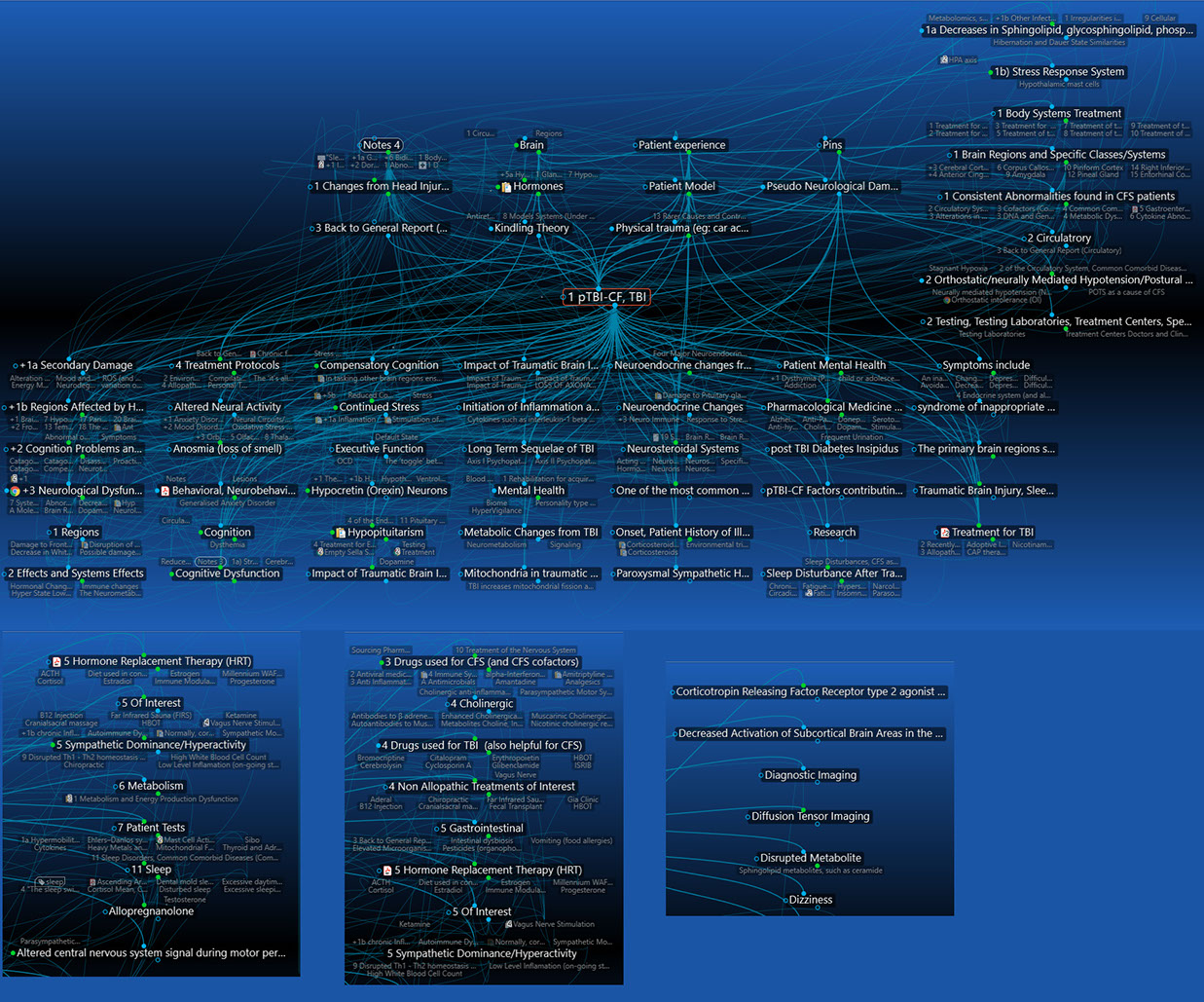
Topics associated with pTBIcf
To view this page on full report, click https://bra.in/6vNaYz













