Melatonin Supplements Review
Find the Best Melatonin
Supplements. Trouble Sleeping? See CL's Tests of Melatonin Supplements
and Top Picks.
Medically reviewed and
edited by Tod Cooperman, M.D. 
Last Updated![]() : 11/18/2021 | Initially Posted:
02/21/2020Latest Update: Fracture Risk with Melatonin Supplements?
: 11/18/2021 | Initially Posted:
02/21/2020Latest Update: Fracture Risk with Melatonin Supplements?

Recent Reviews
·
Aloe Juices, Gels, and Supplements
Review
·
NAD Booster Supplements Review
(NAD+/NADH, Nicotinamide Riboside, and NMN)
·
PQQ (Pyrroloquinoline Quinone)
Supplements Review
Table of Contents
Summary
·
Does melatonin work? Melatonin supplements can help you fall
asleep when taken before bedtime (30 to 60 minutes before for regular pills; 20
minutes before for fast-dissolve pills, chewables, and liquids and chewables).
Melatonin may also alleviate certain types of stomach pain and reduce anxiety
associated with medical procedures (see What It Does).
·
How much melatonin to take: Melatonin is a hormone; use it only as
needed, not every night. Try the lowest dose that will work for you, starting
with about 1 mg or less. If that doesn't work, try 3 mg. Some products contain
greater amounts, such as 5 or 10 mg, which may be more than you need and can
leave you groggy and have other negative effects. Timed release products may
help you not just fall asleep but also stay asleep, but they won't help you
stay asleep as well as a prescription sleep medication (see
ConsumerTips™: What to Consider When Using).
·
What did CL's tests of melatonin supplements show? In laboratory
testing, one melatonin supplement was Not Approved, as it contained nearly twice its listed
amount of melatonin. Our cost comparisons showed you could spend as little as 1
cent to over $5 per milligram of melatonin -- and the product that failed was
among the more expensive products (see What CL Found).
·
Best melatonin supplement? Among 22 CL Approved products, CL
selected Top Picks for
low, moderate, high-dose and timed release melatonin, as well as a product for
pets. These products represent superior quality and value.
·
Melatonin safety and side effects: Short-term use of
melatonin supplements appears to be generally safe for adults. However,
melatonin can potentially affect blood pressure as well as testosterone and
estrogen levels. Melatonin can also interact with certain foods and
medications. Long-term use is associated with an increased risk of bone
fracture. It is probably best to use melatonin "as needed" rather
than on a regular basis (see Concerns and Cautions).
What It Is:
Melatonin
(N-acetyl-5-methoxytryptamine) is a hormone produced by the pineal gland in the
brain from the amino acid tryptophan. The melatonin in dietary supplements is
generally manufactured synthetically or extracted from plants (in which
melatonin also plays a biological role) and both are chemically identical to
the melatonin in your body. Many foods, including nuts, contain extremely tiny amounts
of melatonin — not enough in a typical serving to provide therapeutic amounts
of melatonin.
What It Does:
For Trouble Falling Asleep and Related Conditions:
Melatonin is known to play a role in regulating the body's natural wake-sleep
cycle (circadian rhythm), triggering sleep. Levels of melatonin increase as
exposure to light decreases, and decrease as light exposure increases. On this
basis, it has been proposed as a treatment for people whose natural sleep
cycles have been disturbed.
In adults
A study in China among 97 middle aged men and women (average age
57) with primary insomnia (difficulty sleeping not due to a
medical or mental health condition) found that 3 mg of fast-release melatonin
taken one hour before bedtime for 4 weeks decreased the percentage of time
spent in non-REM sleep (light sleeping from which it is easy to waken) and
decreased early waking by an average of 30 minutes (as measured by
polysomnography, i.e., physiological changes during sleep) compared to placebo.
However, melatonin did not shorten the time it took to fall
asleep, increase total sleep time, decrease waking during sleep, or improve
self-reported sleep quality (Xu, Sleep Med 2020).
Beta blockers have been reported to cause
difficulty sleeping, possibly due to the fact they can suppress the body's own
production of melatonin at nighttime. A small study found that, compared to
placebo, 2.5 mg of melatonin taken one hour before bedtime for three weeks
slightly decreased the amount of time it took to fall asleep by 8 minutes and
increased total sleep time by an average of 37 minutes in men and women who
were taking beta blocker medications (atenolol (Tenormin) or metoprolol
(Lopressor, Toprol XL)) to treat high blood pressure (Sheer, Sleep 2012). There were no adverse
effects.
Melatonin may modestly help people with delayed
sleep phase syndrome (DSPS), a condition in which people cannot fall asleep
until early morning, possibly due to a delay in the body's production or
release of melatonin. In a study in Australia, 104 men and women with DSPS took
either a placebo or 0.5 mg of fast-release melatonin one hour before desired
bedtime for at least 5 nights per week for one month in conjunction with
setting a scheduled bedtime. Those who took the melatonin fell asleep an
average of 34 minutes earlier and had significant decreases in self-reported
sleep disturbance, severity of insomnia, and interference with daily life
compared to placebo. However, by the end of the study there didn't appear to be
any increase in natural melatonin production around the desired bedtime —
suggesting that the treatment did not correct the underlying condition (Sletten, PLOS Med 2018).
Melatonin may also improve sleep in people with Parkinson's
disease (in which the body's own production of melatonin may
decrease), but it does not improve motor symptoms of Parkinson's (Mack, Oxid Med Cell Longev 2017; Medeiros, J Neurol 2007). This
was most recently shown in a study in Korea of 34 men and women with
Parkinson's disease and poor sleep quality. A 2 mg dose of prolonged-release
melatonin taken one hour before bedtime daily for one month improved
self-reported sleep quality (particularly the time it took to fall asleep and
sleep disturbances), but not motor symptoms, compared to placebo. The study was
funded by Kuhnil Pharmaceutical Company, which markets prolonged-release
melatonin (Circadin) sold as a prescription drug in certain countries,
but not in the U.S (Ahn, Parkinsonism Relat Disord 2020).
A study in Korea found that melatonin was not helpful in
men and women with REM sleep behavior disorder (RBD) (a
condition characterized by intense dreams and behavior such as laughing,
yelling, kicking and punching during sleep) of unknown origin. In the study, 2
mg or 6 mg of prolonged-release melatonin taken 30 minutes before bedtime for
one month did not reduce the frequency or severity of episodes, nor improve
sleep quality, compared to placebo. The melatonin used in the study (Circadin,
Neurim Pharmaceuticals) is sold as a prescription drug in certain countries, but
not in the U.S. RBD can occur in people with Parkinson's disease, although none
of the study participants had Parkinson's disease (Jun, Ann Clin Transl Neurol 2019).
Melatonin may also help with sleep problems that occur with withdrawal
of sleeping medication. It has been shown to improve sleep in people
with schizophrenia, and those with Alzheimer's disease.
It has also shown a sleep benefit in people with diabetes; however,
it may impair insulin action (see the Concerns and Cautions section for more
details).
Some benefit has been seen in sleep disorders relating to blindness and delayed
weekend sleep pattern (difficulty falling asleep Sunday night after
staying up late Friday and Saturday night).
Inconsistent evidence suggests that it may aid sleep in jet travelers who
have crossed several time zones.
Although some studies of shift work showed
no benefit with melatonin, a small study among young doctors and nurses doing
three consecutive nightshifts found that taking 6 mg of a slow-release
melatonin product (Circadin, Flynn Pharmaceuticals Ltd.) before sleep
each morning modestly improved concentration and attention before and after
each work shift, although no measures of sleep improved (Thottakam, Front Psychiatry 2020). Another
study, among 27 overweight female night-shift nurses (average age 37) in
Brazil, showed that 3 mg of melatonin taken 1 hour before bedtime on days off
for 12 weeks reduced sleep rhythm misalignment on days off by about 20%
compared to placebo. There were also very slight reductions
in bodyweight (less than one pound), BMI, and waist and hip
circumference without any changes in diet or activity levels,
but only in participants who were considered early chronotypes
(i.e., those who reached mid-sleep earlier in their sleep cycle) (Marqueze, J Pineal Res 2021).
There is some evidence that melatonin may help improve
sleep in people with tinnitus. One clinical study also suggests it may
improve symptoms of tinnitus. The study compared melatonin to drug treatment
(sulpiride) or placebo and found that people who took 3 mg of melatonin daily
for one month had a 40% reduction in perception of tinnitus, compared to a 56%
reduction in those taking the drug and a 22% reduction in those taking a
placebo (Lopez-Gonzalez, J Otolaryngol 2007). Those who
took sulpiride and melatonin had an 81% reduction in perception of tinnitus,
suggesting that melatonin may enhance the effects of the drug.
In women, the body's own production of melatonin at
nighttime may be decreased after menopause (Toffol, Menopause 2014). A study in
Poland among 60 postmenopausal women ages 51 to 64 found that melatonin taken
twice daily (3 mg in the morning and 5 mg at bedtime) for one year modestly
reduced the self-reported severity of symptoms such as difficulty
sleeping, hot flashes and sweating, heart palpitations, dizziness,
irritability, and depressed mood compared to placebo. Those who took
melatonin had an average decrease of 9 points in overall symptom severity on a
scale of 1 to 51, compared to a decrease of 3 points for those who took the
placebo. Three women reported increased fatigue in the morning during the first
week of taking melatonin, but it was otherwise well-tolerated. There were no
significant changes in blood levels of melatonin, estradiol or
follicle-stimulating hormone (FSH) in either group at the end of the study
relative to the beginning of the study (Chojnacki, J Physiol Pharmacol 2018).
In children and adolescents
Melatonin has shown promise in the treatment of children
with chronic sleep problems. A study among 84 children (average age 10)
with chronic sleep onset insomnia (difficulty falling asleep) found 3 mg of
melatonin taken each night at 7:00 pm for 3 to 4 weeks modestly improved sleep
compared to placebo or bright light therapy. The time it took to fall asleep
decreased by about 16 minutes with melatonin and by about 8 minutes using
bright light therapy, while it increased by about 8 minutes among children
given a placebo. However, total sleep time increased by only 5
minutes in those who took melatonin due increased waking after initially
falling asleep (van Maanen, Sleep 2017).
The authors suggested that the increase in waking may indicate that the 3 mg
dose was too high -- noting other research which found lowering the dose of
melatonin may decrease waking, and the recent recommendation (Bruni, Eur J Paediatr Neurol 2017)
that children first try a lower dose (1 mg).
A 3-month study in the U.S. and Europe among 95 children
and adolescents with autism spectrum disorder (ASD) or
Smith-Magenis syndrome and insomnia which did not improve with behavioral
therapy investigated the effects of a prolonged-release melatonin supplement.
Participants received either 2 mg of prolonged release melatonin minitablet
daily (PedPRM from Neurim Pharmaceuticals — which funded the study)
or placebo for the first three weeks of the study and, if there was no
improvement, the dose was increased to 5 mg. Those who took melatonin fell
asleep an average of 25 minutes faster per night and slept an average of 32
minutes longer compared to those who took the placebo. No significant changes
in measures of blood pressure, heart rate or sexual development (important to
note as melatonin may affect testosterone/estrogen metabolism)
were found; however, headache (13% vs 6%) and daytime sleepiness (28% vs. 11%)
were more common in those taking melatonin than in those taking placebo (Gringas, J Am Acad Child Adolesc Psychiatry 2017). In
a follow-up study, 74 of the participants who chose to continue taking the
prolonged-release melatonin (at a dose of 2, 5 or 10 mg) for up to two years
were monitored for long-term safety. During this follow-up, the most frequent
adverse events were fatigue (6.3%), somnolence (6.3%), and mood swings (4.2%),
but changes in average weight, height, and body mass index remained within
normal ranges and there was no evidence of delay in BMI or pubertal development
(Malow, J Am Acad Child Adolesc Psychiatry 2020).
A study in Japan among 169 children and adolescents ages 6
to 15 years old (average age 10) with ASD and difficulty falling asleep
(requiring 30 minutes or more to fall asleep) persisting for three months or
longer found that 1 mg or 4 mg of melatonin, taken 45 minutes before bedtime
for two weeks, cut the time it took to fall asleep by 17 minutes and 23
minutes, respectively, compared to placebo. Melatonin supplementation did not
decrease the number of awakenings after falling asleep or increase total sleep
time, or improve behavioral or emotional symptoms compared to placebo. The 4-mg
dose was slightly more effective in reducing the time it took to fall asleep
compared to the 1-mg dose, and only the 4-mg dose was found to significantly
reduce the time it took to fall asleep in females, taller participants (> 4
ft. 6 in. in height) and those with a history of the sleep medication ramelteon
(which binds to and activates melatonin receptors in the body). However,
supplementation with the 4-mg dose was discontinued in one child as it appeared
to cause excessive sleepiness. For these reasons, the researchers recommended
that melatonin supplementation in children with ASD should be initiated at a
daily dose of 1 mg, and increased only if needed. The melatonin was provided by
Nobelpharma Co., Ltd, which also funded the study (Hayashi, J Autism Dev Disord 2021).
Also see ConsumerLab's answer to the question: Which supplements can help me sleep?
Before and After Medical Procedures and
Hospitalization:
Melatonin may help reduce anxiety and aid sedation before medical
procedures. It does not seem to aid sleep after surgery. It
may help in ICU settings.
Before procedures
A review of 27 clinical studies published between 2004 and
2019, all of which were conducted outside the U.S., concluded that melatonin
taken around 1 to 1 ½ hours before surgery reduces preoperative anxiety
compared to placebo, and, in some cases, as well benzodiazepine medications
such as midazolam, oxazepam, or alprazolam. In the studies reviewed, doses
generally ranged from 3 mg to 10 mg of melatonin (given as tablets or a
liquid). In most cases melatonin was taken by mouth, although in about
one-third of the studies melatonin was given sublingually. Few adverse events
were associated with taking melatonin, although mild nausea, sleepiness,
dizziness, and headache were reported in some of the studies (Madsen, Cochrane Database Syst Rev 2020).
In a clinical study (only the abstract appears to be available) in children age
of 14 and younger, a dose of between 0.5 and 5 mg (0.5 mg/ per kg) taken 30
minutes before a blood draw was found to significantly reduce anxiety and pain
levels compared to placebo (Marseglia, J Biol Regul Homeost Agents 2015).
In intensive care units
Melatonin supplementation may improve sleep quality for patients in intensive
care units where circadian rhythms can be disrupted by 24-hour lighting in
these rooms, but it does not appear to improve sleep after
surgery, which may largely be disrupted due to pain (Lewis,
Cochrane Database Syst Rev 2018).
A study in Brazil among 203 patients hospitalized
in ICU (average age 59) found that 10 mg of melatonin (Now Foods)
given 2 hours after dinner for up to 7 nights improved overall sleep quality as
self-reported and/or assessed by nurses. Compared to placebo, a greater number
of patients given melatonin experienced "very good sleep" (46% vs. 34%)
and fewer had "very poor sleep" (3% vs 14%). Melatonin did not reduce
the use of analgesics or sedatives, or reduce the occurrence of pain, anxiety
or delirium (as has been reported in post-operative patients in another study). The melatonin capsules used in this
study were opened and given via intestinal or nasogastric feeding tubes (Gandolfi, Crit Care Med 2020).
After surgery
In a study of 118 men and women who had just had total hip or knee replacement
surgery, taking 6 mg of melatonin one hour before bedtime did not decrease the
amount of time it took to fall asleep, increase sleep duration, or improve
sleep quality compared to placebo, nor did it decrease the use of
anti-inflammatory medication after surgery (Clarkson,
J Am Acad Orthop Surg 2021).
Reduced melatonin levels following surgery have been
implicated in the development of post-operative delirium (Cronin, Lancet 2000; Lewis, Med Hypotheses 2004), a state of
altered mental status that can cause confusion, agitation and emotional
dysregulation that occurs in approximately 15% of hospitalized older adults (Travers, Curr Gerontol Geriatr Res 2013).
However, a study among 166 men and women (average age 68) in Australia
undergoing major cardiac surgery found that supplementation with melatonin (3
mg taken for seven consecutive nights, starting two nights before surgery)
did not reduce the incidence, severity, or duration of
delirium compared to placebo. Further analysis suggested that melatonin may
have reduced the risk of people age 75 or older but increased the risk among
those with the lowest cognitive performance scores (Ford, J Am Geriatr Soc 2019).
After strokes
Giving 2 mg of melatonin within 24 hours after an ischemic
stroke was shown to modestly reduce risk of post-stroke delirium (PSD) in
an analysis of patients hospitalized in Germany. Melatonin was given along with
standard treatment and was continued once nightly until discharge. PSD occurred
in 25.6% of patients who received melatonin versus 36.6% of those who did not
receive melatonin (Mengel, Eur J Neurol 2021).
Headache:
A placebo-controlled study among 178 men and women
diagnosed with migraine (with or without aura) found that 3 mg
of melatonin taken daily for three months was modestly effective in reducing
the number of days of migraine headache per month (from an average of 7.3 prior
to treatment to 4.6 during the last month of treatment; placebo fell from 7.3
to 6.2 days). As part of the study, a group of patients received 25 mg daily of
amitriptyline, an antidepressant used to prevent migraine. This was also
modestly effective (7.2 days of headache falling to 5.0 days) but not
statistically better than melatonin and it caused more side effects, including
weight gain (Goncalves, J Neurol Neurosurg
Psychiatry 2016).
Melatonin has also been reported to reduce episodes of primary stabbing
headache, or PSH (brief but intense jabs of head pain lasting several
seconds per episode). In adults with PSH, taking between 3 mg and 12 mg of
melatonin nightly for two to four months has been reported to eliminate
episodes (Rozen, Neurology 2003). A
7-year-old boy in Columbia who experienced approximately 21 episodes of primary
stabbing headache per month given 1.5 mg of melatonin nightly experienced only
two episodes within the first two weeks of supplementation, and had no further
episodes during six months of supplementation. The authors of the report noted
that melatonin has anti-inflammatory, analgesic, and antioxidant properties
that may play a role in reducing primary stabbing headaches, and that its
chemical structure is similar to indomethacin, an NSAID drug commonly
prescribed to treat PSH (Salazar, Colomb Med (Cali) 2018).
Cancer and Chemotherapy Side Effects:
Breast cancer
A study among 36 women in Brazil undergoing chemotherapy
after breast cancer surgery found that those who took melatonin (20 mg
each night, one hour before bedtime) for 10 days (beginning three days prior to
the first chemotherapy session had modest but statistically significant
improvements in sleep quality, symptoms of depression, and certain measures of
cognitive function (such as executive function and episodic memory) compared to
those who took a placebo (Palmer, PLoS One 2020). Similarly,
a study in Denmark, using a lower dose of melatonin, found that it helped women
fall asleep during the three months after having breast cancer surgery. Those
who received melatonin (6 mg each night, one hour before desired bedtime) had
4% greater sleep efficiency (the percentage of time asleep while in bed for
sleep) and slept an average of 37 minutes longer per night than those who
received placebo -- although there was no significant difference in self
assessments of sleep quality. Interestingly, only 1 out of the 28 patients
treated with melatonin dropped out of the study, compared to 10 out of the 26
given placebo. The study also aimed to assess cognitive function (which has
been known to decline) during the post-surgical period, but there was no
decline in either group (Hansen, Intl J Breast Cancer 2014).
Lung cancer
Disruption of sleep-wake cycles is common in cancer patients and has been
correlated with tumor progression in people with advanced non-small cell lung
cancer (NSCLC) (Du-Quiton, Psychooncology 2010; Grutsch, BMC Cancer 2011). A study among 67
men and women receiving chemotherapy (etoposide/cisplatin) for advanced NSCLC
found that overall survival time was greater for those given 20 mg of melatonin
every evening (8 pm) compared to those given placebo. This was
particularly true for those who began the study with normal self-reported sleep
quality, who had an average survival time of 17.6 months vs. 10.4 months for
those taking the placebo. A third group of participants, who took melatonin in
the morning (8 am), did not have increased
survival compared to placebo, but the researchers noted that none of the people
in this group began the study with normal sleep quality. There were no
improvements in tumor response to chemotherapy with melatonin, although all
participants who took melatonin (morning or evening) had improvements in
shortness of breath when measured three months after beginning supplementation
(Grutsch, Biol Rhythm Res 2021).
Other Uses:
Melatonin may be of some help to people with atopic
dermatitis -- a common type of eczema characterized by itchy
inflammation of the skin and affecting up to 10% of adults and 30% of children.
A placebo-controlled study in children and adolescents with atopic dermatitis
found that taking 3 mg of melatonin at bedtime every night for 4 weeks resulted
in about a 20% reduction in symptoms and a 21.4 minute decrease in the time to
fall asleep, with no adverse effects. It is unclear if or how melatonin may
have modulated inflammation, as it did not affect measures of immune function,
such as immunoglobulin E levels (Chang, JAMA Pediatr 2016).
Several small studies suggest melatonin may help reduce certain
symptoms of irritable bowel syndrome (IBS), although,
interestingly, it does not appear to reduce sleep disturbance. A small study
among women with IBS found that 3 mg of melatonin taken every night before
bedtime for two months reduced abdominal distension and pain, and abnormal
sensations (urgency, strain, incomplete bowel movement) compared to placebo,
although there were no changes in stool consistency or frequency and no
improvements in sleep or mood (Lu, Aliment Pharmacol Ther 2005).
Two other studies using the same dose of melatonin taken at bedtime found
similar results, with significant improvements compared to placebo in overall
IBS scores (45% vs. 17% improvement) and quality of life scores (44% vs. 15%
improvement) (Saha, J Clin Gastroenterol 2007),
and reductions in abdominal pain scores (2.35 vs 0.70) (Song, Gut 2005), but no improvements in sleep.
In addition to being produced in the brain, melatonin is
also produced by cells in the gut — particularly those lining the stomach.
There is preliminary evidence that supplemental melatonin may be beneficial in
reducing various types and causes of stomach pain, although more
research is needed:
·
Among people with H. pylori bacterial infection
of the stomach (a common cause of stomach ulcer), those who are
symptomatic (experiencing pain) have been shown to have lower nighttime blood
plasma levels of melatonin (Wilhelmsen, J Pineal Res 2011), as well as
lower expression of enzymes which synthesize melatonin (Chojnacki, Biomed Res Intl 2013). Animal
studies suggest that melatonin may help protect the stomach lining and aid
ulcer healing. One study in Poland among people with stomach or duodenal ulcers
showed that taking 5 mg of melatonin twice daily along with triple therapy
(i.e., metronidazole, amoxicillin and omeprazole) for 2 weeks helped heal
ulcers by week 3 in more people compared to triple therapy alone (100% vs. 50%)
(Celinski, J Physiol Pharmacol 2011). However,
the triple therapy used in this study was not the regimen used in the U.S.
·
Animal studies and preliminary human studies suggest that
supplementing with melatonin may reduce the pain of gastroesophageal
reflux disease (GERD). A small study among people with GERD found that a 3
mg daily dose of melatonin for 4 and 8 weeks helped relieve pain associated
with GERD, although not as well as omeprazole (Prilosec). However, these
results are not meaningful because the study did not have a control group of
people with GERD not receiving any treatment, i.e., some of the improvement may
have occurred without treatment (Kandil, BMC Gastroent 2010). Another study
using 6 mg of melatonin at bedtime in a formula including 100 mg of
L-tryptophan, B vitamins, methionine and betaine, reported complete regression
of symptoms after 40 days in 100% of patients, compared to 65.7% of patients
given 20 mg of omeprazole (Pereira, J Pineal Res 2006). The results of
this study are questionable as it was not double-blind, i.e., the researchers
knew which patients received melatonin. The same formula was reported to
successfully treat symptoms in a 64-year old woman with GERD treated for 40
days, although changing the treatment to just 3 mg of melatonin alone for 10
months resulted in some return of symptoms (Werbach, Altern Ther Health Med 2008). Be
aware that any treatment of GERD would likely be long-term and melatonin has
not been adequately studied for long-term use — with which there is a concern
over increased risk of bone fracture.
·
A small study in adults with functional dyspepsia (stomach
pain not caused by an ulcer) found that twelve weeks of melatonin (5 mg taken
at bedtime) resulted in complete resolution of epigastric pain in 56.6% of
patients as compared to only 6.7% of the patients who received placebo (Klupinksa, J Clin Gastroent 2007), although a
study in among children (ages 8 to 17) with functional dyspepsia (who failed to
respond to acid suppression medication) taking 5 mg of melatonin daily for two
weeks was no better than placebo at reducing pain (Zybach, World J Gastro Pharm Ther 2016).
Middle-aged
women in Spain with fibromyalgia reported improvements when
given increasing doses of melatonin (ranging from 3 mg to 15 mg). Each dose was
taken 30 minutes before going to bed for 10 days, preceded by 10 days of
placebo. Although a decrease in pain was reported with 3 mg
and 6 mg doses, it only became only statistically significant at doses of 9 mg
and higher, as was the case with improvements in self-reported
"fitness." Improvements in anxiety and "frame of mind" were
statistically significant at doses of 12 mg and 15 mg. The researchers noted
that other studies using lower daily doses of melatonin (3 mg to 10 mg) over
longer periods (1 to 2 months) have also shown reductions in pain in people
with fibromyalgia. Cortisol levels decreased with 6 mg and progressed with
increasing doses (Castrano, Biol Res Nurs 2018).
Research suggests that melatonin has can
increase bone density but, unfortunately, it may also make
bone more susceptible to fracture. A placebo-controlled study in Denmark
among post-menopausal women with bone loss given 1 mg or 3 mg of melatonin
every night for one year, showed small, but significant, improvements in bone
density of the leg and spine. Most notably, at the 3 mg dose, bone
density in the neck of the femur in the hip increased relative to placebo by
2.3%, and inner bone thickness in the tibia (lower leg) and lumbar spine
increased by 2.2% and 3.6%, respectively. All participants were also given
calcium (800 mg) and vitamin D (800 IU) daily; while this increased calcium
loss in the urine among those receiving placebo, it did not among those
receiving melatonin (Amstrup, J Pineal Res 2015). However,
the study did not determine the effect on fractures, and there is increasing
concern that melatonin increases the risk of fractures by
interfering with the normal cycle of bone resorption and formation (see Concerns and Cautions); more research is
needed to determine if daily melatonin is beneficial for women experiencing
bone loss. Interestingly, further analysis of this year-long study showed
that, in women with a good quality of sleep, melatonin had no effect on sleep
quality; however, in poor quality of sleep, small doses of melatonin trended
towards improving quality. There was no effect on overall quality of life. The
study also found no hangover effect affecting balance and muscle function (Amstrup, Nutrition J 2015).
Melatonin may be moderately helpful to women with polycystic
ovary syndrome (PCOS), a condition affecting up to 10% of premenopausal
women and characterized by hyperandrogenism (causing symptoms including
hirsutism, i.e., unwanted male hair pattern, and ovulatory dysfunction). A
small study in Iran found that 5 mg of melatonin taken twice daily for 12 weeks
modestly reduced hirsutism and total testosterone, as well as biomarkers of
inflammation and oxidative stress compared to placebo (Jamilian, Front Endocrin 2019).
Other potential uses for melatonin include reducing symptoms of tardive
dyskinesia (a potential long term side-effect of anti-psychotic medications)
and nicotine withdrawal symptoms. There is preliminary evidence that melatonin
may also be useful as an adjunct to conventional therapy in treating some forms
of cancer, reducing side effects or enhancing drug efficacy.
It has been said that melatonin levels drop with age and, on
this basis, melatonin has been recommended as an "anti-aging"
supplement. This does not appear to be the case in healthy individuals, but
melatonin levels have been reported to be low in people with suffering from
advanced medical conditions including poorly controlled coronary artery
disease, as well as endocrine and liver disorders (Carillo-Vico, Int J Mol Sci 2013).
COVID-19
Some research suggests that people who take melatonin may
have a lower risk of COVID-19, the infection caused by the SARS-CoV-2
coronavirus, but there is no evidence proving that melatonin prevents COVID-19.
There is preliminary evidence that melatonin may shorten the duration of
certain symptoms of COVID-19, but better clinical trials are needed to prove a
benefit.
How melatonin might work:
Because melatonin can affect immune system responses and has
antioxidant properties, it has been theorized that melatonin may be beneficial
in preventing or treating COVID-19. Experiments in mice have shown melatonin
administration to reduce mortality due to a variety of viral infections,
increasing serum levels of cytokines (immune-regulating molecules) such as
interleukin-1 beta (Carillo-Vico, Int J Mol Sci 2013). Melatonin
also may also, indirectly, make it more difficult for SARS-CoV-2 to attach to
cells in the body by increasing the expression of angiotensin I converting
enzyme 2 (ACE2) and increasing the occupancy of ACE2 receptors, leaving fewer
receptors to which SARS-CoV-2 can attach (Zhou, Cell Discovery 2020).
Prevention:
A study of 11,672 patients tested for COVID-19 at Cleveland
Clinic locations in Ohio and Florida during March and April 2020 found that
those who were taking melatonin (dosage and duration not reported) were less
likely to have a positive test result. Individuals who had had a pneumococcal
polysaccharide or influenza vaccine or those who were taking paroxetine (Paxil)
or the beta-blocker drug carvedilol (Coreg) were also less likely to test
positive (Jehi, Chest 2020). While this is an
interesting finding, it does not prove that taking melatonin supplements can
prevent COVID-19. A clinical study is underway in health care
workers in Spain to test this.
Treatment:
Preliminary evidence suggests that giving melatonin to
people with severe COVID-19 infection may be helpful, although more studies are
needed to test this. A study among 791 patients with COVID-19 at New York
Presbyterian/Columbia University Irving Medical Center requiring mechanical
ventilation found that those who were given melatonin after intubation had a
13% lower risk of dying than those who did not receive melatonin, even after
considering other risk factors. Melatonin was given for reasons including
insomnia, anxiety, delirium and agitation, although dosages were not reported (Ramlall, medRxiv 2020 -- preprint).
A study in Iran among adults hospitalized with mild to
moderate COVID-19 infection found that the duration of hospitalization was
shorter for those given 3 mg of melatonin three times daily for two weeks along
with standard care compared to those given standard care alone (4.65 vs. 8.15
days), although there was no significant difference in the percentage of
patients admitted to ICU. After two weeks, fewer people in the melatonin group
experienced cough (4.2% vs. 25%), shortness of breath (0% vs. 15%) and fatigue
(8.3% vs. 30%) compared to those in the control group, but there was no
difference regarding fever, muscle pain, chill, headache, or other symptoms (Farnoosh, Authorea Preprints 2020).
See the ConsumerTips™ section of this review for
more information about suggested dosage and concerns and cautions.
Quality Concerns and
Tests Performed:
Neither
the FDA nor any other federal or state agency routinely tests supplements for
quality prior to sale. Consequently, ConsumerLab.com tested melatonin products
to determine if they contained listed amounts of melatonin. Standard tablets
and caplets were also tested to be sure that they would disintegrate
("break apart") properly (See Testing Methods and Passing Score for
more information).
Previous testing of melatonin supplements by ConsumerLab.com in 2015 found that
all contained their claimed amounts of melatonin (i.e., not exceeding 10% less
or 35% more than listed — allowing for normal manufacturing overage). A study
of 30 melatonin supplements from Canada found that the majority (71%) were not
within 10% of the amounts claimed on labels. Products with the most variability
were chewable tablets (one contained 478% of the labeled amount), combinations
with herbs (one contained 83% less than claimed), and capsules. Products least
likely to vary from labels were melatonin-only, particularly in the form of
regular or sublingual tablets, or as liquids. Tiny amounts of serotonin were found
in 26% of the products, in most cases likely due to natural phytoserotonin in
herbal ingredients (Erland, J Clin Sleep Med, 2017).
What CL Found:
All but one of the 13 supplements that ConsumerLab.com selected
for testing contained their claimed amounts of melatonin, and if a regular
tablet or caplet, disintegrated properly. An additional 10 products evaluated
through ConsumerLab.com's voluntary Quality Certification Program also
passed these tests.
The supplement that failed testing was Zarbee's
Naturals Children's Sleep With Melatonin — Natural Berry Flavor. It was
discovered to contain 1.9 mg of melatonin per gummy, which is nearly double the
1 mg claimed. This problem was confirmed in a second independent laboratory.
This is of concern because people should take the lowest effective dose of
melatonin. Accidentally taking a higher dose can lead to increased side
effects, such as next-day drowsiness. Also be aware that these gummies contain
sugar (1 gram per gummy) and are sticky, so, to avoid causing tooth decay, it
would seem prudent to have children brush their teeth well after using any gummy
product before bedtime.
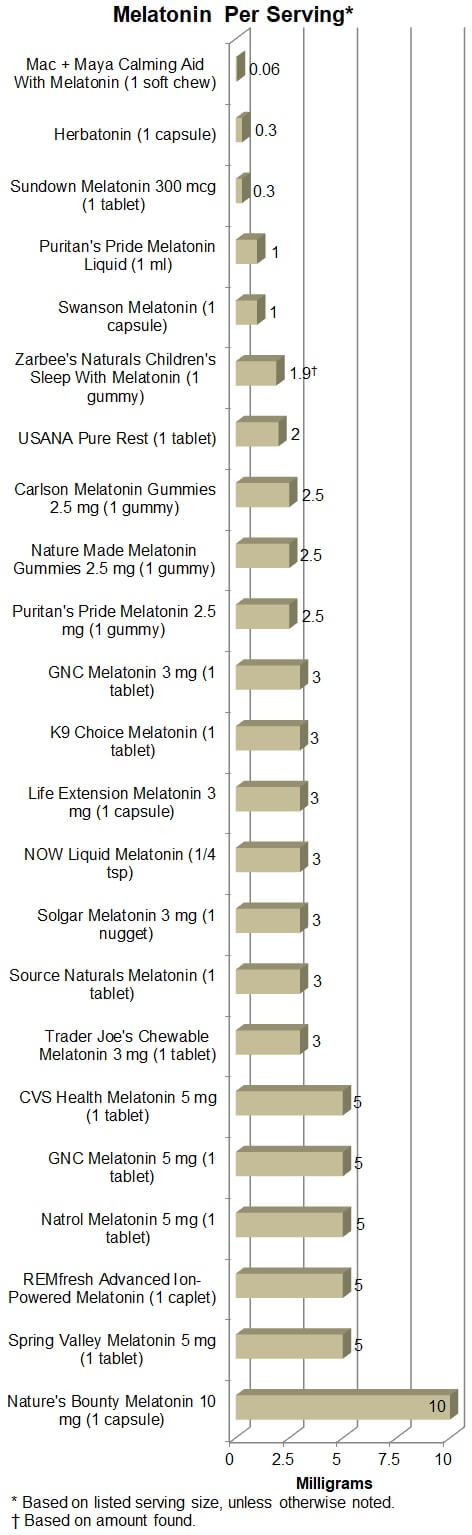
Wide range of strengths and cost:
Although we identified many high-quality products, there is a wide range of
dose per serving and pricing among the tested supplements. All of these
differences can be seen in the Results table. The following graphs highlight
the differences in dose per serving, which ranged from 0.06 mg (in a pet
supplement) to 10 mg of melatonin.
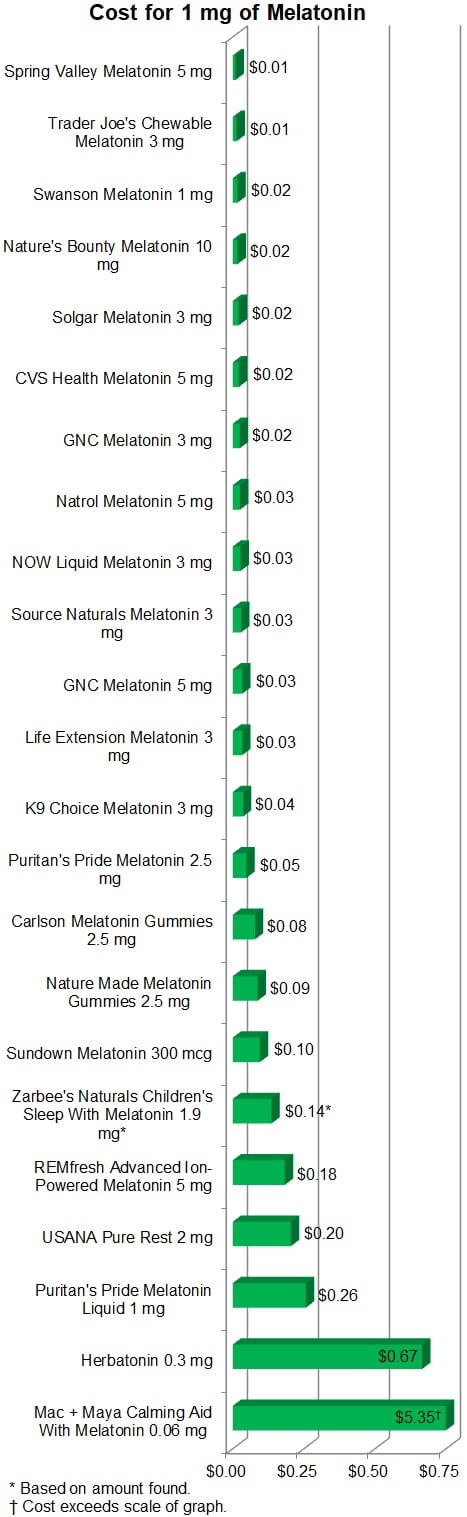
The following graph highlights the difference in how much you pay for melatonin
from each of the products reviewed. To compare apples-to-apples we calculated
this based on the cost to obtain 1 mg of melatonin from each product. This cost
varied more than 500-fold, from 1 cent to $5.35!
Top Picks:
Low Dose
ConsumerLab's overall Top Pick among melatonin supplements
and for a low dose is Swanson Melatonin 1 mg. Each capsule
provides 1 mg of melatonin for just 2 cents.
While 1 mg is a low dose, it's best to take as little melatonin as needed to
feel dozy, and just 0.3 mg can do this for some people (See What to Consider When Using for more
about dosage). Two products that were Approved provide exactly 0.3 mg. One is
nearly as inexpensive as Swanson and is suitable for
vegetarians: Sundown Naturals at 3 cents per vegetarian
tablet. The other is a lot more expensive, but is suitable for
vegans: Herbatonin at 20 cents per vegan capsule. Herbatonin is
described on its packaging as "slow-release" but it is not actually a
"timed-release" product. [Note: Herbatonin is also
sold exclusively through healthcare providers as HerbatoninPro,
although the capsules and their contents are the same, as we have
confirmed with the distributor of both, Symphony Health.] An even less
expensive and more versatile option than either of these is to use a smaller
than recommended dose of our Top Pick among liquids -- NOW
Liquid Melatonin. Just 2 drops will give you 0.3 mg of melatonin for only 1
cent!
Moderate dose
If a low dose doesn't work for you, it is okay to move to a moderate dose.
Our Top Pick for moderate dose melatonin is Trader
Joe's Chewable Melatonin 3 mg — Peppermint Flavor costing 4 cents
per tablet. Be aware that it contains lactose, so if you are lactose-intolerant
consider, instead, our Top Pick for vegans in the moderate
dose category -- Solgar Melatonin 3 mg at 6 cents per
nugget.
Although a few cents more, our Top Pick for liquid
melatonin, NOW Liquid Melatonin, will also give you 3 mg of
melatonin, for 8 cents, at its recommended serving of 20 drops. As mentioned
earlier, it also gives you the flexibility to adjust your dose to the lowest
that works for you by varying the number of drops you choose to use. This also
make it a good choice for families in which the appropriate dose may differ by
family member.
A word about gummies: Three gummies were Approved in our tests,
each providing 2.5 mg of melatonin per gummy at a cost of 12 to 22 cents. As
these gummies are sticky and each contain one gram of sugar, if you choose to
use a gummy it would be best to brush your teeth well before going to bed to
avoid fostering tooth decay and gum inflammation.
Timed release
While regular melatonin may help you fall asleep, timed release formulas may
help you to stay asleep for a few hours after you dose off — although not as
well as a prescription sleep medicine. If you have trouble with waking during
the night, you may want to try this type of formula.
We tested two products labeled as "timed release" (Source Naturals
3 mg and CVS 5 mg) and one that claimed to release
melatonin "continuously for up to 7 hours" (REMfresh Advanced
Ion-Powered Melatonin). All contained their labeled amounts of melatonin.
We did not determine the extent to which the timed release products delayed
melatonin release, but we did check to see if the REMfresh caplets
could do what has been claimed (Seiden, Prim Care Companion CNS Disord 2019).
We put REMfresh caplets in simulated gastric fluid, which
caused them to lose their outer coats (which contains the initial dose of
melatonin) and then we moved them into simulated intestinal fluid, in which
they very gradually disintegrated over several hours, as promised.
Although it is an expensive product (92 cents per 5 mg caplet), REMfresh was
the only special-release product for which we could verify timed-release
activity. For this reason, our Top Pick among timed release
melatonin products is REMfresh.
High dose
If a low dose doesn't work for you, our Top Pick is Well
at Walgreens Quick Dissolve Melatonin 3 mg costing 4 cents per tablet.
Although it may not be necessary, you can get 2 mg more melatonin per pill and
save a penny with H-E-B Super Strength Melatonin 5 mg.
We only tested one high-dose product, Nature's Bounty Melatonin 10 mg,
which is our Top Pick for high-dose melatonin, providing
10 mg per capsule for 17 cents. We suggest, however, not using a
high-dose product as it should not be necessary for sleep purposes, is more
likely to cause next-day drowsiness, and little is known about its long-term
safety.
For Pets
We tested two melatonin supplements for dogs. Our Top Pick for
dogs is K9 Choice Melatonin — Peanut Butter Flavored Tabs at 11 cents
for 3 mg of melatonin per chewable tablet. The other product that we
tested, Mac + Maya Calming Aid with Melatonin provides only
0.06 mg of melatonin per soft chew and costs 32 cents. (See
"Directions" in the third column of the results table for recommended
dosages based on the weight).
Test Results by Product:
Listed
below are the test results for 23 melatonin supplements. Products are listed
alphabetically. ConsumerLab.com selected 13 of these products. Ten products
(each indicated with a CL flask) were tested at the request of their
manufacturers/distributors through CL's voluntary Quality Certification Program and are
included for having passed testing.
Shown for each product are the claimed amount of melatonin and the serving size
recommended on its label. Products listed as "Approved" met their
label claims and ConsumerLab.com's quality criteria (see Passing Score). Directions for use and pill
size are in the 3rd column. The price
per serving and a comparison of the cost (shown in brackets) to obtain 1 mg of
melatonin are shown in the 4th column. Notable features, including special dietary
designations, are shown in the 5th column. The full list of ingredients) is available the
last column. You may need to swipe sideways on the table to view all
columns.
Results of
ConsumerLab.com Testing of MELATONIN SUPPLEMENTS
(Click arrows or swipe left or right to see all columns)
Approval Statusⓘ
Product Name
Claimed Amount of Melatonin Per Servingⓘ
Disintegration
Directions
Pill Sizeⓘ
Cost per Serving
[Cost per 1 mg Melatonin]
Price
Notable Features
Full List of Ingredients Per Serving
Low Dose: 1 mg or less:
APPROVED
Top Pick
for Vegans - Low Dose
Herbatonin®
![]()

Dist. by Symphony Natural Health
1 capsule
0.3 mg
✔
NA
Take 1 capsule once daily or as directed by your
healthcare practitioner.
Medium/large vegan capsule
$0.20/vegan capsule
[$0.67]
$17.99/90 vegan capsules
Gluten Free. Vegan. Kosher. Contains No:
chemicals, solvents, excipients, preservatives, artificial colors or flavors,
sucrose, yeast, dairy, soy, wheat, corn or gluten.
1 capsule
Melatonin [From Plant Origin (100:1 extract - Oryza sativa spp, Medicago sativa
& Chlorella pyrenoidosa - Leaves & Stems)] 0.3 mg.
Other Ingredients: Hypromellose (plant derived cellulose) capsule.
APPROVED
Puritan's Pride® Melatonin Liquid - Natural Black
Cherry Flavor![]()
![]()

Dist. by Puritan's Pride, Inc.
1 ml
1 mg
✔
NA
For adults, take one (1) to four (4) mL at
bedtime only as melatonin may product drowsiness.
Liquid from bottle
$0.26/ml
[$0.26]
$15.18/2 fl oz [59 ml] bottle (approx. 59 servings)
No Artificial Flavor, No Artificial Sweetener,
No Sugar, No Milk, No Lactose, No Soy, No Gluten, No Wheat, No Yeast, No Fish.
1 ml
Melatonin (as n-Acetyl-5-Methoxy-tryptamine) 1 mg.
Other Ingredients: Vegetable Glycerin, Water, Natural Black Carrot and Black
Currant Concentrates (Color), Citric Acid, Natural Black Cherry Flavor, more...
APPROVED
Sundown® Melatonin 300 mcg
![]()

Mfd. by Rexall Sundown, Inc.
1 tablet
0.3 mg
✔
✔
For Adults, Take One (1) Tablet 30 Minutes
Before Bedtime.
Medium circular tablet
$0.03/tablet
[$0.10]
$3.44/120 tablets
Gluten Free. Dairy Free. Vegetarian. Non-GMO. No
Gluten. No Wheat. No Milk. No Lactose. No Artificial Color. No Artificial
Flavor. No Artificial Sweetener. No Preservatives. No Soy. No Yeast. No
Peanuts. No Tree Nuts. No Fish. Sodium Free.
1 tablet
Melatonin 300 mcg.
Other Ingredients: Vegetable Cellulose, Dextrates, Vegetable Magnesium
Stearate.
APPROVED
Top Pick
for Low Dose - 1 mg
Swanson® Melatonin
![]()

Dist. by Swanson Health Products
1 capsule
1 mg
✔
NA
As a dietary supplement, take one capsule with
water one half-hour before bedtime.
Medium/large capsule
$0.02/capsule
[$0.02]
$1.99/120 capsules
None.
1 capsule
Melatonin 1 mg.
Other Ingredients: Rice flour, gelatin.
NOT APPROVED
Zarbee's Naturals® Children's Sleep With
Melatonin - Natural Berry Flavor
![]()

Dist. by Zarbee's Inc.
1 gummy
1 mg
Found 1.9
mg per serving (187% of listed amount)
NA
If your child weighs less than 31 lbs. (14 kg),
this product is not recommended for use. 3 Years to 5 Years: Consult your
physician for adequate serving, not to exceed 1 gummy. 6 Years to 12 Years:
Take 2 gummies. 12 Years and Older: Take 3 gummies.
Medium/large bee-shaped gummy
$0.25/gummy
[$0.25 based on amount listed]
[$0.14 based on amount found]
$12.74/50 gummies
Allergen Friendly. Manufactured in a facility
without: Milk, Egg, Fish, Shellfish, Tree Nut, Wheat, Peanut, Soy. No Drugs or
Alcohol. No High Fructose Corn Syrup. No Artificial Sweeteners. No Artificial
Flavors.
1 gummy
Calories 5, Total Carbohydrate 2 g, Total Sugars [Includes Added Sugars 2 g] 2
g, Melatonin 1 mg.
Other Ingredients: Honey, Glucose Syrup, Sucrose, Water, Pectin, Natural
Flavors, Citric Acid, Sodium Citrate, more...
Moderate Dose: 2 mg to 5 mg:
APPROVED
Carlson® Melatonin Gummies 2.5 mg - Natural
Strawberry Flavor![]()
![]()

Dist. by Carlson Div. of J.R. Carlson
Laboratories, Inc.
1 gummy
2.5 mg
✔
NA
Adults: Take one gummy one to two hours before
bedtime.
Medium/large gumdrop-shaped gummy
$0.20/gummy
[$0.08]
$11.74/60 gummies
Gluten-free. Soy-free. No Artificial
Preservatives.
Precaution: Contains beeswax and carnauba wax.
1 gummy
Calories 10, Total Carbohydrate 2 g, Total Sugars [Includes 1 g Added Sugars] 1
g, Melatonin 2.5 mg.
Other Ingredients: Glucose Syrup, sucrose, gelatin, citric acid, lactic acid,
black carrot juice concentrate, more...
APPROVED
GNC Melatonin 3 mg![]()
![]()

Dist. by General Nutrition Corporation
1 tablet
3 mg
✔
✔
As a dietary supplement, take one tablet before
bedtime.
Medium circular vegetarian tablet
$0.07/vegetarian tablet
[$0.02]
$8.99/120 vegetarian tablets
1 tablet
Vitamin B-6 (as Pyridoxine Hydrochloride) 2 mg
Kosher.
1 tablet
Vitamin B-6 (as Pyridoxine Hydrochloride) 2 mg, Melatonin 3 mg.
Other Ingredients: Dicalcium Phosphate, Cellulose.
APPROVED
GNC Melatonin 5 mg![]()
![]()

Dist. by General Nutrition Corporation
1 tablet
5 mg
✔
✔
As a dietary supplement, take one tablet before
bedtime.
Medium circular vegetarian tablet
$0.17/vegetarian tablet
[$0.03]
$9.99/60 vegetarian tablets
None.
1 tablet
Melatonin 5 mg.
Other Ingredients: Dicalcium Phosphate, Cellulose.
APPROVED
Life Extension® Melatonin 3 mg![]()
![]()

Dist. by Quality Supplements and Vitamins, Inc.
1 capsule
3 mg
✔
NA
Take one (1) capsule 30 to 60 minutes before
bedtime, or as recommended by a healthcare practitioner.
Medium/large vegetarian capsule
$0.10/vegetarian capsule
[$0.03]
$6.00/60 vegetarian capsules
Non-GMO.
1 capsule
Melatonin 3 mg.
Other Ingredients: Microcrystalline cellulose, vegetable cellulose (capsule),
rice concentrate.
APPROVED
Natrol® Melatonin 5 mg
![]()

Mfd. by Natrol LLC
1 tablet
5 mg
✔
NA
Take 1 tablet 20 minutes before bedtime.
Medium fast-dissolve tablet
$0.13/fast-dissolve tablet
[$0.03]
$11.79/90 fast-dissolve tablet
Vegetarian. No: Milk, Egg, Fish, Crustacean
Shellfish, Tree Nuts, Peanuts, Yeast, Artificial Colors, Flavors or
Preservatives.
Precaution: Contains: Wheat, Soy.
1 tablet
Melatonin 5 mg.
Other Ingredients: Xylitol, Cellulose Gum, Soy Polysaccharides, Maltodextrin,
Dextrose, Crospovidone, more...
APPROVED
Nature Made® Melatonin Gummies 2.5 mg - Dreamy
Strawberry
![]()

Dist. by Nature Made Nutritional Products
1 gummy
2.5 mg
✔
NA
Adults, chew 1 gummy one hour before bedtime.
Medium/large gumdrop-shaped gummy
$0.22/gummy
[$0.09]
$17.49/80 gummies
No Artificial Flavors - Natural Fruit Flavors.
No Synthetic Dyes - Color Derived from Natural Source. No High Fructose Corn
Syrup. No Artificial Sweeteners. Gluten Free.
1 gummy
Calories 10, Total Carbohydrate 2 g, Total Sugars [Includes 1 g Added Sugars] 1
g, Melatonin 2.5 mg.
Other Ingredients: Glucose Syrup, Sugar, Water, Gelatin, Citric Acid, Malic
Acid, Palm Oil, more...
APPROVED
Top Pick
for Liquid
NOW® Liquid Melatonin
![]()

Mfd. by Now Foods
1/4 tsp [0.9 ml]
3 mg
✔
NA
Take 1/4 teaspoon (~20 drops) just prior to
bedtime.
Liquid from bottle
$0.08/1/4 tsp
[$0.03]
$5.42/2 fl oz [59 ml] bottle (approx. 66 servings)
Not manufactured with wheat, gluten, soy, milk,
egg, fish or shellfish ingredients.
1/4 tsp
Melatonin 3 mg.
Other Ingredients: Water, Vegetable Glycerin, Fructose, Xylitol, Organic Cane
Alcohol (6%), Natural Orange Extract (Citrus sinensis), Natural Flavors, more...
APPROVED
Puritan's Pride® Melatonin 2.5 mg - Natural
Strawberry Flavor![]()
![]()

Mfd. by Puritan's Pride, Inc.
1 gummy
2.5 mg
✔
NA
For adults, chew one (1) gummy only at bedtime
as melatonin may produce drowsiness.
Medium/large gumdrop-shaped gummy
$0.12/gummy
[$0.05]
$7.19/60 gummies
No Artificial Flavor, No Artificial Sweetener,
No Preservatives, No Milk, No Lactose, No Soy, No Gluten, No Wheat, No Yeast,
No Fish, Sodium Free.
Precaution: Contains Carnauba Wax.
1 gummy
Calories 10, Total Carbohydrate 2 g, Total Sugars [Includes 1 g Added Sugars] 1
g, Melatonin 2.5 mg.
Other Ingredients: Corn Syrup, Sugar, Gelatin. Contains <2% of: Citric Acid,
Natural Flavor, Pectin, more...
APPROVED
Top Pick
for Vegans - Moderate Dose
Solgar® Melatonin 3 mg![]()
![]()

Mfd. by Solgar, Inc.
1 nugget
3 mg
✔
✔
As a dietary supplement for adults, take one (1)
nugget at bedtime as melatonin may produce drowsiness, or as directed by a
healthcare practitioner.
Small circular nugget
$0.06/nugget
[$0.02]
$7.49/120 nuggets
Kosher. Non-GMO, Free Of: Gluten, Wheat, Dairy,
Soy, Yeast, Sugar, Sodium, Artificial Flavor, Sweetener, Preservatives and
Color. Suitable for vegans.
1 nugget
Melatonin (as N-Acetyl-5-Methoxy-tryptamine) 3 mg.
Other Ingredients: Microcrystalline Cellulose, Vegetable Cellulose, Silica,
Vegetable Stearic Acid, Vegetable Magnesium Stearate.
APPROVED
Spring Valley™ [Walmart] Melatonin 5 mg -
Artificial Strawberry Flavor
![]()

Dist. by Wal-Mart Stores, Inc.
1 tablet
5 mg
✔
NA
Adults, take 1 tablet 20 minutes before bedtime.
For best results, allow a tablet to dissolve in mouth before swallowing.
Medium circular fast-dissolve tablet
$0.05/fast-dissolve tablet
[$0.01]
$5.94/120 fast-dissolve tablet
100% Vegetarian. No Gluten, Wheat, Milk, Eggs,
Fish, Crustacean Shellfish, Tree Nuts, Peanuts, Soybeans, Yeast, Artificial
Colors or Preservatives.
1 tablet
Melatonin 5 mg.
Other Ingredients: Dextrose, Microcrystalline Cellulose, Cellulose Gum,
Crospovidone, Maltodextrin, Glyceryl Behenate, Sucrose Esters of Fatty Acids,
Gum Acacia, Beet Root Extract, more...
APPROVED
Top Pick
for Moderate Dose - 3 mg
Trader Joe's® Chewable Melatonin 3 mg -
Peppermint Flavor
![]()

Dist. by Trader Joe's
1 tablet
3 mg
✔
NA
Take one (1) tablet daily, preferably 30 to 60
minutes before bedtime, or as directed by a health professional.
Medium chewable tablet
$0.04/chewable tablet
[$0.01]
$3.99/100 chewable tablets
Precaution: Contains Milk.
1 tablet
Melatonin 3 mg.
Other Ingredients: Lactose (Milk), Microcrystalline Cellulose, Natural
Peppermint Flavor, Croscarmellose Sodium, Magnesium Stearate (Vegetable
Source).
APPROVED
USANA® Pure Rest™![]()
![]()

Mfd. by USANA
1 tablet
2 mg
✔
NA
Adults take 1/2 to 2 dissolvable tablets as
needed one hour before bedtime for relief of occasional sleeplessness.
Medium dissolvable tablet
$0.41 / dissolvable tablet
[$0.20]
$22.88/56 dissolvable tablets
None.
1 tablet
Melatonin 2 mg.
Other Ingredients: Xylitol, Natural Orange Flavor, Ascorbyl Palmitate, Silicon
Dioxide.
Moderate Dose Timed-Release: 2 mg
to 5 mg:
APPROVED
CVS Health® Melatonin 5 mg
![]()

Dist. by CVS Pharmacy, Inc.
1 timed-release tablet
5 mg
✔
NA
For adults, take one (1) tablet at bedtime as
melatonin may produce drowsiness.
Medium circular tablet
$0.11/tablet
[$0.02]
$9.79/90 tablets
1 tablet
Vitamin B-6 (as Pyridoxine HCl) 10 mg, Calcium (as Dicalcium Phosphate) 80.5 mg
Timed release. No yeast, wheat, gluten, milk or milk derivatives, lactose,
sugar, preservatives, soy, artificial color, artificial flavor, salt.
1 tablet
Vitamin B-6 (as Pyridoxine HCl) 10 mg, Calcium (as Dicalcium Phosphate) 80.5
mg, Melatonin 5 mg.
Other Ingredients: Vegetable Magnesium Stearate, Stearic Acid and Silica.
APPROVED
Top Pick
for Moderate Dose Timed-Release
REMfresh® Advanced Ion-Powered Melatonin™
![]()
Dist. by Physician's Seal®, LLC
1 caplet
5 mg
✔
✔
Take 1 caplet 30 to 90 minutes before intended
bedtime. For extra support, take 2 caplets nightly.
Medium caplet
$0.92/caplet
[$0.18]
$32.99/36 caplets
7 Hour Absorption.
1 caplet
Melatonin (UltraMel®) 5 mg.
Other Ingredients: Silicified Microcrystalline Cellulose, Citric Acid,
Hydroxypropyl Methylcellulose, Starch, Talc. Less than 2% of: FD&C Blue #1
Lake, more...
APPROVED
Source Naturals® Melatonin
![]()

Dist. by Source Naturals, Inc.
1 timed-release tablet
3 mg
✔
NA
1 tablet approximately 30 to 60 minutes before
bedtime.
Medium circular tablet
$0.09/tablet
[$0.03]
$21.12/240 tablets
1 tablet
Calcium (as dibasic calcium phosphate) 31 mg
Non-GMO. Timed Release.
1 tablet
Calcium (as dibasic calcium phosphate) 31 mg, Melatonin 3 mg.
Other Ingredients: Dibasic calcium phosphate, microcrystalline cellulose,
cellulose acetate, stearic acid, magnesium stearate, and silica.
High Dose: 10 mg:
APPROVED
Top Pick
for High Dose - 10 mg
Nature's Bounty® Melatonin 10 mg![]()
![]()

Mfd. by Nature's Bounty, Inc.
1 capsule
10 mg
✔
NA
For adults, take one (1) capsule at bedtime as
melatonin may produce drowsiness.
Large capsule
$0.17/capsule
[$0.02]
$10.23/60 capsules
Non-GMO. No Artificial Color, No Artificial
Flavor, No Artificial Sweetener, No Preservatives, No Sugar, No Starch, No
Milk, No Lactose, No Soy, No Gluten, No Wheat, No Yeast, No Fish, Sodium Free.
1 capsule
Melatonin 10 mg.
Other Ingredients: Vegetable Cellulose, Gelatin, Silica, Vegetable Magnesium
Stearate.
Pet Products:
APPROVED
Top Pick
for Pets
K9 Choice Melatonin - Peanut Butter Flavored
Tabs
![]()

Dist. by Products Development, LLC
1 tablet
3 mg
✔
NA
One (1) tablet for dogs under 30 lbs. every 12
hours. Two (2) tablets for dogs over 30 lbs. every 12 hours.
Medium circular chewable tablet
$0.11/chewable tablet
[$0.04]
$12.99/120 chewable tablets
Precaution: Contains: Wheat.
1 tablet
Melatonin 3 mg.
Other Ingredients: Brewer's Yeast Powder, Dicalcium Phosphate, Stearic Acid,
Magnesium Stearate, Microcrystalline Cellulose, Natural Flavor, Silicon
Dioxide.
APPROVED
Mac + Maya™ Calming Aid With Melatonin![]()
![]()

Dist. by The Nature's Bounty Co.
1 soft chew
0.06 mg
✔
NA
Also tested for heavy metalsⓘ
✔
For use in dogs only over the age of 12 weeks.
Up to 27 lbs.: 1 soft chew. 27 to 50 lbs.: 2 soft chews. 51 to 99 lbs.: 4 soft
chews. 100 lbs. and over: 6 soft chews.
Medium/large cube-shaped soft chew
$0.32/soft chew
[$5.35]
$22.49/70 soft chews
1 soft chew
Chamomile 75 mg, Passion Flower 50 mg, Ginger 50 mg, Thiamine Mononitrate 45
mg, L-Tryptophan 15 mg.
No artificial flavors or colors
1 soft chew
Chamomile 75 mg, Passion Flower 50 mg, Ginger 50 mg, Thiamine Mononitrate 45
mg, L-Tryptophan 15 mg, Melatonin 60 mcg.
Inactive Ingredients: Brewers Dried Yeast, Canola Oil, more...
Unless otherwise noted, information about the
products listed above is based on the samples purchased by ConsumerLab.com (CL)
for this Product Review. Manufacturers may change ingredients and label
information at any time, so be sure to check labels carefully when evaluating
the products you use or buy. If a product's ingredients differ from what is
listed above, it may not necessarily be of the same quality as what was tested.
The information contained in this report is
based on the compilation and review of information from product labeling and
analytic testing. CL applies what it believes to be the most appropriate
testing methods and standards. The information in this report does not reflect
the opinion or recommendation of CL, its officers or employees. CL cannot assure
the accuracy of information.
Copyright ConsumerLab.com, LLC, 2021 All
rights reserved. Not to be reproduced, excerpted, or cited in any fashion
without the express written permission of ConsumerLab.com LLC
ConsumerTips™:
Most melatonin
supplements are synthetically manufactured but chemically identical to the
melatonin produced in the body. Supplements are required to list their source
of melatonin if made directly from plant or animal sources. If the source is
not given, it is assumed to be synthetic. Consequently, supplements that
promote being made of "vegetarian" or "non-animal"
melatonin but don't list the specific source are likely to be synthetic
melatonin.
Herbatonin, a branded melatonin supplement tested in this review, is
promoted as "phyto-melatonin," or plant-based melatonin.
It contains a 100:1 extract of rice, alfalfa and chlorella, which contain
modest amounts of melatonin (Meng, Nutrients 2017).
Melatonin extracted
from animal glands carries a concern for potential infection with the
prion that causes Mad Cow Disease (bovine spongiform encephalopathy) and
variant Creutzfeldt-Jakob disease in humans. Transmission of this disease from
supplements, however, has not been documented.
The full chemical name
for melatonin is "N-acetyl-5-methoxytryptamine." Some products state
"5-methoxy-tryptamine" while others just state "melatonin"
— all three are synonymous.
The labeled amount of melatonin
in products can range significantly, for example, from just 0.3 milligrams to
10 milligrams per pill, and suggested daily dosages may vary even more.
Purchase a product that will conveniently provide the appropriate dose for the
intended use (see Dosage information below).
Melatonin is available in
a variety of forms -- liquids and lozenges, regular tablets, capsules, and
softgels and special timed-release forms that claim to extend its release over
a period of hours (also referred to as extended-release or controlled-release).
Regular melatonin formulas act fairly quickly, within 30 to 60 minutes, while
timed-release may also help, to some extent, with staying asleep.
If you are trying
melatonin for the first time, start with a very low dose (1 mg or less) and see
if it helps. Liquids may be convenient as they allow you to adjust the amount
you take by small increments based on the number of drops you use. Liquids may
also be preferable for children, as they can be mixed into beverages.
Additional ingredients in melatonin products may include herbs
of a calming reputation, such as valerian -- which may promote sleep (see Product Review of Valerian). Vitamin B6 is added
to some products, presumably because of its role in the synthesis of serotonin,
a melatonin precursor. However, the value of vitamin B6 in such products seems
unclear. Theanine, an amino acid which may reduce stress but also
increase mental alertness, is also added to some products. However, theanine is
typically taken daily (at a dose of about 200 to 400 mg daily) for a period of
weeks, and not on an "as needed" basis like melatonin, so it would
seem advisable to take theanine as a separate supplement and not part of
melatonin product (see our Review of L-Theanine Supplements).
GABA, a neurotransmitter that calms nerves is in some products, but GABA taken
orally does not increase GABA levels in the brain and is not likely to aid
sleep (Boonstra, Front Psychol 2015).
Other ingredients are added for their supposed calming effects, such as lemon
balm, hops, passion flower, and chamomile. When using combination formulas, be
aware of potential side effects and drug interactions associated with each ingredient
(as discussed in the reviews linked above).
Bioavailability
Melatonin is both fat and water soluble, so it can be taken with or without a
meal. Once, absorbed, it first goes to the liver where much of it is broken
down, so that only about 15% of melatonin taken orally makes it into the blood
stream (Di, N Engl J Med 1997; DeMuro, J Clin Pharmacol 2000) although this
can vary significantly from person to person (Andersen, BMC Pharmacol Toxicol 2016).
Theoretically, melatonin absorbed directly through blood vessels in the mouth
(such as from a patch worn on the inner cheek) would bypass the liver, but
there does not appear to be published research showing better bioavailability
with this approach versus melatonin that is swallowed (Zetner, Drug Res (Stuttg) 2016).
In short, melatonin gets absorbed through the gut and there is no good reason
at this time to believe that one formulation is better than another for
maximizing bioavailability.
Timed release formulation will not increase bioavailability but can sustain
blood levels of melatonin for a longer period of time.
What to Consider When Using:
How and when to take: As noted above, melatonin can be taken with
or without food. For regular tablets, caplets, and capsules, take melatonin
about 30 — 60 minutes before you want to go to sleep (except when using for
specific conditions noted below, such as delayed sleep patterns, that require
different timing). Liquids and fast-dissolving tablets can be taken about 20
minutes before you want to go sleep. Gummies, as long as well chewed, can also
be taken about 20 minutes before you want to go sleep, but keep in mind that
these are sticky and typically contain some sugar, so teeth should be
well-brushed after use and before going to bed.
Dosage: Below are dosages that
have been used in clinical trials. However, as melatonin is a hormone, you may
want to try lower amounts. For some people, as little as 0.5 mg may be
sufficient to aid sleep onset. In fact, doses as low as 0.1 to 0.3 mg of
melatonin have been shown to increase blood concentrations into the range
normally found at night in young adults. Doses that have been used in clinical
studies for insomnia in children (1 to 5 mg daily) can achieve melatonin levels
that are five to 25 times higher than the range normally found
at night, and the long-term safety of this is unknown (Abramowicz, JAMA 2020). (Remember: 1 mg =
1,000 mcg)
·
To aid in falling asleep: Typically, a dose of 2-3 mg of
melatonin is taken 30 to 60 minutes before bedtime, although recommendations
vary from 0.5 mg to 5 mg. This dose should be taken for four days following
travel to counter insomnia after a long flight. A sustained release form in a
dosage of 3 mg may also be combined with an immediate release form at a dosage
of 2-3 mg. Dosages less than 2 mg may not be effective for some adults.
·
To treat insomnia in children with chronic sleep onset insomnia:
1 to 3 mg at 6 PM daily have been used, although doses as low as 0.1 to 0.3 mg
of melatonin can increase blood concentrations into the range normally found at
night in young adults (Abramowicz, JAMA 2020), and it may be safer to
try lower doses first.
·
To treat insomnia in children with developmental disorders: 5 mg
at 8 PM daily. Again, as noted directly above, it may be safer to try lower
doses first.
·
To prevent cluster headache: 10 mg before bedtime daily.
·
As an adjunct in cancer chemotherapy: 10 to 50 mg daily has been
used prior to and during therapy.
·
To reduce tardive dyskinesia: 10 mg daily of time-release form.
·
For irritable bowel syndrome: 3 mg at bedtime daily.
·
For sleep difficulties associated with use of beta block
medications, 2.5 mg melatonin one hour before bedtime (note: melatonin may
increase blood pressure when taken with certain other blood pressure lowering
medications, see Concerns and Cautions).
·
For delayed weekend sleep pattern: 6 mg five hours before the
desired Sunday bedtime.
Use with prescription sedatives and sleep medications
There is mixed evidence on whether or not melatonin is helpful to people taking
prescription sedatives or sleep medications. A study among 34 men and women
(average age 68) who had been taking a daily dose of between 0.5 mg and 2 mg of
benzodiazepine medications such as lorazepam (Ativan) or alprazolam (Xanax) for
at least six months to treat insomnia found that a greater number of
participants who took melatonin were able to discontinue use of their
benzodiazepine medication after six weeks compared to placebo (Garfinkle, JAMA 1999).
On the other hand, another study among older adults (average age 70) with insomnia
who were taking similar doses of benzodiazepines found that melatonin did not
improve sleep or help to reduce benzodiazepine dosage (Cardinali, Neuro Endocrinol Lett 2002). Due to
the potential for increased sedation and side-effects, it is best to consult
with your physician about using melatonin along with prescription sleep
medications (see Concerns and Cautions below).
Melatonin supplements and natural production of
melatonin
Taking small to moderate doses of melatonin does not appear decrease the body's
own production of melatonin (endogenous melatonin). This was demonstrated in a
small, placebo-controlled study among adults who took 0.5 mg of melatonin every
evening for seven days (Matsumoto, J Pineal Res 1997).
Furthermore, a study in Israel found that daily supplementation with 2 mg of
prolonged-release melatonin for 6 to 12 months did not cause
"rebound" insomnia or symptoms of withdrawal when stopped, and, two
weeks after stopping, endogenous melatonin levels (as measured by a melatonin
metabolite in urine) were within normal ranges (Lemoine, Ther Clin Risk Manag 2011).
Factors that may decrease endogenous melatonin levels include
exposure to light at night (Gooley, J Clin Endocrinol Metab 2011) and
certain medications, such as the benzodiazepine drug diazepam (Valium) (Djeridane, Psychopharmacology
(Berl) 2001). Drinking caffeinated coffee in the afternoon or
evening may decrease melatonin levels (Shilo, Sleep Med 2002), although,
interestingly, taking melatonin along with caffeine may increase blood levels
of melatonin (Hartter, Br J Clin Pharmacol 2003).
A study among older people in Japan with cataracts (clouded
lenses of the eye) found that having the cataracts removed (and replaced
with clear intraocular lenses) significantly increased natural
melatonin production three months after surgery as compared to people who did
not have cataracts removed. The researchers hypothesized that cataract removal
and use of clear lenses allowed for greater nonvisual light perception and
improved circadian alignment, increasing melatonin secretion. A non-significant
increase in melatonin production occurred when yellow intraocular
lenses were used. Yellow lenses block blue light, which may reduce nonvisual
light perception, and they are used, theoretically, to protect the retina
against age-related macular degeneration, although this benefit has not been
proven (Nishi, JAMA Opthal 2020).
Are nuts a good source of melatonin?
Nuts contain extremely small amounts of melatonin. Pistachios contain some of
the highest concentrations of melatonin among raw nuts, but this is just
0.00001 mg of melatonin per gram (about 4 nuts) (Verde, J Food Compost Anal 2021). A study from
Iran published in 2014 suggested that pistachios from that country contained
much higher amounts of melatonin (0.23 mg per gram) (Oladi,
Spectrochim Acta A Mol Biomol Spectrosc 2014), but the unusual
extraction method used in the study and near identical results across four
types of pistachio raised questions about the comparability and reliability of
the pistachio findings (Nawaz, Front Plant Sci 2016). Chestnuts,
almonds and pine nuts contain slightly higher concentrations of melatonin than
pistachios, but these are still minute amounts. Other nuts (such as Brazil
nuts, cashews, hazelnuts, and peanuts) contain much lower concentrations.
Roasting significantly decreased melatonin concentrations in all of these nuts
with the exception of peanuts, in which melatonin concentrations appear to
increase with roasting, but remained minute.
Concerns and Cautions:
While
it has been found to be generally safe, at least in short-term uses, melatonin
is a hormone and, like any hormone, could potentially have wide-ranging effects
in the body, as noted below.
·
A review of clinical studies of melatonin found the most
commonly reported adverse effects to be drowsiness (20.3%), headache (7.8%), dizziness (4.0%)
and nausea (1.5% incidence) (Buscemi, AHRQ 2004). Occasionally, other
gastrointestinal effects such as mild abdominal pain, cramps and
diarrhea have been reported (Van der Heijden, J Am Acad Child Adolesc Psychiatry 2007; Papavasiliou, JAMA 1972). There is one report
of melatonin triggering symptoms of active Crohn's disease (abdominal
cramps and diarrhea) in a 35-year-old woman with Crohn's disease who took 3 mg
of melatonin for four days; the symptoms resolved within one day of stopping
supplementation (Calvo, J Pineal Res 2002).
·
Although not all studies have found a problem (particularly with
younger adults), drowsiness and impaired balance may occur for up to
six hours after taking and you should not drive or operate heavy machinery
during that time. A study among men and women ages 60 to 71 in China found
that, compared to placebo, a single, 3 mg dose of melatonin significantly
impaired balance one hour after taking, although it did not negatively affect
cognitive function (Lui, J Aging Phys Act 2018).
·
There does not appear to be a "hangover"
effect the day after using regular-release products. A
long-term, placebo-controlled study in postmenopausal women found no increase
in adverse events or daytime drowsiness, nor reductions in muscle strength or
balance, at daily doses of 1 mg and 3 mg administered at bedtime the day before
(Amstrup, Nutrition J 2015).
However, higher-dose, controlled-release products may cause
next-day drowsiness due to the longer time that melatonin remains in the
system. This is suggested by a study among older adults that found that a 4 mg
product (3 mg controlled-release + 1 mg immediate-release) resulted in high
blood levels of melatonin for an average of 10 hours, while a 0.4 mg product (0.3
mg controlled-release and 0.1 mg immediate-release), resulted in high blood
levels for only 6.4 hours (Gooneratne, J Pineal Res 2012 -- Note:
ConsumerLab.com was retained by the researchers to test the dissolution of both
products. The study was funded by the National Institutes of Health).
·
Taking melatonin may increase leg movements in restless
legs syndrome (RLS). A small study in people with severe RLS found
significantly more leg movement when measured about one hour and four and a
half hours after consuming 3 mg of melatonin in the evening than when no
melatonin was taken. However, patients did not report any increase in
discomfort (Whittom Sleep Med 2010).
The body's own secretion of melatonin in the evening has also been associated
increased discomfort and leg movements in people with RLS; some researchers
theorize this may be due to melatonin's inhibition of the neurotransmitter
dopamine, which may play a role in RLS (Guo, Front Aging Neurosci 2017). In contrast,
there is preliminary evidence that melatonin may be helpful in a less common
condition known as periodic limb movement disorder (PLMD), which
involves involuntary leg movements while sleeping, while RLS occurs when a
person is awake (Aurora, Sleep 2012).
·
Although some research has linked use of sleeping
pills (any type) with increased risk of Alzheimer's disease (Leng, Alzheimers Dement 2019; Vernon, Alzheimers Dement 2019),
the results do not prove a cause-and-effect relationship and there is no
evidence that taking melatonin, specifically, increases the risk of Alzheimer's
disease. However,
people who use sedating drugs such as the benzodiazepines lorazepam (Ativan) or
alprazolam (Xanax), or hypnotic drugs such as zolpidem (Ambien, Edular), should
be aware of melatonin's potential to increase sedation and/or
side effects. A small study in adults found that, when taken for two
days with the hypnotic drug zolpidem (Ambien), 2 mg of prescription
prolonged-release melatonin (Circadin) increased zolpidem's effects on
participant's cognitive and driving performance four hours after taking, and
memory recall 12 ½ hours after taking (Otmani, Hum Psychopharmacol 2008). Side
effects have generally not been reported with use of melatonin with
benzodiazepines in short-term studies (Garfinkle, JAMA 1999; Cardinali, Neuro Endocrinol Lett 2002), but
long term studies do not appear to have been conducted.
·
Long-term use of melatonin has been
associated with an increased risk of fractures, suggesting that it
should only be used as needed for limited periods of time. A study of adults
(average age 65) in the United Kingdom found that those prescribed melatonin
were 90% more likely to have suffered a fracture than a matched control group
of people who had not taken melatonin or other sleep aids. Even after adjusting
for variables such as sleep disorders, arthritis, and vision disorders,
melatonin takers were still 44% more likely to have suffered a fracture than
those in the control group. However, only patients who had received three or
more melatonin prescriptions had elevated risk (Frisher, Age and Ageing, 2016). (In the UK
melatonin is only available by prescription [2 mg, extended-release] for
patients aged 55 or over for up to 13 weeks). Risk of fracture was also elevated
among those prescribed hypnotics (e.g., zolpidem), although not as much as with
melatonin.
·
It may not be advisable to use melatonin, at
least at high doses, after suffering a fracture. Although melatonin seems to
increase bone density (see What It Does), it may do so by inhibiting bone
resorption rather than increasing bone formation. Bone resorption is an
essential requirement for adequate remodeling during fracture healing. A study
found that mice given very high daily doses of melatonin had impaired fracture
healing compared to non-treated controls (Histing, J Surg Res 2012).
·
Testosterone and estrogen metabolism may be affected, impairing
sperm function in men. In very high doses (over 75 mg daily), melatonin might
prevent ovulation in women. In women entering menopause,
melatonin may cause a resumption of menstrual flow or spotting. Oral
contraceptives may increase the absorption of melatonin from
supplements in some people (Hilli, J Clin Pharmacol 2008).
·
Melatonin was shown to modestly increase reactive aggression (i.e.,
aggression in response to provocation or threat) in a study among male college
students in China. When given the opportunity to administer high or low
punishments to opponents during a game-type experiment, participants who had
ingested melatonin (5 mg, 1 ½ hours prior) selected the high punishment more
often (57.3% of the time) than those who ingested placebo (41.5% of the time).
The increased aggression was determined not be attributed to factors such as
sleepiness or reduced inhibition (Liu, Psychopharm 2017).
·
Extremely high doses of melatonin (250 mg to 1,200 mg) taken
orally or intravenously in divided doses throughout the day for three days to
one month have been reported to worsen depression and cause
auditory hallucinations and episodes of unprovoked tears, rage, terror in
people with depression and bipolar depression. These high doses have also been
found to cause depression in two people with Huntington's disease who had no
symptoms of depression before supplementation with melatonin (Carman, Am J Psychiatry 1976). The same study
noted a report of an exacerbation of symptoms lasting 18 to 36 hours in people
in remission from schizophrenia, immediately following a dose of
300 mg of melatonin. However, more recent studies among people with depression
using much lower doses of melatonin (0.5 mg to 6 mg daily) for up to 3 1/2
years have not reported a worsening of depression (Hansen, Eur Neuropsychopharmacol
2014). ConsumerLab.com received a report from an individual who
experienced suicidal urges after two weeks of melatonin supplementation (dose
unknown). Overall, research suggests that typical doses (< 10 mg) do not
appear to cause or worsen depression. To be safe, however, if you experience
new or worsening depression after taking melatonin, it may be best to stop
supplementation and consult your physician.
·
Some people report having more vivid dreams when
using melatonin.
·
There is some evidence that melatonin may affect seizure
activity. Although some studies have found melatonin supplementation to
decrease seizures or improve sleep in children (Chen, J Formos Med Assoc 2012),
others have reported an increase in seizure activity in neurologically disabled
children with chronic, severe sleep complaints (Sheldon, Lancet 1998).
Until more is known, consult your physician before taking melatonin if you have
a seizure disorder or take anti-seizure drugs such as phenobarbital, primidone
(Mysoline), valproic acid (Depakene), gabapentin (Neurontin), carbamazepine
(Tegretol), phenytoin (Dilantin).
·
Insulin action may be impaired by melatonin. One study among 21
non-diabetic women who were given 5 mg of melatonin 15 minutes prior to two
different oral glucose tolerance tests (OGTT), one in the morning and one at
night, showed that melatonin impaired glucose tolerance by decreasing insulin
release in the morning and decreasing insulin sensitivity at night (Rubio-Sastre, Sleep 2014). Another study
among 70 people with type 2 diabetes (average age 58) showed that taking 6 mg
of melatonin at bedtime for 8 weeks did not affect fasting blood sugar or HbA1c
compared to placebo, but tended to slightly worsen measures of insulin
resistance and insulin sensitivity, although these differences were not
significant (Farrokhian, Iran J Pharm Res 2019). To be
safe, people with diabetes or who are taking antidiabetes drugs such as
glimepiride (Amaryl), glyburide (DiaBeta, Glynase PresTab, Micronase), insulin,
pioglitazone (Actos), rosiglitazone (Avandia) should use with caution if
considering use of melatonin.
·
People with low blood pressure should be aware
that melatonin has been reported to significantly decrease blood pressure in
healthy people without hypertension (Arangino, Am J Cardiol 1999; Cagnacci Am J Physiol 1998). On the other
hand, melatonin may increase blood pressure in people taking certain
antihypertensive medications. In men and women taking 30 mg or 60 mg of
nifedipine GITS (Procardia XL) each morning, taking 5 mg of immediate-release
melatonin at bedtime increased average systolic and diastolic blood pressure by
6.5 mmHg and 4.9 mmHg, respectively (Lusardi Br J Clin Pharmacol 2000).
·
The SSRI antidepressant fluvoxamine (Luvox) may
significantly increase the amount of melatonin absorbed from supplements, which
could increase the risk of drowsiness and other side effects (Harter, Clin Pharmacol Ther 2000).
·
Consuming caffeine with melatonin supplements
may significantly increase melatonin levels (Harpsoe, Eur J Clin Pharmacol 2015).
·
Melatonin supplements may decrease blood clotting (Wirtz J Pineal Res 2008)
and there have been isolated reports of bleeding in people taking melatonin
along with warfarin. Although reports of bleeding are rare, use with caution if
taking blood-thinning medications such as clopidogrel (Plavix), aspirin,
nonsteroidal anti-inflammatory drugs (NSAIDs) such as diclofenac (Voltaren,
Cataflam), ibuprofen (Advil, Motrin, etc.).
·
Some laboratory and animal studies suggest melatonin may
increase the production of lymphocytes (a type of white blood cell) (Miller, Int J Exp Pathol 2006). Until more is
known, people with lymphoproliferative disorders (LPDs) such
as X-linked lymphoproliferative disease, acute lymphoblastic leukemia, chronic
lymphocytic leukemia, B-cell or T-cell lymphomas, multiple myeloma, or other
LPDs should consult with their physician before taking melatonin.
·
Some of the same contaminants found in L-tryptophan and
associated with cases of eosinophilia myalgia syndrome have
been found in melatonin (Williamson, Chem Res Toxicol 1998).
In addition, melatonin at the fairly high dose of 15 mg per day was found to
amplify the eosinophilia experienced by cancer patients who were receiving
interleukin-2 immunotherapy (Lissoni, J Biol Regul Homeost Agents 1993). However,
there have not been other reports of eosinophilia associated
with melatonin use, and it is important to note that the typical dose of
L-tryptophan is 500 to 4,000 mg daily -- many times the standard dose of
melatonin of about 0.5 to 5 mg.
·
It is theorized, but not proven, that people with autoimmune
diseases such as lupus or rheumatoid arthritis should not take melatonin
supplements and that melatonin could cause potential problems in people with
depression or schizophrenia.
Melatonin's safety in young children, pregnant or nursing women,
or people with severe liver or kidney disease has not been established. A review article (Kennaway, J Paed Child Health 2015) notes
that, although studies with melatonin in children have not reported serious
adverse effects, the studies have not been rigorous enough to determine
long-term safety. The same article points out that melatonin is available only
by prescription many countries. In Australia, for example, a prescription
version of melatonin is approved as short-term treatment of insomnia only in
patients who are aged 55 years and older and is not recommended for use in
children and adolescents due to insufficient safety and efficacy data. Animal
studies using very low doses of injected melatonin have caused reductions in
ovarian and testicular weights and other sexual effects. These doses ranged
from 1 to 185 micrograms per kilogram. A 3 mg dose of melatonin equates to 200
mcg/kg for a 33 lb. child and 60 mcg/kg for a 110 lb. child — doses very
similar, if not larger, than those which caused sexual effects when injected
into animals.
To further assist consumers, ConsumerLab.com licenses its flask-shaped CL Seal
of Approved Quality (see The CL Seal) to manufacturers for use on
labels of products that have passed its testing. ConsumerLab.com will
periodically re-evaluate these products to ensure their compliance with
ConsumerLab.com's standards.
Information on this site
is provided for informational purposes only. It is not an endorsement of any
product nor is it meant to substitute for the advice provided by physicians or
other healthcare professionals. The information contained herein should not be
used for diagnosing or treating a health problem or disease. Consumers should
inform their healthcare providers of the dietary supplements they take.
Latest Clinical Research Updates for Melatonin Supplements
Fracture Risk with Melatonin Supplements?
12/03/2021
This week a newsletter
reader asked if taking 3 mg of melatonin every night for sleep can increase the
risk of fractures. Get the answer and find out why this is a valid concern in
the Concerns and Cautions section of our
Melatonin Supplements. Also see our Top Picks among melatonin supplements.
Does Melatonin Increase Alzheimer’s Risk?
11/18/2021
My doctor said that melatonin may increase the risk of Alzheimer's as
some sleeping pills do. Is this true? See the answer in Concerns and Cautions section of the
Melatonin Supplements Review.
When Melatonin Does or Doesn't Help in Hospitals
11/05/2021
See the latest research
on whether or not melatonin helps people undergoing medical
procedures or when hospitalized. Also learn if melatonin has
been shown to help with other sleep issues. It's all in our Melatonin
Supplements Review, which includes our Top Picks for melatonin.
11/02/2021
Do pistachios or other
nuts contain significant amounts of melatonin? How does roasting affect the
melatonin content in nuts? See what a new study found in the ConsumerTips section of our Melatonin
Supplements Review. Also see our Top Picks among melatonin supplements.
7/13/2021
Can melatonin
supplementation improve sleep, behavior, or mood in children with autism
spectrum disorder? See what a new study found in the What It Does section of the Melatonin
Supplements Review. Also see our Top Picks among melatonin supplements.
Related CL Answers (22)